Article Text

Abstract
Objective To assess the clinical effect of caudate-putaminal transplantation of fetal striatal tissue in Huntington's disease (HD).
Methods We carried out a follow-up study on 10 HD transplanted patients and 16 HD not-transplanted patients. All patients were evaluated with the Unified HD Rating Scale (UHDRS) whose change in motor, cognitive, behavioural and functional capacity total scores were considered as outcome measures. Grafted patients also received morphological and molecular neuroimaging.
Results Patients were followed-up from disease onset for a total of 309.3 person-years (minimum 5.3, median 11.2 years, maximum 21.6 years). UHDRS scores have been available since 2004 (median time of 5.7 years since onset, minimum zero, maximum 17.2 years). Median post-transplantation follow-up was 4.3 years, minimum 2.8, maximum 5.1 years. Adjusted post-transplantation motor score deterioration rate was reduced compared to the pretransplantation period, and to that of not-transplanted patients by 0.9 unit/years (95% CI 0.2 to 1.6). Cognitive score deterioration was reduced of 2.7 unit/years (95% CI 0.1 to 5.3). For grafted patients the 2-year post-transplantation [18F]fluorodeoxyglucose positron emission tomography (PET) showed striatal/cortical metabolic increase compared to the presurgical evaluation; 4-year post-transplantation PET values were slightly decreased, but remained higher than preoperatively. [123I]iodobenzamide single photon emission CT demonstrated an increase in striatal D2-receptor density during postgrafting follow-up.
Conclusions Grafted patients experienced a milder clinical course with less pronounced motor/cognitive decline and associated brain metabolism improvement. Life-time follow-up may ultimately clarify whether transplantation permanently modifies the natural course of the disease, allowing longer sojourn time at less severe clinical stage, and improvement of overall survival.
- Huntington's
- Stereotaxic Surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Human fetal striatal transplantation is being investigated as possible treatment for Huntington's disease (HD),1 with the goal of restoring striatal function impaired by primary degeneration.2 Pilot studies have demonstrated the feasibility and safety of the therapy.3–8 Imaging has shown controversial data on survival and efficacy of the graft,8–10 and long-term pathological studies reported its eventual neuronal degeneration.11 Different graft growth patterns have been described.5 ,6 ,12–14 Even though alloimmunisation has been reported,13–16 and its possible role in graft degeneration has been hypothesised,17 the host/graft immune response is not well understood. Neoplastic/teratogenic transformation of the graft has never been observed, while the occurrence of overgrowth has seldom been reported.18 According to a few long-term follow-up studies, fetal striatal transplantation provided a period of clinical improvement in three out of five patients,9 stability in one out of two,10 while no significant clinical benefit was found in a group of five patients compared with 12 non-grafted patients.8 We report the results of a follow-up study designed to assess disease progression in 10 consecutive HD transplanted patients and 16 HD not-transplanted patients, and discuss how fetal striatal transplantation may affect the disease course.
Patients and methods
The present clinical investigation has been conducted according to the Declaration of Helsinki principles. The study begun in 2004 and it was authorised by the Italian National Health Institute, National Transplantation Centre (upon approval by Health Ministry, Consiglio Superiore di Sanità, Sessione XLV, Sezione II, 21 July and 22 September 2005, and acceptance by the National Bioethics Committee). In particular, items to be fulfilled included: (1) distinct separation between the research team and the institution carrying out the pregnancy interruption, (2) lack of benefits for the transplantation and obstetric teams and (3) request of donor's consent after pregnancy interruption. All patients gave written informed consent prior to being enrolled in the study. All were included in the European HD Network REGISTRY.19
The design is an observational cohort aimed at describing the disease evolution since onset of symptoms and any putative changes after transplantation. The series consisted of 26 HD patients (tables 1 and 2) who were acquainted with the transplantation programme and adhered to the protocol. Ten patients asked to undergo transplantation and were grafted between 2006 and 2008—patients 1, 4, 6, 8 having been partially described.13 ,14 All patients were evaluated with the Unified HD Rating Scale (UHDRS)20—high functional and cognitive scores denote better performance, low behavioural and motor scores denote better performance. Moreover, grafted patients were evaluated according to Core Assessment Program for Intracerebral Transplantation21 and received MRI, [18F]fluorodeoxyglucose ([18F]FDG) positron emission tomography (PET) and, after a 10-day drug wash-out, [123I]iodobenzamide ([123I]IBZM) single photon emission CT (SPECT). Details of imaging techniques are provided in online-only material.
Demographic and clinical characteristics of 10 Huntington's disease patients who underwent human fetal striatal transplantation
Demographic and clinical characteristics of 16 not-transplanted Huntington's disease patients
Transplanted patients underwent bilateral, in two sessions 2–6 months apart, stereotactic intrastriatal grafting. Detailed neurotransplantation protocols are reported in online-only material. For each procedure, both ganglionic eminences were dissected from the floor of the forebrain ventricles of a single legally aborted fetus (9–12.4 weeks, median 10.5 weeks; viability >80%, mean 87.2±4.42; with no or negligible haematopoietic contamination measured as CD45 positive cells, mean 1.4±1.7%). After isolation, tissue was washed with saline solution and cut into small fragments, gently dissociated and resuspended in 500 μL of saline solution. 1.5 T MRI (Symphony Siemens, The Netherlands) using 3-dimensional contrast-enhanced T1 MPRAGE sequence was obtained 1–4 days before each surgery. On the day of intervention, stereotactic CT was used to obtain coordinates after coregistration with the previously acquired MRI. Transplantation was performed under general anaesthesia, in robotic-assisted conditions (NeuroMate Schaerer Mayfield, France). Tissue suspension was transplanted into the caudate head and the precommissural and postcommissural putamen (3–9 tracks, mean 6.6), within 4–6 h after abortion. At the level of each track, a total of 50 μL of grafting suspension was injected, using a needle connected to a Hamilton syringe. For each procedure (table 3) the estimated number of grafted cells ranged from 2.85 to 20 millions (median 5.73 millions). Intravenous antibiotic prophylaxis with cefotaxime (2 g) and teicoplanin (200 mg) daily, started 1 day before surgery and continued for 6 days; a single intravenous dose of fluconazole (400 mg) was administered the day of the intervention. Immunosuppression protocol originally included oral administration of methylprednisolone (40 mg/daily for 3 days after surgery, then tapered and discontinued within 2 weeks), azathioprine (3 mg/kg/daily for 12 months) and cyclosporine A (5 mg/kg/daily for 12 months) starting from the day before the first procedure. A serum taken 19 months after her first implant from Patient 1, and 7 months after immunosuppression was discontinued, eventually showed positive results for anti-HLA (Human Leukocyte Antigen) class I and class II antigens.14 Therefore, we modified the immunosuppression protocol by reintroducing cyclosporine A to sensitised patients sine die. Cyclosporine A serum levels were checked weekly for the first 2 months and bimonthly thereafter.
Details of the transplantation procedure in 10 Huntington's disease patients
Descriptive statistics and standard statistical procedures—Student t test, Fisher's Exact test (α=0.05 two-sided), were used to summarise group characteristics. Main outcomes were the deterioration rate in motor, cognitive, behavioural and functional capacity as measured by UHDRS total scores. Repeated measurements at patient-specific follow-up times were available (see Results and online-only material table S1A). Therefore, we described the individual evolution of each outcome by time since disease onset. Transplantation was considered a time-varying binary variable, and we evaluated if transplantation was associated to a change in the deterioration rate for each outcome. To this purpose, for each outcome separately, we fitted a series of linear mixed models with subject-specific random intercepts.22 For simplicity's sake, we fitted a linear time trend. The transplantation effect was modelled as change-in-slope after grafting, specified by an interaction term. We used baseline measurement of disease burden23 and an interaction term between disease burden and time to take into account any potential regression to the mean effect.24 ,25 Age, gender, education, cytosine-adenine-guanine (CAG) repeats were considered potential confounders. A series of linear mixed models including confounders and testing for interactions were fitted; in this phase, we checked for homogeneity of not-transplanted patients’ time profiles and the pretransplantation time profiles of the transplanted patients. We also fitted linear mixed models to grafted case series only. That analysis is expected to be more sensitive but, being based on fewer subjects, to provide less robust results. Results are expressed as point and interval estimates at 95% CI. On analysing multiple outcomes, we applied the Benjamini–Hochberg procedure to control the false discovery rate at 10%.26 A sensitivity analysis was conducted assessing: (1) non-linearity, (2) goodness-of-fit and outlying/influential observations,27 (3) subject-specific time effects, (4) heterogeneity of fetal striatal transplantation effect among subjects, (5) confounding adjustment and use of propensity score, (6) SEs estimates by bootstrap/jackknife. PET imaging differences between pretransplantation and follow-up normalised values were assessed by the paired t test adjusting for multiplicity. SPECT imaging differences between pretransplantation and follow-up times normalised values were assessed by linear mixed models. The potential effect of the length of follow-up on the SPECT difference from baseline was assessed comparing different models by AIC/BIC.22
Results
Patients were followed-up from disease onset for 309.3 person-years (median 11.2 years, maximum 21.6). No significant differences in demographic and disease-related baseline characteristics emerged between transplanted and not-transplanted patients (tables 1,2 and 4). In particular, homogeneity tests showed: sex p=0.22 (Fisher's Exact test); onset age p=0.12 (Student t test); calendar year of onset p=0.08 (Student t test); years of education p=0.48 (Student t test); CAG repeats p=0.12 (Student t test); affected parent p=0.28 (Fisher's Exact test); symptom at onset p=0.84 (Fisher's Exact test); DB p=0.51 (Student t test); UHDRS functional p=0.36, behavioural p=0.78, cognitive p=0.50, motor p=0.10 (Student t test).
Mean and median of baseline characteristics of Huntington's disease patients at study entry
Grafted patients
Follow-up ranged from 6.8 to 21.6 years (median, 13.0 years) since disease onset. Median post-transplantation follow-up was 4.3 years, minimum 2.8, maximum 5.1 years. In Patient 2, subdural haematomas were surgically evacuated 1 month after each stereotaxy, without neurological consequences. After grafting, no adjunctive symptomatic drugs were introduced to any patient. Patient 1 experienced weight loss, fever, worsening of the chorea and leukopenia related to a left thigh abscess 21 months after transplantation.14 Patients 2 and 7 died of sudden death, respectively, at 16.2 and 10.1 years since disease onset (4.1 years and 3.1 years after grafting), without graft-related events. Patient 3 died of pneumonia at 16.4 years since onset (4.2 years after transplantation). We were not able to perform pathological study on the brain of deceased patients.
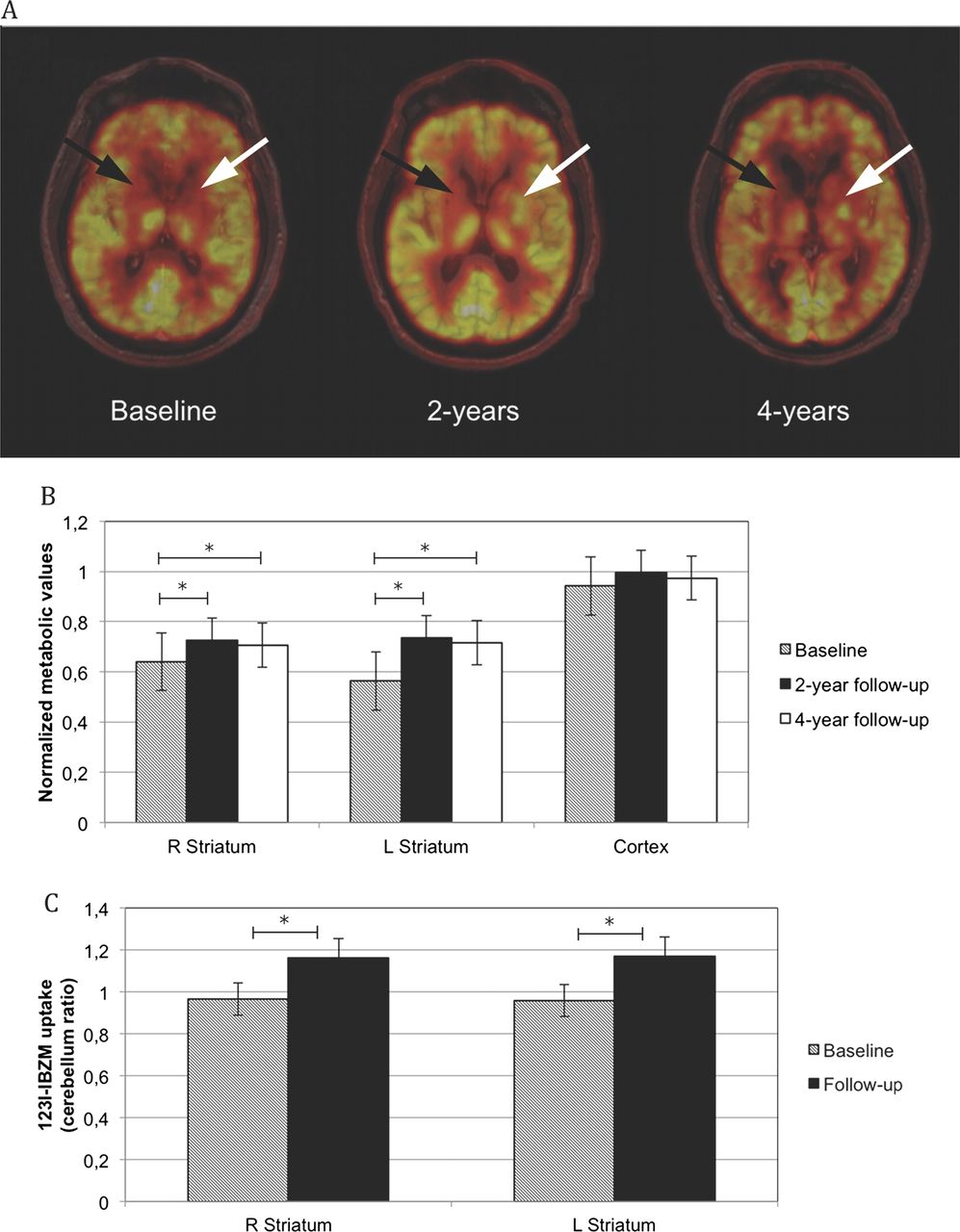
Follow-up times and frequency of morphological and metabolic neuroimaging studies are reported in online-only material table S1B. Preoperative MRI showed striatal/cortical atrophy. The last available MRI (median 4.3 years, maximum 5.1 years), revealed no graft development in one patient, and 3 mm maximum diameter tissue nodules exhibiting moderately hyperintense signal in T2-weighted images in the neostriatum in five patients. Large tissue nodules, exhibiting moderately inhomogeneous hyperintense T2 signal, in the neostriatum (figure 1A), frontal lobe and, in one case also in the ventral striatum, were seen mono/bilaterally in four patients.14 Such large tissue nodules remained unchanged at last follow-up. Pretransplantation PET studies demonstrated severe striatal hypometabolism in all grafted patients, more pronounced in the caudate than in the putamen, associated with moderate cortical hypometabolism (figure 1A). Two years after grafting, [18F]FDG PET showed significant striatal metabolic increase and slight bilateral increment of cortical metabolism, which remained stable up to 4 years (figure 1B). [123I]IBZM SPECT was performed only in patients who tolerated drug washout. Significant striatal D2-receptor binding increase was found (figure 1C). The increase was reached at 12 months and remained stable (best fitting model using AIC/BIC). All patients complied with immunosuppression. Donor-specific anti-HLA antibodies appeared 1.2–3.6 years after the first surgery in five patients, whose immunosuppression regimen with cyclosporine A is continuing up to now.
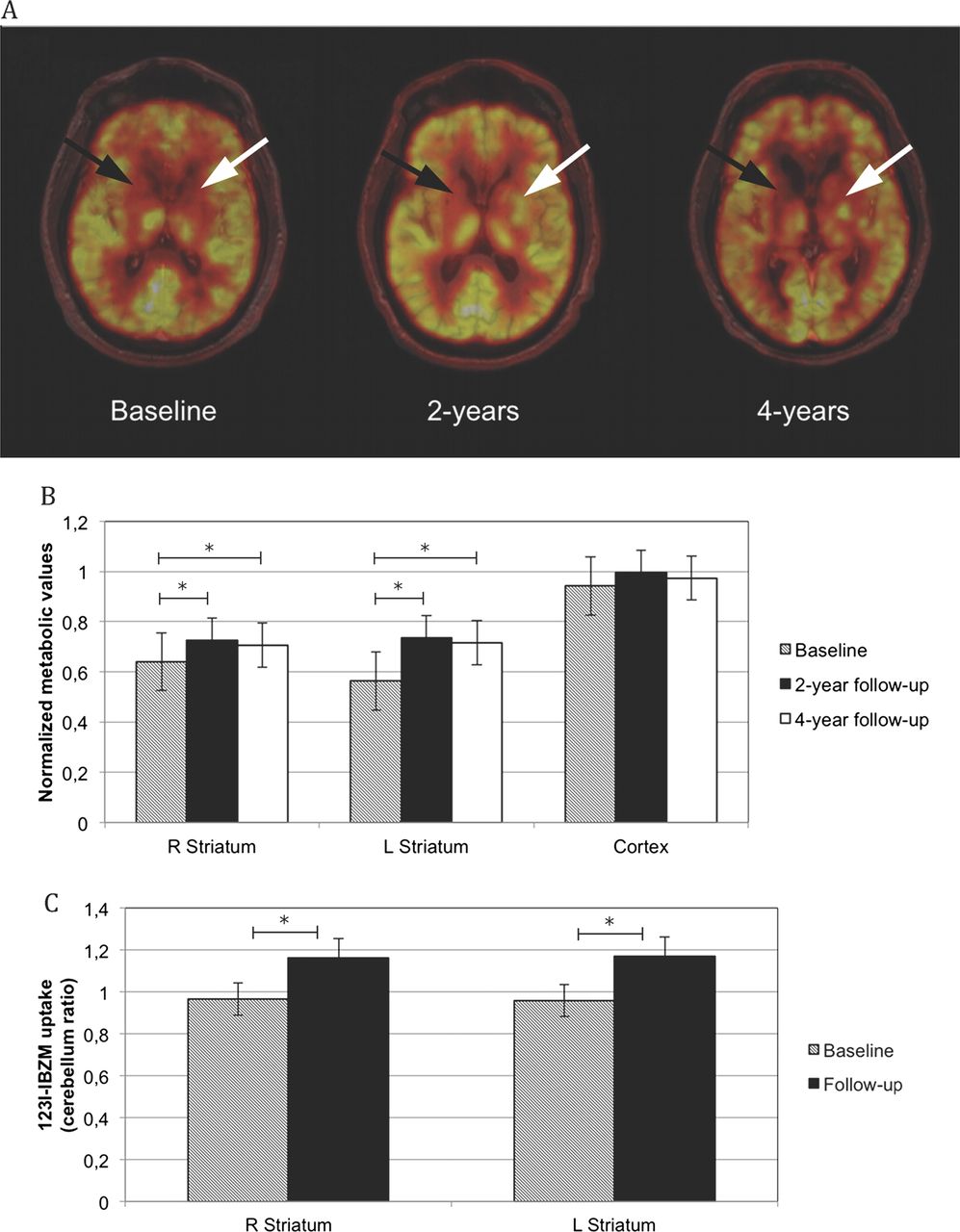
Neuroimaging results in 10 Huntington's disease patients who underwent human fetal striatal transplantation. (A) Co-registered MRI and [18F]fluorodeoxyglucose ([18F]FDG) positron emission tomography (PET) of a representative case (Patient 4). Baseline [18F]FDG PET shows severe striatal hypometabolism (arrows), with moderate cortical hypometabolism. Two-year [18F]FDG PET demonstrates metabolic stability of right striatum (black arrow) and in the cortex, and metabolic increment in left striatum (white arrow), associated with graft growth in the same region. At 4 years after grafting, [18F]FDG PET shows a slight reduction of right striatal (black arrow) and cortical metabolism, and stability of left striatal metabolism (white arrow), compared to baseline and 2-year follow-up. (B) Metabolic activity in striatal and cortical regions measured by [18F]FDG PET: follow-up vs baseline means and SDs, Bonferroni p values. At 2 years after transplantation (10 patients) right striatum: 0.72±0.12 vs 0.64±0.09, *p=0.018; left striatum: 0.74±0.17 vs 0.56±0.14, *p=0.010; cortex 0.99±0.14 vs 0.94±0.13, *p=0.058. At 4 years after grafting (7 patients) right striatum: 0.71±0.08, *p=0.026; left striatum: 0.72±0.17, *p=0.034; cortex 0.98±0.15, p=0.220. (C) Preoperative and postoperative striatal D2-receptor binding measured by [123I]iodobenzamide ([123I]IBZM) single photon emission CT (SPECT) in five patients (ID 2, 3, 4, 7, 8) at baseline, three patients (ID 3, 4, 7) at 12 months, one patient (ID 8) at 18 months, one patient (ID 2) at 24 months after transplantation. Patient identifier (ID) as in Table 1. Postoperative versus preoperative SPECT showed a significant increase in striatal D2-receptor binding. R: right (*p=0.024) and L: left (*p<0.001).
Not-transplanted patients
Follow-up ranged from 5.3 to 20.6 years (median, 10.2 years) since disease onset. Patient 26 experienced sudden death 19.0 years after disease onset; patients 14 and 17 died of pneumonia 18.6 and 14.0 years, respectively, since disease onset. Six patients have experienced one or more psychotic episodes since enrolment in the study. The incidence of psychotic events was higher in not-transplanted than in transplanted patients (6/16 vs 0/10; Fisher's Exact test p=0.053).
UHDRS results
Scores have been routinely available since 2004, at a median time of 5.7 years since disease onset, for 113.2 follow-up person-years. On the whole, 202 tests were administered. Transplanted and not-transplanted patients were evaluated 11–21 and 3–6 times, respectively (see also online-only material table S1A). Linear mixed models, taking into account the longitudinal features of the data with repeated measurements per subject, adjusting for the effect of baseline disease burden on the rate of progression of the disease to control for regression to mean effect, were fitted (table 5, figure 2, online-only material tables S2A–C). Fetal striatal transplantation effect is expressed by comparing the slope (disease progression over time) before and after transplantation (change-in-slope Δslope) and, as secondary outcome, measuring the immediate change at transplantation (change-in-intercept Δintercept). Remember that the slope is the change in each outcome per 1-year increase since disease onset, and represents the disease progression over time. The sign of the coefficient depends on the outcome actually measured, with higher total motor scores and total behavioural scores being worse, and lower total cognitive scores and total functional scores being worse. The change-in-slope is the difference between the slope before and after transplantation. Table 5, left panel, reports regressions on the whole set of enrolled patients’ measurements; in table 5, right panel, regressions are restricted only to measurements of patients who underwent transplantation (online-only material tables S2A–C). The analysis strategy assumes that the disease history of not-transplanted patients did not differ from the disease history of transplanted patients if not transplanted: indeed, we tested an interaction term on all fitted models, and this resulted not statistically significant. However, by comparing the left and right panels, we can judge the stability of the results. We found an adjusted decrease in motor performance of 5.2 units/year (95% CI 3.9 to 6.5) in the whole patients’ series and of 6.7 units/year (95% CI 5.1 to 8.3) among grafted patients only. Transplantation had an immediate positive effect, that is, with an estimated change-in-intercept of −2.3 units (95% CI −5.8 to 1.2) in the whole patients’ series and −6.8 units (95% CI −10.6 to −3.0) among grafted patients (table 5). Transplantation also had a long-lasting positive effect over a 4-year postoperative period, slowing the rate (change-in-slope) by −0.9 units/year (95% CI −1.6 to −0.2) in the whole series, and −2.0 units/year (95% CI −2.8 to 1.2) among grafted patients. The rate of deterioration of total motor scores was contrasted by transplantation, with an immediate improvement in performance shortly after grafting and a reduction of the rate of change (figure 3). The transplantation effect was present, but with wider CI, for total cognitive scores, and scarcely evident for total behavioural and functional scores. Figure 2A reports regression analysis results for each item of motor UHDRS (see online-only material table S2B). Chorea and ocular movements mostly benefited from transplantation. Figure 2B (see online-only material table S2C) reports results for each item of cognitive UHDRS. All cognitive items were positively affected by transplantation in the grafted patients’ series. Using the total HD patients’ series, only symbol digit combination was improved. Alternative models were explored in the sensitivity analysis (see online-only material), but our results appeared robust and no major differences were found under alternative modelling.
Human fetal striatal transplantation effect on Unified Huntington's Disease (HD) Rating Scale (UHDRS) total scores
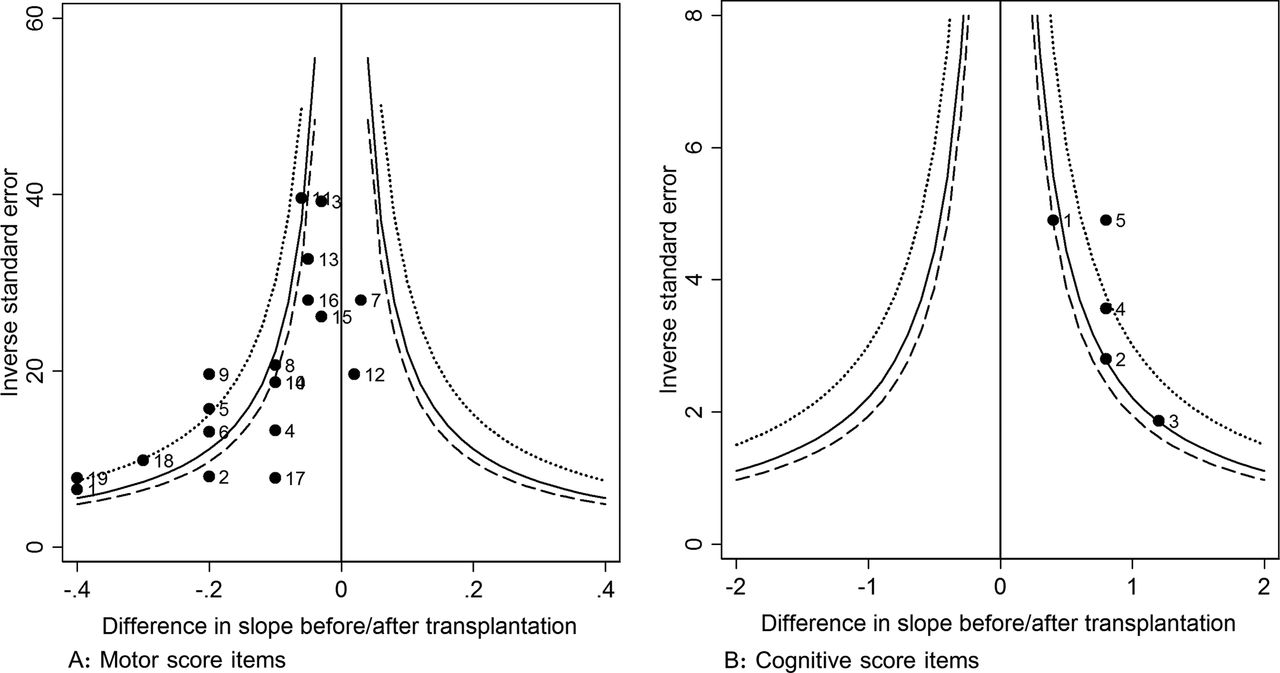
Human fetal striatal transplantation effect on the motor and cognitive items of the Unified Huntington's Disease Rating Scale scores. Funnel plot of effect estimates (Δslope: difference in slope before/after transplantation) for motor (A) and cognitive (B) items with thresholding lines (dot: Bonferroni p value; solid: false discovery rate <0.05; dashed: false discovery rate <0.10). A point labels: 1 chorea, 2 dystonia, 3 gait, 4 ocular pursuit, 5 saccade initiation, 6 saccade velocity, 7 dysarthria, 8 tongue protrusion, 9 finger taps, 10 pronate/supinate hands, 11 Luria, 12 rigidity, 13 bradykinesia, 14 tandem walk, 15 retropulsion, 16 dystonia axial, 17 dystonia articular, 18 chorea axial, 19 chorea limbs. B point labels: 1 phonemic verbal fluency, 2 Stroop reading fluency, 3 Stroop colour naming, 4 Stroop interference, 5 symbol digit combination.
{kind=link}
{kind=link}
{kind=link}
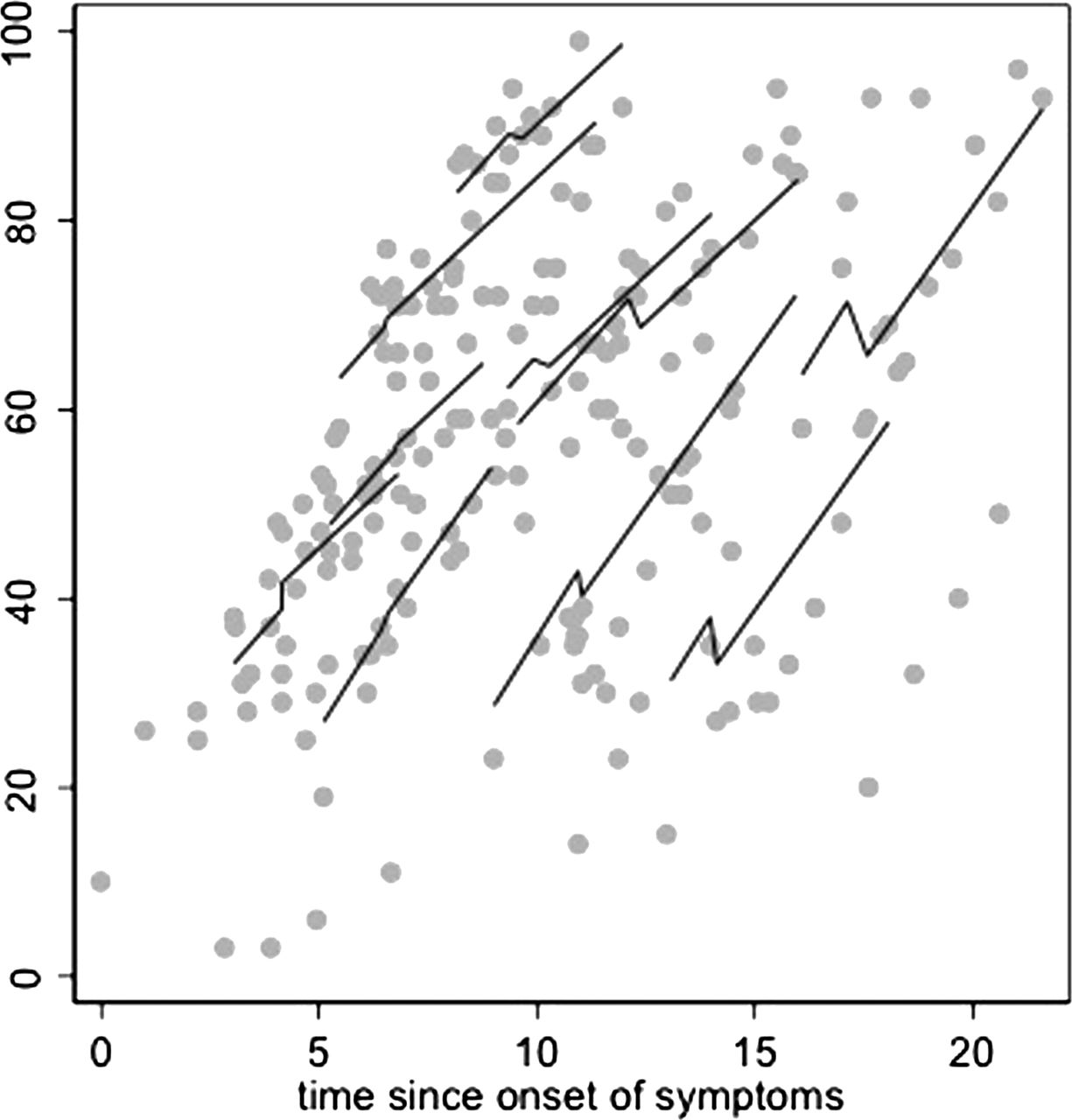
Unified Huntington's Disease Rating Scale total motor scores deterioration in Huntington's disease patients. Scatter plot of 202 measurements on 26 patients and fitted patient-specific pre and post- transplantation regression lines of 10 grafted patients. Total motor scores (y-axis, better down) over time since onset of symptoms (x-axis, in years).
To appreciate the clinical relevance of our findings, we calculated the impact of fetal striatal transplantation in terms of time gained in less severe condition. The transplantation effect was to reduce the rate of progression from 5.2 to 5.2−0.9=4.3 scores per year. In other words, to worse by 30 units the total motor score, transplanted patients need 7.0 years instead of 5.8, about 1 year and half gained in better health. Table 6 reports these calculations using the average deterioration observed among not-transplanted patients for each main UHDRS, that is, the estimated deterioration time, and the estimated transplantation impact in terms of time the patient has spent in a less invalidating condition.
Clinical impact of human fetal striatal transplantation in Huntington's disease
Discussion
Neurotransplantation has been explored since the 1990s as a possible therapy for HD.1 Ethical issues have been raised when fetal tissues are collected as a graft source.29 Indeed, neurotransplantation remains highly experimental, and clinical trials are lacking. Previous fetal striatal transplantation studies have been carried out in a few patients.1 Kopyov et al3 reported three transplanted subjects showing slight improvement of motor and cognitive functions at 12-month follow-up. Hauser et al5 described no significant changes in motor and functional scores at 12 months in seven patients. Transplantation provided a period of motor and cognitive improvement in three patients of Bachoud-Lévi et al9 series at 6 years, and in one patient of Reuter et al10 series over 5 years. Recently, Barker et al8 reported no significant clinical benefit of cell transplantation in neurological, neuropsychological and imaging assessment of five patients followed up to 10 years. Overall, an effect of transplantation remained questionable.
Our study provides evidence that transplantation is associated with slower motor and cognitive deterioration in HD. However, our findings should be interpreted with caution. The main drawback of non-randomised studies is the potential unbalance between treatment and control condition. In our study, the comparison is the disease progression rate before and after transplantation, which is a within-subject comparison. The not-transplanted patients’ series and the pretransplantation period of observation in the transplanted cases provided an estimate of disease progression over time in the absence of transplant. The potential bias is related to lack of homogeneity of disease progression in not-transplanted patients and grafted patients before transplantation. We did not find major differences in that, but we preferred to present two analyses, the first using the total patients’ series and the second using only grafted patients. A strong placebo effect has been demonstrated in the context of Parkinson's disease.30 The difference between the transplantation effect estimated on the grafted patients’ series and the transplantation effect estimated on the total HD patients’ series (see table 5, figure 2 and online-only material tables S2A–C) may be interpreted due to a placebo effect and/or a residual regression to the mean effect. In fact, we found a slightly higher pretransplantation deterioration rate in patients actually transplanted. Notwithstanding these potential biases, our report is important because randomised trials have not been approved for fetal striatal transplantation yet.21
Follow-up measurements varied in number and timing among patients, depending on the patient-specific clinical course. We have taken into account these data features by linear mixed models. Patients entered the transplantation protocol at different times since onset and, therefore, we cannot disentangle a potential calendar period effect from the effect of time since disease onset. This did not introduce important biases because in the last 15 years no decisive therapeutics has been introduced.31 We adjusted for disease burden at onset and other confounding variables. Our results were robust as documented in the sensitivity analysis (see online supplementary data), when we also accounted for heterogeneity of transplantation effect among patients. Our post-transplantation follow-up was around 4 years, and extrapolation to longer follow-up times should be considered with attention.
In our study, fetal striatal grafting was associated with slower motor and cognitive deterioration rate, but did not halt disease progression. Bachoud-Levy et al9 focused on an immediate relief or even improvement that plateaued over about 2 years, followed by a progression of symptoms. Barker et al8 reported no sustained functional benefit and concluded that this may relate to the small amount of grafted tissue. However, no differences in the total amount of grafted cells between Barker et al8 and our study are apparent (table 3), suggesting that other patient/donors features need further exploration. Barker et al8 analysed the individual evolution of each outcome on ‘time since transplantation’ matching grafted patients with a comparable series of not-transplanted patients defining a counterfactual, hypothetical time of transplantation for them. We found that grafted patients after transplantation exhibited a slower disease progression, but after some years, the patients’ condition will be the same as before transplantation. This does not imply absence of effect, because the correct comparison is between the observed and the expected condition if transplantation had not taken place (table 6). To do this, it is important to adjust for time since disease onset and burden of disease at onset. The Bachoud-Lévi et al9 analysis could be considered similar to what we addressed in measuring the change-in-intercept after transplantation. This variation occurring immediately after surgery should be discussed as a potential tractotomy effect.
Chorea was the most responsive sign in limbs and trunk. Dystonia benefited in a minor way, while fetal striatal transplantation did not affect bradykinesia and rigidity. Effects were also seen in the cephalic district, particularly tongue protrusion and eye movements. Long-term stabilisation of eye movements has already been reported.9 Since neural circuits involved in ocular movements are mainly in the caudate body and tail, regions outside the tissue deposits, this benefit cannot be explained by a direct mechanism of substitution of striatal neurons. We did not observe any significant improvement in gait or postural control. Inadequate grafting of postcommissural putamen has been hypothesised as a possible cause.9 In our study, even extensive grafting of postcommissural putamen7 did not result in significant improvement in gait and postural competence. We speculate that the circuits involved are no longer adequately represented in the residual putamen and, therefore, unlikely to be restored by a substitutive mechanism.
Post-transplantation decline in cognitive tasks of UHDRS was slower than in controls. Partial recovery of learning motor abilities was suggested by improvement in Luria item. These results may relate to a better allocation of attention resources and suggest a beneficial effect of fetal striatal grafting on the executive domain. A modulation of the excitatory cortical efferences probably explains these cognitive benefits. The relative impact of graft development and/or of thalamocortical tractotomy on this effect is not known. Even if grafted patients showed improvement in judgment capacity and awareness, their behaviour was not significantly affected by transplantation. Tractotomy per se might explain the early feeling of well-being reported by patients just after the first surgery, which was performed on the non-dominant hemisphere.
Benefits to functional capacity have been reported.9 Grafted patients in our study did not show substantial functional improvement. Six patients recovered their previous capacities or simple home activities, but the benefit persisted in only three of them.
Transplantation induced persistent improvement in striatal metabolic activity, suggesting graft survival and development. The effects seen at the 2-year PET reversed the progressive annual decrease of striatal metabolism expected in HD.32 Thereafter, as already reported by Gaura et al33 and by Bachoud-Lévi et al,9 the slight decline in striatal metabolism supports the hypothesis that the pathological process does not stop. Cortical metabolism did not decrease after grafting, contrary to progressive annual decrease expected in HD.34 An increase in D2-receptor binding as measured by [123I]IBZM SPECT suggests progression in striatal differentiation of the graft as already assessed using 11C-raclopride PET.10 Overall, these data suggest that striatal/cortical hypometabolism is reversible in HD, and striatal grafts can anatomically and functionally replace degenerated neurons, thus supporting the rationale of transplantation.
In conclusion, human fetal striatal transplantation favourably affected the motor and cognitive course of HD. Longer follow-up is necessary to understand whether transplantation can have a significant impact on the natural history of the disease in terms of overall survival and/or time spent in earlier disease stages. If further studies will confirm our results, it might be worthwhile to perform transplantation in less severely affected patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors MP, AB, and PG designed the study and wrote the manuscript with support from BP, NDL, and LM. MP, AMR, CM, EG, and SP analysed neurological data. PG performed the neurosurgical procedures. SB, LL, RS, and GBV performed the fetal tissue preparation procedures. AB and DC performed statistical analysis. VB and MM analysed imaging data. BP analysed genetic and immunogenetic data.
-
Funding This work received grants from Ministero Istruzione Università e Ricerca, Italy (PRIN 2008, research programme N 2008XN9KLA) and by Ente Cassa di Risparmio, Florence, Italy (2011.120).
-
Competing interests None.
-
Ethics approval The study was authorised by the Italian National Health Institute, National Transplantation Centre (upon approval by Health Ministry, Consiglio Superiore di Sanità, Sessione XLV, Sezione II, 21 July and 22 September 2005, and acceptance by the National Bioethics Committee).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Raw anonymised data available upon request to the corresponding author.
Linked Articles
- Editorial commentary