Article Text

Abstract
The neurodegenerative syndrome amyotrophic lateral sclerosis (ALS) is characterised by increased cortical excitability, thought to reflect pathological changes in the balance of local excitatory and inhibitory neuronal influences. Non-invasive brain stimulation (NIBS) has been shown to modulate cortical activity, with some protocols showing effects that outlast the stimulation by months. NIBS has been suggested as a potential therapeutic approach for disorders associated with changes in cortical neurophysiology, including ALS. This article reviews NIBS methodology, rationale for its application to ALS and progress to date.
- als
- motor neuron disease
- electrical stimulation
- magnetic stimulation
- neurophysiology, expt
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is an aetiologically complex neurodegenerative syndrome of the motor system and its wider cerebral networks.1 There is a clinicopathological overlap with frontotemporal dementia through a shared molecular signature of neuronal and glial cytoplasmic aggregates of the 43 kDa transactive region DNA-binding protein—TDP-43. No highly effective disease-modifying therapy exists, and progressive muscular weakness results in a median survival of 30 months from symptom onset. Understanding the underlying pathological processes is therefore of vital importance.
A number of studies have been performed which have investigated changes in inhibitory signalling in the primary motor cortex early in the disease. The observation of a somatotopically enlarged region of cortical activation during the performance of a focal motor task using activation positron emission tomography (PET) led to the first hypothesis that ALS pathogenesis may involve a relative reduction in cortical inhibitory interneuronal signalling,2 as cortical representations are thought to be determined by local circuits involving the inhibitory neurotransmitter g-aminobutyric acid (GABA).3
A substantial body of evidence suggests pathological loss of inhibitory neuronal influences in ALS.4 Postmortem studies show depletion of GABA-ergic (parvalbumin-positive) inhibitory interneurons in the motor cortex in ALS, irrespective of the severity of Betz cell loss.5 Additionally, reduction in GABAA receptor α1 subunit expression in surviving pyramidal cells of the prefrontal cortex implies specific dysregulation of GABAA-mediated inhibitory signalling.6 Postmortem findings are corroborated in vivo by evidence of reduced motor cortex binding of the GABAA-selective PET ligand flumazenil.7 Cortical GABA-ergic signalling is further pathophysiologically implicated in ALS by loss of physiological short-interval cortical inhibition (SICI)—a GABAA-mediated phenomenon—demonstrated by paired-pulse transcranial magnetic stimulation.8 Loss of SICI is a consistent observation across the clinically heterogeneous syndrome of ALS and predates the onset of symptoms in carriers of ALS-causing genetic variants.9
Another manifestation of lost intracortical inhibitory signalling might be widely dysfunctional cortical dynamics. For example, interhemispheric functional connectivity10 and callosal structural integrity11 12 are reduced in ALS. Furthermore, integrated analysis of white-matter structural information and resting-state functional connectivity suggests a pattern of increased functional connectivity as white-matter tract damage increases with disease progression.13 14 A putative mechanistic explanation for these various lines of evidence is a progressive pathological loss of cortical inhibitory signalling over time.
In addition to cortical dysfunction, loss of inhibition may contribute directly to the degenerative process in ALS. Excitotoxic mechanisms of cell death have been postulated in ALS due to the finding of excess glutamatergic activity.15 The first licensed disease-modifying treatment for ALS, although with only a small effect on survival, is the broadly antiexcitatory drug riluzole.16 17 Although several drugs with broadly proinhibitory cortical action have appeared ineffective for the treatment of ALS, such studies relied on relatively insensitive clinical outcome measures such as manual muscle strength testing and rate of decline of a composite disability score.18 Modulation of cortical inhibitory influences in ALS is therefore a plausible strategy to mitigate disrupted motor system function, and more speculatively to modify the degenerative process.
Non-invasive brain stimulation (NIBS) encompasses a set of promising research tools that may modulate cortical inhibitory signalling in this way.19 NIBS approaches are applied through the scalp and skull with the common goal of modulating brain activity using some form of energy—electrical current, magnetic pulses or focused ultrasound. These operate at a wide range of scales, from cortical microcircuits to wider brain regions, and can exert effects that persist for hours to days (figure 1). However, there remain significant doubts about the efficacy and reproducibility of NIBS in even the healthy brain. This article reviews the range of NIBS techniques, underlying physiological mechanisms, current limitations and potential application to ALS.

A simplified overview of a range of interventions that alter brain function, with their spatial and temporal scale. tFUS is very early in development, putatively offering finer spatial resolution than other NIBS techniques. Adapted with permission from Polania 2018, N ature R eviews N euroscience. NIBS, non-invasive brain stimulation; tFUS, transcranial focused ultrasound; rTMS, repetitive transcranial magnetic stimulation; tACS, transcranial alternating current stimulation; tDCS, transcranial direct current stimulation; tRNS, transcranial random noise stimulation.
Stimulation methods
Historical development
Electrical stimulation of biological tissues has a long history. Roman physician Scribonius Largus reportedly applied electric shocks from live torpedo fish to the forehead in the treatment of headache. Galvani demonstrated in 1791 that electrical current could make a dismembered frog leg twitch. Ten years later, his nephew Aldini applied direct-current stimulation over a moistened area of the parietal scalp in a farmer diagnosed with ‘melancholy’, reporting improvement in mood.20 A variety of enterprising practitioners from 1870 to 1930 promoted do-it-yourself electrical therapies for indications including headache, pain, insomnia and low mood.21 Mainstream adoption followed with the description of electroconvulsive therapy (ECT) by Italian neurologists Ugo Cerletti and Luigi Bini in 1938.22 The original forms of ECT involved the application of much larger currents across the entire head to evoke seizures, and supplanted interest in the smaller currents used for transcranial stimulation for decades. The promise of smaller currents as potential therapies has only recently been more widely investigated.
NIBS approaches are commonly categorised according to the form of energy used to stimulate the brain: magnetic, electrical (figure 2), and most recently ultrasonic. Transcranial electrical stimulation can be further subdivided into transcranial direct current (tDCS), alternating current (tACS) and random noise (tRNS) stimulation. NIBS can also be classified into neurostimulatory approaches, whereby stimulation directly induces action potentials in the underlying neuronal tissue, or neuromodulatory techniques, which act by modulating the ongoing firing rate of stimulated tissue. In both categories, a range of secondary mechanisms have been proposed to explain the long-term effect—this is discussed further for each modality.

Examples of commercial (A) transcranial direct current stimulation and (B) transcranial magnetic stimulation equipment (C,D) coil/electrode montage over motor cortex, and (D,E) maps of electrical fields generated.
Transcranial direct current stimulation
Modern interest in transcranial direct current electrical stimulation was sparked by the demonstration that weak direct current stimulation over the motor cortex modulated excitability in the cortical representation of the hand.23 tDCS involves the application of a small direct current (1–2 mA) through a circuit formed by two or more electrodes (at least one cathode and anode) applied to the scalp with conductive gel or paste. This produces a gradient electric field that alters resting neuronal membrane potential and excitability properties - presumed to be subthreshold for action potential generation.24 25 Protocols vary extensively in electrode size, placement, current applied and duration of stimulation.26 27
Depending on the protocol used, the effect of a single session of tDCS on cortical excitability can persist for 90 min beyond cessation of stimulation, or longer.28 The frequency of tDCS sessions is also thought to determine the duration of effect. Repeated sessions with short intervening breaks are associated with excitability alterations up to 24 hours later,29 and longer term behavioural effects have been demonstrated.30
Wide inter-individual and between-session variability is reported in tDCS. These differences in response may be partly explained by the underlying mechanisms of tDCS, and therefore can potentially be reduced if the physiological effects of tDCS are better understood. To this end, in addition to human studies, in-vitro, animal and computational models have been used to elucidate the physiological mechanisms of tDCS. Brain tissue preparations can model the effect of an electrical field at the single cell level, with complex effects depending on the predominant orientation of the cell relative to the field (see figure 3A). Of particular importance is the alignment of the subcellular structures where action potentials originate (soma, axon hillock and apical dendrites)31 with respect to the field direction. If aligned with the field, the cell becomes electrically polarised–depolarised at the soma and hyperpolarised at the axon terminal.32 This reduces the threshold potential at the axon hillock. However, where a cell is perpendicular to the field, this effect is negligible as smaller compartments bounded by membranes restrict current and the gradient is smaller.33 As a result, cortical microarchitecture, macroscopic folding and orientation relative to the conducting skin pad will all determine which subpopulations of neurons become more excitable. Computational models of the electric field also demonstrate the impact of pad size, skin contact, skull thickness and head shape on the field geometry.25 The acute effects of tDCS on excitability are abolished by voltage-gated ion channel blockade, but unaffected by glutamate or GABA antagonism, suggesting the primacy of electrical effects in the acute phase.34 Conversely, the N-methyl-D-aspartate (NMDA) receptor antagonist dextromethorphan abolishes the after-effect of both anodal and cathodal tDCS, suggesting a role for glutamatergic synaptic function.35
{kind=link}
{kind=link}
{kind=link}
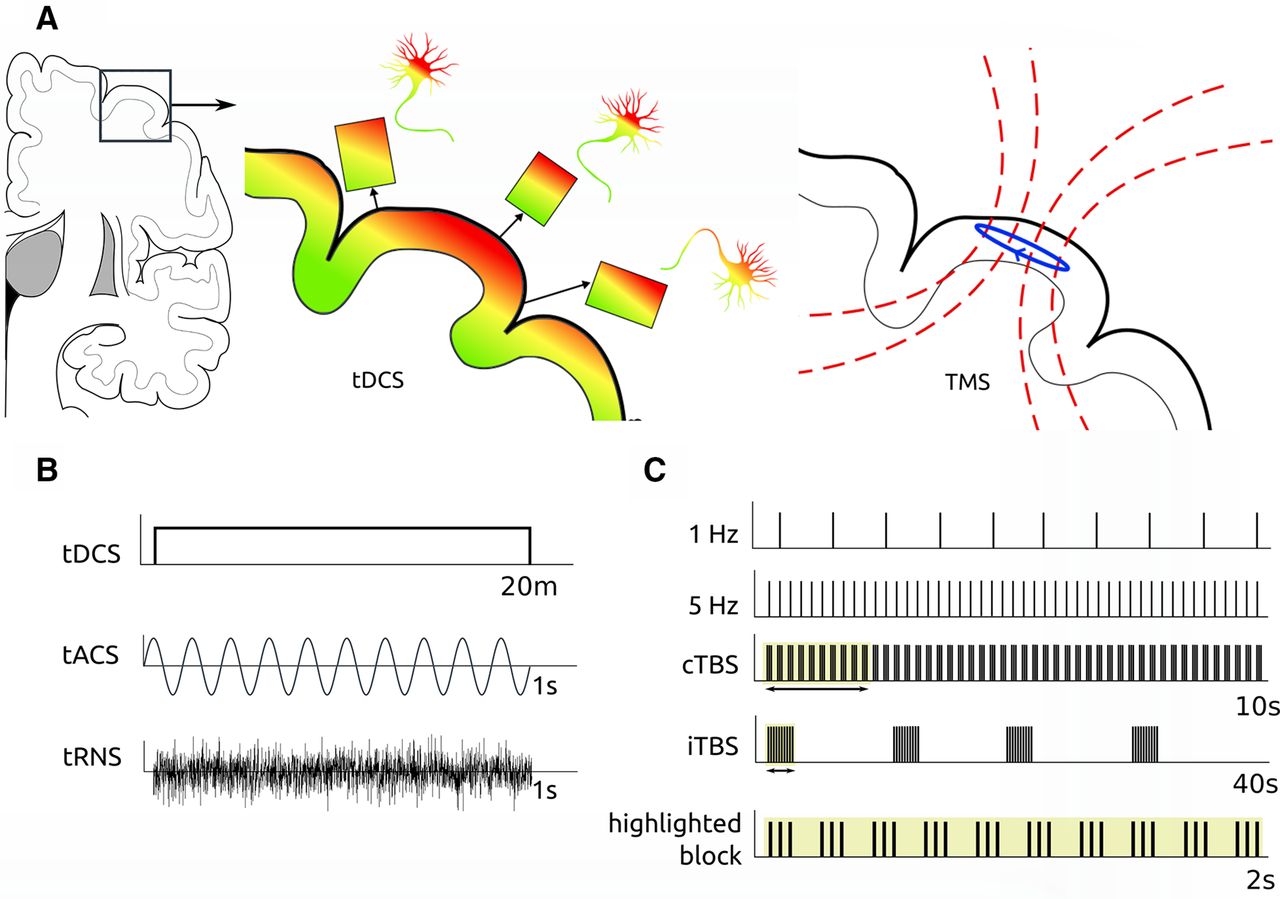
(A) Representations of electrical and magnetic fields induced by tDCS and TMS with influence of cortical orientation on the fields experienced. (B) Different patterns of current that may be applied transcranially. (C) Different stimulation frequencies and the cTBS pattern in repetitive TMS. cTBS, continuous TBS; iTBS, intermittent TBS; tACS, transcranial alternating current stimulation; TBS, theta burst stimulation; tDCS, transcranial direct current stimulation; tRNS, transcranial random noise stimulation; TMS, transcranial magnetic stimulation.
Neurochemical changes after stimulation can also be quantified using magnetic resonance spectroscopy (MRS). Some MRS studies have demonstrated an increase in glutamate after anodal stimulation and decrease in glutamate after cathodal stimulation, although this has not been consistent in all studies.36 37 More consistently, GABA has been shown to be decreased after both anodal and cathodal stimulation—and for at least 1 hour after anodal tDCS38–leading to the suggestion of GABA as a gating factor whose reduction allows plastic changes to occur. The neurochemical basis of the tDCS after-effect also helps explain its variability, with multiple factors affecting neurochemical concentrations—such as alertness, sleep quality and caffeine—varying both within and between subjects.
Although less well understood, tDCS may also influence brain function at larger scales. Motor cortex (M1) anodal tDCS results in increased functional connectivity both within M1,39 and between M1 and anatomically distant motor-related brain regions.40 The links between the effects of stimulation at these distinct spatial scales have yet to be fully explored.
Other electrical stimulation protocols
A sinusoidal, or alternating, current is delivered across two scalp electrodes (of similar size and placement to tDCS) in tACS. tACS is believed to interact with ongoing frequency-specific activity within the stimulated brain regions, potentially leading to entrainment of endogenous rhythms, although this has yet to be definitively proven. The behavioural effects of tACS are modest, although with increasingly sophisticated waveform parameters there is increasing evidence as to its behavioural relevance.41 42
High-frequency (100–640 Hz) tRNS with a random stimulation pattern with a bell-shaped probability distribution has also been suggested to increase motor cortex excitability.43 The physiological basis, reproducibility, and effect size of tACS/tRNS are less well understood than tDCS, and to date they have not been applied to ALS.
Transcranial ultrasound
In 1955, the formation of a pinpoint brain lesion using high-energy focused ultrasound was demonstrated in a cat.44 Precise intracranial lesioning using mechanical energy has been widely applied as a non-invasive neurosurgical technique in movement disorders and malignancy. At much lower energies where tissue is not damaged, a neuromodulatory role for transcranial focused ultrasound (tFUS) is emerging. Application of tFUS over the primary somatosensory cortex can elicit tactile sensations in the hand.45 Recently, a neuromodulatory effect on motor cortex excitability has been suggested when tFUS is applied in conjunction with transcranial magnetic stimulation (TMS).46 Focused ultrasound is in its very early days as a neuromodulatory technique and its effects on the brain are not yet clear. As this technique is refined and the underlying mechanisms investigated, it may find wider application, with key advantages of precise spatial localisation and access to deep structures.
Transcranial magnetic stimulation
Magnetic fields have historically been shown to interact with nervous system function. French physician Jacques Arsène d’Arsonval described in 1896 the induction of physiological effects by induction from a coil carrying 42 Hz alternating current: ‘There occurs, when one plunges the head into the coil, phosphenes (bright spots in the visual field) and vertigo, and in some persons, syncope…’.47 48
In 1985, Anthony Barker and colleagues49 at the University of Sheffield reported using a pulsed magnetic field to stimulate the motor cortex and peripheral nerves. Modern TMS remains fundamentally similar—involving the use of a magnetic field generator (‘coil’) placed over the scalp. Coils vary in material and geometry, resulting in differing magnetic field patterns; for example, ‘figure of eight’ coils have been developed to deliver a more focal pattern of activation than the original round coils.50 A short-lived, large, electric current is passed through the hand-held coil, which generates a magnetic field. Through electromagnetic induction, this rapidly changing magnetic field induces a current flowing parallel but opposite to that in the coil in the brain, a nearby conducting medium. The current produced can be targeted to the hand area of the motor cortex using electromyographic recording of the motor evoked potential (MEP) in the intrinsic muscles (reviewed in detail in ref 51).
As with tDCS, the effects of TMS vary depending on the protocol used. Single-pulse and paired-pulse protocols are powerful neurophysiological tools to investigate cortical excitability. The paired-pulse TMS measures intracortical facilitation (ICF) and SICI assess cortical glutamatergic and GABA-ergic activity, respectively.52 TMS can also be used as a tool for modulating cortical excitability. Repetitive TMS (rTMS), where trains of pulses are used at a variety of frequencies, has been suggested to have prolonged effects on cortical excitability. The specific frequency and pattern of stimulation can produce divergent responses—low frequency constant-rate rTMS (1 Hz) decreases motor cortex excitability, while excitability increases with higher stimulation frequencies (10 Hz).53
More recently, higher frequency TMS stimulation patterns that mimic physiologically occurring activity have been developed. Similar responses to constant-rate stimulation have been reported with much shorter stimulation time and fewer pulses. Theta burst stimulation (TBS), which has garnered increasing interest in recent years, depends on the application of three pulses at 50 Hz, delivered every 200 ms.54 This pattern can be delivered as continuous TBS (cTBS) as a 40 s train with a total of 600 pulses, or as intermittent TBS (iTBS), with 2 s blocks of TBS separated by 8 s intervals with no stimulation (figure 3). cTBS protocols have been suggested to produce depression of motor cortex excitability for up to 60 min poststimulation,54 but with more recent debate as to whether effects are reproducible in all subjects.55
The variability (between-protocol, inter-individual and intra-individual) of rTMS effects may be explained by individual-level factors (including age, sex, genetics, sleep quality, exposure to caffeine) and tissue-level factors affecting the specific populations of cortical neurons stimulated. As with tDCS, the orientation of cortical folding with respect to the TMS coil will affect the direction and depth of currents induced in the brain.50 Cortical cytoarchitecture, axon fibre diameter and preferential axon orientation will affect which specific populations of neurons are stimulated. In particular, inter-individual variation in intracortical circuit function (as measured by latency of MEP responses) can predict response to iTBS versus cTBS.56
As with tDCS, mechanisms of synaptic plasticity such as long-term potentiation (LTP) or long-term depression (LTD) have been invoked to explain the rTMS after-effect.57 58 NMDA receptor antagonists inhibit the after-effects of both cTBS and iTBS,59 suggesting a role for LTP mediated by glutamatergic signalling. The divergent effects of cTBS and iTBS may in part be explained by interactions between GABA-ergic signalling and the mechanisms of LTP, with motor cortex GABA significantly increased after cTBS,36 although the effects of iTBS on M1 GABA have yet to be explored.
A wide range of other mechanisms that may play a significant role in the effects of both tDCS and rTMS have been suggested, including serotonergic60 or dopaminergic61 neurotransmission, brain-derived neurotrophic factor (BDNF), neuroinflammation and glial signalling. A full understanding of NIBS techniques may require the integration of processes across a wide range of spatial and temporal scales and may allow fine-tuning of stimulus frequency, intensity and duration to maximise effect.
Current state of NIBS in ALS
To assess the progress to date in applying NIBS techniques to ALS, a systematic search of the National Center for Biotechnology Information (NCBI) MEDLINE database was undertaken on 22 February 2019. Entries were included if a term identifying ALS and a term identifying a stimulation technique were present in medical subject heading (MeSH) terms or title/abstract. The following were the full search terms:
(((Amyotrophic Lateral Sclerosis [MeSH Terms]) OR Motor Neuron Disease [MeSH Terms])) AND ((Transcranial Direct Current Stimulation [MeSH Terms]) OR (Transcranial Magnetic Stimulation [MeSH Terms]) OR (Magnetic Field Therapy [MeSH Terms])))
OR
(amyotrophic lateral sclerosis [Title/Abstract]) AND ((transcranial direct current stimulation [Title/Abstract]) OR (transcranial magnetic stimulation [Title/Abstract]) OR (transcranial alternating current stimulation [Title/Abstract]) OR transcranial focused ultrasound [Title/Abstract]))
From 276 initial results, 72 duplicates were removed. The remaining 204 were manually reviewed and filtered for relevance. Results were excluded if not original research (n=55), not conducted in humans with ALS (n=19) or applied stimulation for purposes other than persistent neuromodulation (n=118)—for example, paired-pulse TMS as a diagnostic marker. One study was reported twice—the preliminary report was excluded. After review, 11 studies remained and are summarised in table 1.
Summary of identified studies using non-invasive brain stimulation techniques in ALS with the aim of prolonged neuromodulation62–68 70–73
Repetitive TMS
Four studies62–65 applied the cTBS pattern. Stimulation frequency varied in the remaining studies. Two studies66 67 compared low-frequency (1 Hz) and high-frequency (20 Hz) rTMS. Zanette et al 68 used an intermediate frequency of 5 Hz with the stated rationale of combining the effects of reduced cortical excitability with low-frequency rTMS and BDNF release at high frequencies.
No consistent pattern in outcomes was seen. Di Lazzaro et al 69 reported a statistically significant reduction in the Revised ALS Functional Rating Score (ALSFRS-R) declines with active cTBS but this was not replicated in the follow-up study by the same group in 2009.62 Munneke et al 64 assessed neurophysiological outcomes of a short cTBS protocol, finding that it induced a reduction in MEP in both the controls and participants with ALS, but with more sessions of stimulation required to reach the same effect size in the ALS group. Ceccanti et al 70 assessed the effect of a low-frequency paired associative stimulation protocol before and after riluzole administration.
Transcranial direct current stimulation
Three studies of tDCS in ALS were identified. Quartarone et al 71 reported that the after-effects of tDCS seen in healthy individuals were not reproducible in patients with ALS. Munneke et al 72 assessed neurophysiological outcomes (single-pulse MEP, paired-pulse SICI and ICF) in participants with ALS and in healthy controls after single tDCS sessions lasting 7, 11 or 15 min. The reduction in MEP with tDCS seen in the control group was not replicated in individuals with ALS. No significant effect of tDCS on SICI or ICF was demonstrated in either group. Madhavan et al 73 applied anodal, cathodal and sham tDCS over the motor cortex in a single subject safety pilot, with no reported adverse effects. While electrode montages were consistent between studies, the application of 2 mA current raises concerns about blinding, while the number and duration of sessions differed significantly.
Current limitations
Small sample sizes, clinical heterogeneity, variable sham techniques and stimulation protocols are all sources of potential type II error in published studies of NIBS in ALS. Power calculations are not routinely presented in the literature,74 and estimates of the effect size of tDCS in particular have decreased as the body of literature has grown.75 Where sham stimulation is used at all, it has been suggested that double-blind procedures are imperfect,76 with skin redness in tDCS77 and subtler cues such as the position of the operator78 reducing blinding efficacy. TMS sham coils, while mimicking the click produced on pulse generation, cannot reproduce somatosensory stimulation from peripheral nerve stimulation, or indeed motor stimulation, and may be fundamentally insufficient.79
Adopting more robust operator procedures and publishing indices of blinding efficacy (eg, Bang’s Blinding Index80) may address widespread concerns over blinding methodology in NIBS. Methodological variations may arise from stimulation frequency and duration, along with coil and electrode positioning. There is evidence of non-linear (and sometimes contradictory) responses to increased duration or intensity of tDCS,81 so that simplistic concepts such as proinhibitory cathodal stimulation become less convincing. Potential drug effects may be ethically difficult to exclude in patient populations, and riluzole has been shown to influence cortical excitability in several studies.82 83
Future prospects
The continued pursuit of NIBS as a therapeutic intervention in ALS is justified based on the emerging understanding of the pathology as a more complex degeneration across cerebral networks.84 Neuromodulation via brain stimulation could potentially reduce pathological processes directly or support compensatory mechanisms. Measuring effect is a challenging aspect of all therapeutic studies in ALS. The rate of change in the ALSFRS-R is clinically relevant but too insensitive to demonstrate short-term proof-of-principle effects.
Progress in NIBS will depend on greater standardisation of delivery and more robust short-term and longer term markers of successful modulation of cortical function. The effects of modulation by NIBS are currently difficult to predict even in the healthy state, given the currently superficial understanding of brain function at the synaptic through to network level. As a more integrated and detailed understanding of the mechanisms of NIBS is built, this may allow more rational design of stimulation protocols to maximise effect. Much as the TBS pattern increases the efficacy and efficiency of rTMS, protocols with varying frequency and incorporating bursting activity85 may advance the state of transcranial electrical stimulation. Maximising effect size will be essential to apply NIBS as a neuromodulatory or neuroprotective approach in neurodegenerative disease. In the context of ALS, despite underwhelming outcomes to date, advances in the understanding of cortical microcircuit and network-level dysfunction10 86 point towards therapeutic potential. Alterations in resting-state functional MRI of carriers of highly penetrant, ALS-causing genetic mutations are demonstrable prior to the onset of symptoms.87 Magnetoencephalography may be sufficiently sensitive to changes in the dynamic brain function to detect dysfunction amenable to early modulation.88 As a more detailed understanding of the complex cortical oscillatory dysfunction in ALS emerges,89 more sensitive measures of target engagement will be developed.90 Standardisation of stimulation protocols and robust study designs that allow for rapidly accruing disability will realise the goal of NIBS as a therapeutic tool in ALS.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
Footnotes
Contributors Study concept and design: ECE, CJS, MRT. Data acquisition and analysis: ECE, MRT. Drafting and critical review of the manuscript: ECE, CJS, MRT. All three authors approved the version published and are accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.