Article Text

Abstract
Objective To evaluate the effectiveness of anterior temporal lobectomy (ATL) versus selective amygdalohippocampectomy (SAH) on seizure-free outcome in patients with temporal lobe epilepsy, using both direct and indirect evidence from the literature.
Methods MEDLINE, Embase and Cochrane databases were searched for original research articles and systematic reviews comparing ATL versus SAH, and ATL or SAH versus medical management (MM). The outcome was seizure freedom at 12 months of follow-up or longer. Direct pairwise meta-analyses were conducted, followed by a random-effect Bayesian network meta-analysis (NMA) combining direct and indirect evidence.
Results Twenty-eight articles were included (18 compared ATL vs SAH, 1 compared ATL vs SAH vs MM, 8 compared ATL vs MM, and 1 compared SAH vs MM). Direct pairwise meta-analyses showed no significant differences in seizure-free outcome of ATL versus SAH (OR 1.14, 95% CI 0.93 to 1.39; p=0.201), but the odds of seizure-free outcome were higher for ATL versus MM (OR 29.16, 95% CI 10.44 to 81.50; p<0.00001), and SAH versus MM (OR 28.42, 95% CI 10.17 to 79.39; p<0.00001). NMA also showed that the odds of seizure-free outcome were no different in ATL versus SAH (OR 1.15, 95% credible interval (CrI) 0.84–1.15), but higher for ATL versus MM (OR 27.22, 95% CrI 15.38–27.22), and SAH versus MM (OR 23.57, 95% CrI 12.67–23.57). There were no significant differences between direct and indirect comparisons (all p>0.05).
Conclusion Direct evidence, indirect evidence and NMA did not identify a difference in seizure-free outcome of ATL versus SAH.
Statistics from Altmetric.com
Introduction
Temporal lobe epilepsy (TLE) is the most common cause of drug refractory epilepsy, especially in adults. Eighty per cent of TLEs have onset in the hippocampus,1 and hippocampal sclerosis is a major aetiology in the adult epilepsy surgery series. Advances in neuroimaging and neurophysiology have enabled more precise localisation of the epileptogenic zone and the eloquent areas, thus helping in planning surgical resection. Two randomised controlled trials have established the superiority of epilepsy surgery over medical management (MM) for patients with TLE.2 3 Standardised anterior temporal lobectomy (ATL) involves removing 4–6 cm of the anterior temporal lobe, including the amygdala and hippocampus. Selective amygdalohippocampectomy (SAH), the other common surgery for TLE, preserves the temporal neocortex and underlying white matter, and offers theoretical advantage of lower cognitive decline following surgery. The choice of resective surgery for TLE remains elusive. Previous meta-analyses have shown discordant findings, with ATL reported to achieve better seizure outcome when compared with SAH in two meta-analyses,4 5 and similar seizure outcome was reported with ATL and SAH in another meta-analysis.6 Hu et al 4 also showed that there was no significant difference in full-scale performance and verbal IQ scores of ATL relative to SAH. Further, all three meta-analyses were conducted using standard pairwise comparison of ATL versus SAH.
Network meta-analysis (NMA) has the advantage of incorporating both direct and indirect evidence. Direct evidence compared ATL relative to SAH; indirect evidence compared the relative effect of either of these two temporal lobe surgeries with the common comparator, that is, MM. NMA includes multiple pairwise comparisons across a range of interventions, that is, ATL versus SAH, ATL versus MM, and SAH versus MM, and provides estimates of the relative effect on multiple treatment comparisons.7 The aim of this systematic review and NMA was to evaluate the effectiveness of ATL versus SAH on seizure-free outcome, using both direct and indirect evidence from the literature.
Methods
Search strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline. MEDLINE, Embase and the Cochrane databases were searched systematically (on 27 June 2017) using the key terms ‘temporal lobe epilepsy’, ‘anterior temporal lobectomy’ and ‘amygdalohippocampectomy’. The search strategy is detailed in online supplementary table 1. We also screened the reference section of the included articles for any additional relevant studies.
Supplemental material
Original research articles (experimental or observational) and systematic reviews comparing ATL versus SAH, ATL versus MM, or SAH versus MM for TLE, with at least 12 months of follow-up, were included. Searches were restricted to English-language articles published from 1990 to 2017. If there were multiple studies reporting on overlapping patient populations from the same centre, the most recent article was used. Exclusion criteria were non-human studies, grey literature, conference abstracts, case reports and editorials.
Data extraction
Two authors (PJ and EW) independently extracted the data including author, year of publication, country of origin, interventions used, study design, criteria for choosing a particular intervention, investigations for presurgical evaluation, age at the time of surgery or study enrolment, duration of epilepsy, side of surgery, duration of follow-up, sample size, classification used for seizure outcome and seizure-free outcome. Any disagreement in the extracted data was resolved by reaching a consensus through discussion. Where the relevant data were missing, we contacted the corresponding author for further details.
Outcome measure
The outcome was seizure freedom on follow-up at 12 months or longer. If the seizure outcome was reported at multiple prespecified time points, outcome at 2 years was used for the meta-analysis and NMA.
Data analysis
Meta-analyses: direct pairwise comparisons
RevMan (Review Manager) V.5.2 was used for direct pairwise meta-analyses.8 Three separate meta-analyses were done, comparing ATL versus SAH, ATL versus MM, and SAH versus MM. The data from various studies were pooled and expressed as OR with 95% CI. A p value <0.05 was considered statistically significant. We used the Q statistic and I2 to test for between-study heterogeneity. If statistically significant heterogeneity was present (Q statistic p<0.05 or I2 ≥50%), the pooled estimate and 95% CI were calculated using a random-effect model. If there was no significant heterogeneity between studies, the fixed-effect model was used. Publication bias was assessed using funnel plot. The funnel plot was visually assessed for asymmetry, which is indicative of potential publication bias. Assessment of publication bias was conducted if there were at least three studies for each pairwise comparison.
Subanalyses were conducted for ATL versus SAH for studies reporting on surgery for hippocampal sclerosis only; studies reporting on seizure-free outcome at 1-year, 2-year and 5-year follow-up; studies reporting complete seizure freedom and free from disabling seizures; and studies published before and after 2000.
Network meta-analysis
A random-effect NMA combining direct and indirect evidence was performed within a Bayesian framework9 using R V.3.3.3, gemtc package. Consistency of direct and indirect evidence was assessed using node-splitting models. The consistency results were considered insignificant when the p value was greater than 0.05 for the comparison between direct and indirect effects in the node-splitting analysis. Model convergence was assessed using the Gelman-Rubin statistics, and convergence was considered to have been achieved if the widths of pooled runs and individual runs stabilised around the same value and their ratio was approximately 1.
Quality of evidence
The GRADE Profiler software (V.3.2) was used to assess the quality of evidence included in the meta-analyses. The following were considered in the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) criteria10: study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, magnitude of effect, dose response gradient and residual confounding. The quality of evidence was classified as very low, low, moderate or high.
The quality of previous systematic reviews was assessed by the Assess the Methodological Quality of Systematic Review (AMSTAR) tool.11
Results
Of the 4696 citations identified, full texts of 51 articles were reviewed for eligibility (figure 1). Twenty-eight studies were included in this systematic review. Twenty-three studies were excluded as the outcomes of interests were not reported,12–27 there was overlapping patient population,28–30 unclear nature of surgery,31 32 or the follow-up was less than 1 year.33 34
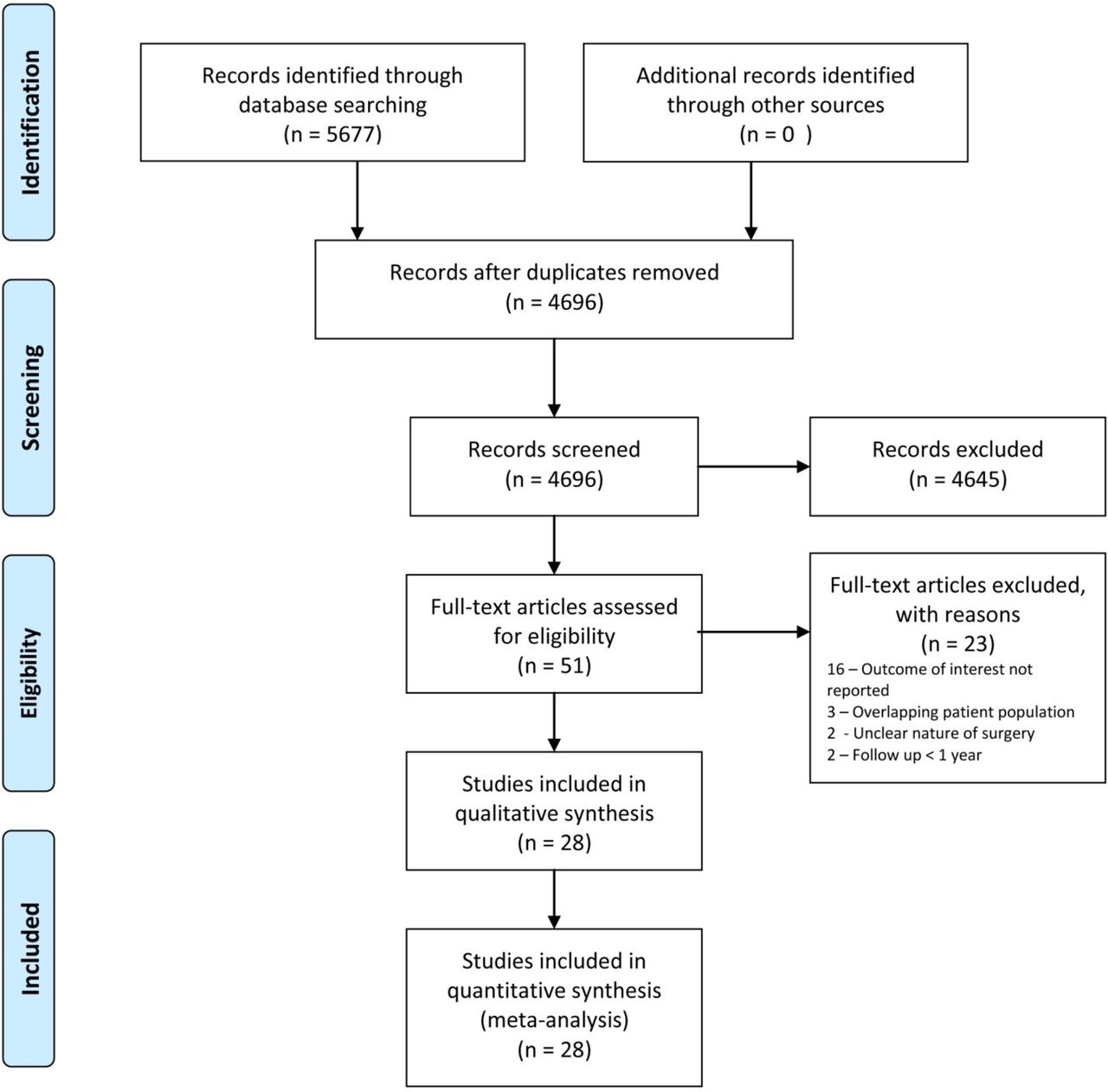
PRISMA flow chart of study selection and reasons for exclusion. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The study characteristics are summarised in online supplementary table 2. The studies were from the USA (8), Canada (5), Brazil (4), Germany (4), UK (4), France (1), Japan (1), Australia (1) and Pakistan (1). All the included studies were observational studies except for two randomised controlled trials.2 3 Four were prospective studies35–38 and the rest were retrospective or had unknown study designs. Of the 28 articles included, 18 studies provided direct pairwise comparison of ATL versus SAH,35 36 39–54 1 study compared three interventions (ATL, SAH and MM),55 8 studies compared ATL versus MM,2 3 38 56–60 and 1 study compared SAH versus MM.37 In 17 studies, the outcome was seizure freedom (or specified using Engel Ia or International League against Epilepsy (ILAE) class I), and in 12 studies the outcome was freedom from disabling seizures.
Supplemental material
The SAH was done through transcortical (nine studies), trans-sylvian (seven studies) and subtemporal (two studies) approaches. In most studies, selection of the surgical procedure was based on time period, with SAH being conducted later in the study period compared with ATL, surgeon’s expertise or preference. Majority of the studies enrolled adult patients except one.44 The mean duration of epilepsy was predominantly greater than 10–20 years, with the exception of the Early Randomized Surgical Epilepsy Trial,2 where the median duration of epilepsy was 5.2 years. Hippocampal sclerosis was the exclusive aetiology in 12 articles.36 37 40 41 45 47 48 52–54 57 60
Previous systematic reviews
We found three systematic reviews and meta-analyses4–6 comparing ATL versus SAH. The odds of seizure-free outcome were lower for SAH relative to ATL in one systematic review,4 and the relative risk of seizure-free outcome was higher for ATL relative to SAH in another systematic review5 (see online supplementary table 3). One systematic review did not identify significant differences in the relative risk of seizure-free outcome of ATL versus SAH.6 The detailed AMSTAR scoring is tabulated in online supplementary table 4.
Meta-analyses: direct pairwise comparisons
ATL versus SAH
There were 19 studies comparing ATL versus SAH. There was no significant difference in seizure-free outcome following ATL relative to SAH (OR 1.14, 95% CI 0.93 to 1.39; p=0.20) (figure 2). The funnel plot (figure 3A) showed no evidence of publication bias. The quality of evidence was ‘very low’ (online supplementary table 5).
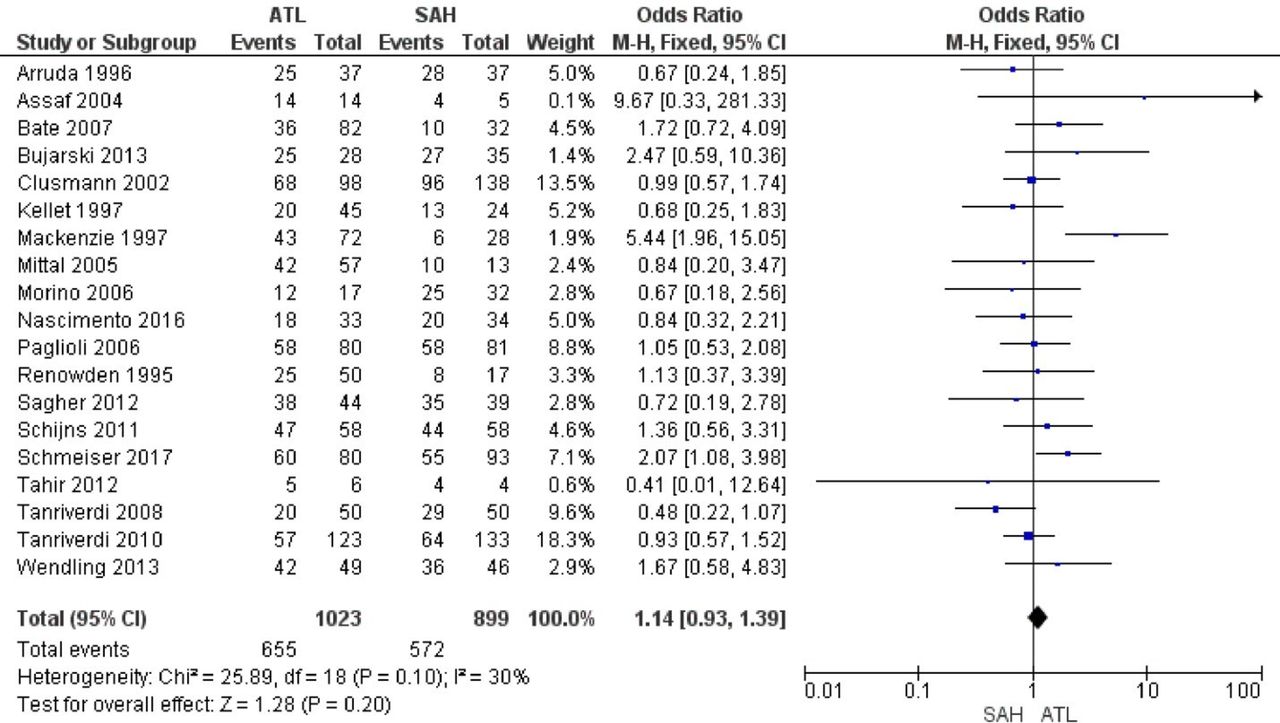
Forest plot comparing anterior temporal lobectomy (ATL) and selective amygdalohippocampectomy (SAH) for seizure-free outcome. M-H, Mantel-Haenszel.

Funnel plots of anterior temporal lobectomy (ATL) versus selective amygdalohippocampectomy (A), and ATL versus medical management (B).
Subgroup analysis (online supplementary table 6) of studies that included patients with hippocampal sclerosis only36 40 41 45 47 48 52–54 showed no significant difference in the seizure-free outcome of ATL versus SAH (OR 1.05, 95% CI 0.80 to 1.37; p=0.75). Subgroup analyses of studies that reported on seizure-free outcome at 1-year (OR 1.08, 95% CI 0.82 to 1.41; p=0.58), 2-year (OR 1.48, 95% CI 0.97 to 2.27; p=0.07) and 5-year (OR 1.49, 95% CI 0.82 to 2.70; p=0.19) follow-up also did not show significant differences in seizure-free outcome of ATL versus SAH. Studies reporting complete seizure freedom (OR 0.95, 95% CI 0.73 to 1.24; p=0.72) and studies published before 2000 (OR 1.10, 95% CI 0.83 to 1.46; p=0.52) and after 2000 (OR 1.36, 95% CI 0.89 to 2.09; p=0.15) did not show any significant difference in seizure outcome of ATL versus SAH (online supplementary table 6). However, studies reporting freedom from disabling seizure showed that ATL had higher odds of freedom from disabling seizure compared with SAH (OR 1.48, 95% CI 1.16 to 1.87; p=0.001).
ATL versus MM
There were nine studies comparing ATL versus MM. The odds of seizure-free outcome were significantly higher for ATL as compared with MM (OR 29.16, 95% CI 10.44 to 81.50; p<0.00001) (figure 4). The funnel plot (figure 3B) showed evidence for publication bias, with fewer studies on the right of the funnel plot, suggesting that the effect size would have been smaller if there were more studies on the right of the funnel plot. The quality of evidence for the nine studies was ‘very low’.

Forest plot showing the comparison between anterior temporal lobectomy (ATL) and medical management (MM) for seizure-free outcome. M-H, Mantel-Haenszel.
SAH versus MM
Two studies compared SAH versus MM. The odds of seizure-free outcome were also significantly higher for SAH as compared with MM (OR 28.42, 95% CI 10.17 to 79.39; p<0.00001) (figure 5). The quality of evidence for these two studies was ‘very low’.
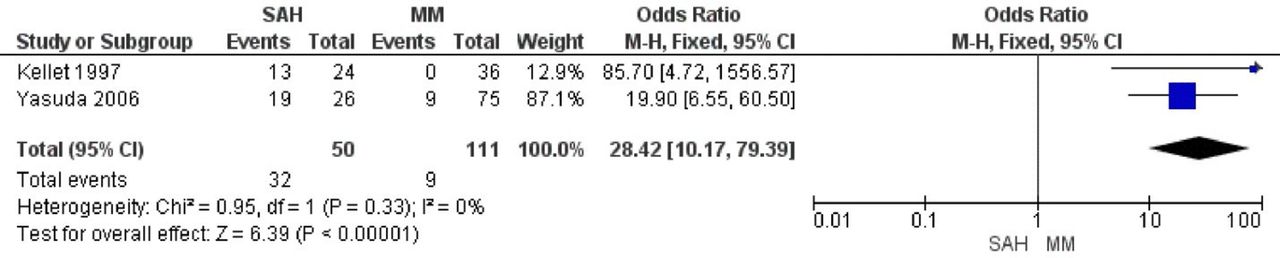
Forest plot showing the comparison between selective amygdalohippocampectomy (SAH) and medical management (MM) for seizure-free outcome. M-H, Mantel-Haenszel.
Network meta-analysis
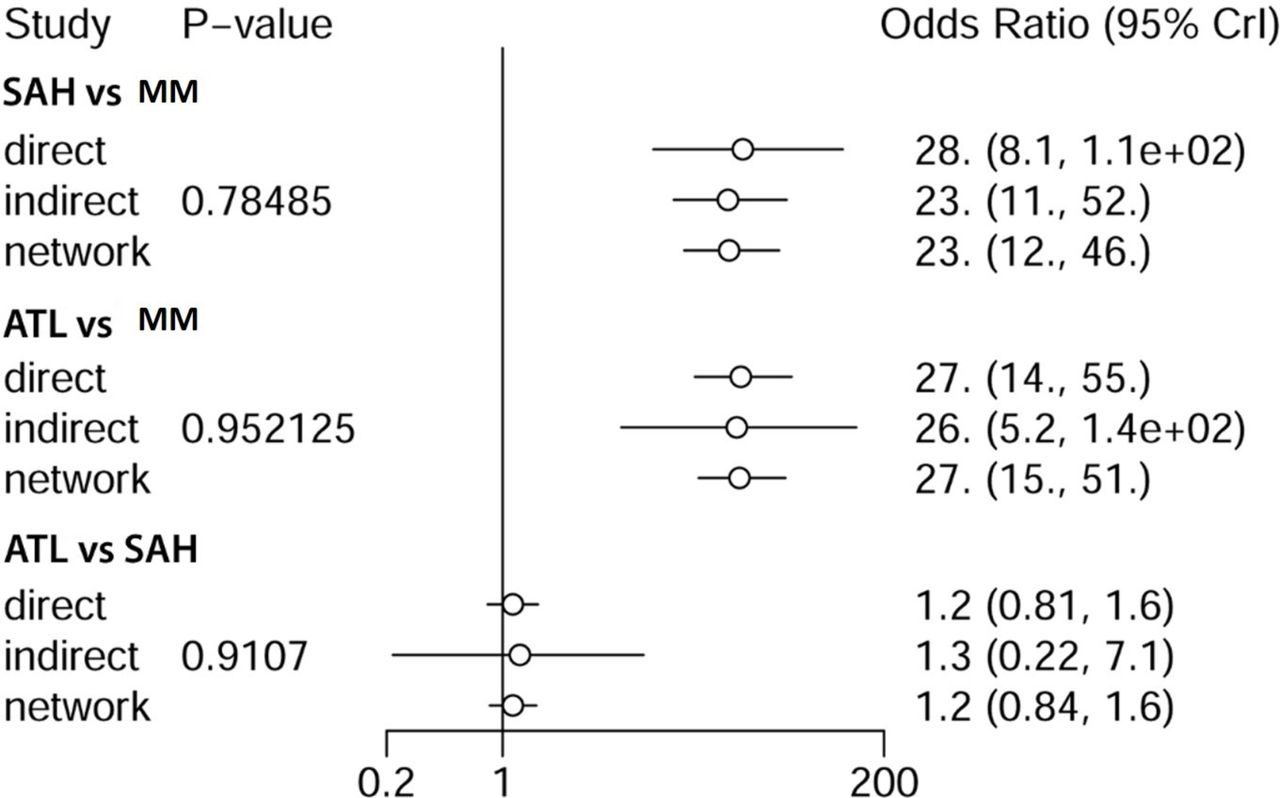
The network plot (online supplementary figure 1) shows that the strength of comparison, as reflected by the edges linking the treatment strategies, was greatest for ATL versus SAH, followed by ATL versus MM, and weakest for SAH versus MM. NMA showed that there was no difference in the odds of seizure-free outcome of ATL versus SAH (OR 1.15, 95% credible interval (CrI) 0.84–1.15). The odds of seizure-free outcome were higher for ATL versus MM (OR 27.22, 95% CrI 15.38–27.22) and also for SAH versus MM (OR 23.57, 95% CrI 12.67–23.57). There were no significant differences between direct and indirect comparisons for the three pairwise comparisons (ATL vs SAH, ATL vs MM, and SAH vs MM) (all p>0.05) (figure 6). The Gelman diagnostic indicated that the model converged (all 1.00).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[SP1.jpg]](https://jnnp.bmj.com/content/jnnp/89/11/1138/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
Forest plot for the direct and the indirect comparisons and network meta-analysis. There were no significant differences between direct and indirect comparisons for the three pairwise comparisons (ATL vs SAH, ATL vs MM, and SAH vs MM) (all p>0.05). The values of the odds ratio are truncated after the decimal points if more than 10. ATL, anterior temporal lobectomy; CrI, credible interval; MM, medical management; SAH, selective amygdalohippocampectomy.
Discussion
Existing meta-analyses have used direct pairwise comparison of ATL versus SAH. The study by Josephson et al 5 included 11 articles in their meta-analysis and found that the relative risk of freedom from disabling seizures was 1.3 times higher with ATL compared with SAH. In the meta-analysis conducted by Hu et al,4 the authors also included 11 articles in their meta-analysis and demonstrated that the odds of seizure freedom were 0.65 times lower for SAH compared with ATL. Kuang et al 6 did not find a significant difference in seizure control rate 1 year after surgery, but only included six articles in their meta-analysis. The difference in findings of these meta-analyses could be related to the inclusion of different number of studies, studies with different follow-up duration or restricting the studies to those with 1-year follow-up. There were more studies that were included in our meta-analysis compared with prior meta-analyses by Josephson et al 5 and Hu et al.4 In particular, there were seven studies that were not included in prior meta-analyses—Arruda et al,39 Renowden et al,48 Tahir et al,51 Sagher et al,49 Bujarski et al,41 Wendling et al 54 and Nascimento et al 46—which demonstrated no significant difference in seizure-free outcome of ATL versus SAH. The inclusion of new data from these studies may have contributed to differences in this study’s conclusion relative to prior meta-analyses.
This study combined both direct and indirect evidence, which may strengthen the assessment of direct pairwise comparison of ATL versus SAH,61 as both direct and indirect evidence contribute to the total body of evidence. Combining direct and indirect evidence may avoid bias from omission of data, and can give more precise estimates of treatment effects.9 In our study, we have included 19 articles with direct pairwise comparison of ATL versus SAH, and 10 articles (one of the articles compared ATL vs SAH vs MM) provided indirect comparison of ATL or SAH with MM. By including more evidence in the pairwise analysis compared with the study by Josephson et al 5 and Hu et al,4 we showed that ATL did not achieve significantly better seizure-free outcome relative to SAH. Further, we demonstrated that direct and indirect evidence, as well as NMA, all reached the same conclusion, in that ATL was not superior to SAH in achieving seizure-free outcome. It is possible that improvement in presurgical evaluation, including high-resolution structural and functional imaging, and technical advances in electroencephalography (EEG), may have contributed to improved selection of candidates for SAH.
The criteria for selecting the surgical technique (ATL vs SAH) in the articles were variable and were frequently based on institutional preference and expertise of the neurosurgeon. Few studies also reported preferred use of SAH if the interictal/ictal EEG findings were restricted to the mesial temporal lobe. A previous randomised controlled trial comparing 2.5 cm vs 3.5 cm mesial temporal resection in TLE found no difference in seizure freedom rate for the 2.5 cm resection relative to 3.5 cm resection group, suggesting that adequate volume resection rather than maximal volume resection is more important for good seizure outcome.62 Given that complete resection of the epileptogenic zone plays an important role in determining the success of epilepsy surgery, there could be a preference for SAH if the interictal/ictal EEG findings were localised to the mesial temporal lobe. There are various surgical approaches for SAH, such as trans-sylvian, transcortical/transtemporal and subtemporal approach, which have been postulated to have different theoretical advantages,63 and the use depends on surgeons’ experience and skills. Studies comparing these approaches are limited and showed similar seizure outcome.48 64 65
There is lack of consensus in the literature regarding the neuropsychological outcomes following ATL and SAH.63 The standardised mean differences in verbal IQ, performance IQ and full-scale IQ following ATL and SAH were found to be not significant in a meta-analysis.4 Schramm66 showed that 11 out of 14 articles on SAH reported better cognitive outcome. Tanriverdi et al 53 reviewed cognitive outcome after temporal lobe surgery and found that 16/21 studies demonstrated better cognitive outcome after SAH, compared with 5/21 studies which showed no difference. Due to the lack of standardised testing and reporting of neuropsychological outcome in the literature, we did not undertake a meta-analysis of neuropsychological outcome following ATL versus SAH. Neuropsychological outcomes following temporal lobe surgery are dependent on factors other than the type of surgery, including cortical eloquent sites for language or memory,67 pathological status (presence or absence of hippocampal sclerosis)68 and age at seizure onset, with older age at seizure onset associated with worse outcome.69
There are several limitations to this systematic review and meta-analyses. All direct evidence, that is, pairwise comparison of ATL versus SAH, were observational studies and were of ‘very low’ quality evidence. Similarly, all except two indirect evidence, that is, pairwise comparison of ATL or SAH versus MM, were observational studies and were of ‘very low’ quality evidence. Another limitation of this study is the variability in the definition of seizure-free outcome. Over half of the articles used complete seizure freedom to infer seizure-free outcome, while just under half of the articles used freedom from disabling seizures as the outcome measure. Heterogeneity with respect to duration of follow-up could potentially confound the findings. We have conducted subgroup analyses and showed that seizure-free outcomes at 1-year, 2-year and 5-year follow-up were not significantly different between ATL and SAH. There was also heterogeneity in aetiologies, criteria for selection of surgical procedures and surgical approach for SAH. A randomised controlled trial comparing ATL versus SAH will overcome many of the methodological limitations of observational study, and could include seizure freedom as an outcome measure, and other outcome measures such as neuropsychological performance and health-related quality of life.
In summary, we have included direct and indirect evidence from the literature to evaluate seizure-free outcome of ATL versus SAH. We have used NMA to incorporate all relevant evidence from the literature so as to provide a more precise estimate of the treatment effect compared with using direct evidence of pairwise comparison of ATL versus SAH. We showed that direct evidence, indirect evidence and NMA did not identify a difference in seizure-free outcome of ATL versus SAH in TLE, suggesting that in patients with mesial TLE, ATL is not superior to SAH in achieving seizure-free outcome. However, there are methodological limitations in the existing literature, highlighting the need for a randomised controlled trial so as to provide a definitive answer on the effectiveness of ATL versus SAH.
Acknowledgments
The authors would like to thank Alanna Marson (librarian at The Hospital for Sick Children) for assisting with the literature search.
References
Footnotes
Contributors EW and PJ planned the study. PJ and EW performed the systematic review and meta-analysis. PJ and EW wrote the first draft of the manuscript. PJ, GT, CS, BS and EW provided inputs for the revision of the first draft of the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.