Article Text

Abstract
Objective In patients with atherosclerotic major cerebral artery disease, low blood pressure might impair cerebral perfusion, thereby exacerbate the risk of selective neuronal damage. The purpose of this retrospective study was to determine whether low blood pressure at follow-up is associated with increased selective neuronal damage.
Methods We retrospectively analysed data from 76 medically treated patients with atherosclerotic internal carotid artery or middle cerebral artery disease with no ischaemic episodes on a follow-up of 6 months or more. All patients had measurements of the distribution of central benzodiazepine receptors twice using positron emission tomography and 11C-flumazenil. Using three-dimensional stereotactic surface projections, we quantified abnormal decreases in the benzodiazepine receptors of the cerebral cortex within the middle cerebral artery distribution and correlated these changes in the benzodiazepine receptors index with blood pressure values at follow-up examinations.
Results The changes in the benzodiazepine receptor index during follow-up (mean 27±21 months) were negatively correlated with systolic blood pressure at follow-up. The relationship between changes in benzodiazepine receptor index and systolic blood pressure was different among patients with and without decreased cerebral blood flow at baseline (interaction, p<0.005). Larger increases in benzodiazepine receptor index (neuronal damage) were observed at lower systolic blood pressure levels in patients with decreased cerebral blood flow than in patients without such decreases.
Conclusion In patients without ischaemic stroke episodes at follow-up but with decreased cerebral blood flow due to arterial disease, low systolic blood pressure at follow-up may be associated with increased selective neuronal damage.
- carotid artery disease
- middle cerebral artery disease
- positron-emission tomography
- benzodiazepine receptor
- blood pressure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- carotid artery disease
- middle cerebral artery disease
- positron-emission tomography
- benzodiazepine receptor
- blood pressure
Introduction
In patients with atherosclerotic internal carotid artery (ICA) or middle cerebral artery (MCA) disease, chronic reductions in cerebral perfusion pressure may increase their risk for cerebral ischaemic damage.1–4 Although severe ischaemia causes ischaemic stroke, ischaemia of moderate severity may cause selective neuronal damage.5–7 In patients with chronic haemodynamic impairment caused by atherosclerotic major cerebral artery disease, transient decreases in perfusion pressure may reduce perfusion below the penumbra threshold for minutes, which may cause selective neuronal damage without overt stroke.8–11 Low blood pressure (BP) might impair cerebral perfusion in patients with atherosclerotic major cerebral artery disease12 and thereby exacerbate the degree of haemodynamic impairment and the risk of selective neuronal damage in these individuals.2 13 Therefore, low BP at follow-up may be associated with a risk of selective neuronal damage during the follow-up period. However, no studies have investigated the relationship between BP and selective neuronal damage during this period. Given its association with cognitive impairment, selective neuronal damage may constitute an essential target for the treatment of patients with chronic haemodynamic impairment.14–16
Because most cortical neurons express central-type benzodiazepine receptors (BZRs), specific imaging of these receptors allows for in vivo visualisation of neuronal receptors alterations induced by ischaemia.17 18 For instance, selective neuronal damage can be detected in humans using positron emission tomography (PET) and 11C- flumazenil (FMZ), a ligand for BZR.6 7 We retrospectively analysed the relationship between BP at follow-up and the changes in the BZRs during follow-up in patients with atherosclerotic ICA or MCA disease and no ischaemic stroke episodes during follow-up. The aim of this study was to determine whether low BP at follow-up is associated with increases in selective neuronal damage, evaluated as a decrease in BZRs.
Subjects and methods
Patients
In this study, we did a retrospective analysis of a prospectively collected data set investigating the relationship between changes in selective neuronal damage and haemodynamic impairment in patients with atherosclerotic ICA or MCA disease.8 We used 76 patients with a follow-up time of 6 months or more in these analyses (table 1). All patients were part of a previously published data set.8 We evaluated the distribution of BZRs in the brains of these patients twice using PET. Patients were referred to our PET unit for evaluation of the haemodynamic effects of ICA or MCA disease as part of a comprehensive clinical evaluation to determine whether they required vascular reconstruction surgery.
Patient characteristics
Inclusion criteria were as follows: (1) occlusion or stenosis of the ICA (>60% diameter reduction according to the North American Symptomatic Carotid Endarterectomy Trial criteria19) or MCA (>50% diameter reduction20) as documented by conventional or magnetic resonance (MR) angiography; (2) functional independence in daily life (a modified Rankin Scale score <3); (3) for symptomatic patients, history of transient ischaemic attack (TIA) or minor completed stroke in ICA or MCA distribution; (4) medical treatment with no TIA or stroke since the first PET examination; (5) availability and willingness to return for follow-up PET examination; and (6) a follow-up time allowance of 6 months or more. TIA was defined as focal symptoms of presumed ischaemic cerebrovascular origin lasting <24 hours. Exclusion criteria were (1) infarction in the cerebral cortex, in the cerebellum or in the brainstem detectable on routine MRI (T1-weighted, T2-weighted or fluid-attenuated inversion recovery imaging) or CT imaging; (2) a history of vascular reconstruction surgery; (3) unilateral arterial disease with extensive white matter lesions in both hemispheres, likely caused by bilateral small vessel disease; (4) a history of BZR agonist use; and (5) the presence of potential sources of a cardiogenic embolism.
We evaluated patient status with respect to hypertension, diabetes mellitus, ischaemic heart disease, hypercholesterolaemia and smoking at the first PET examination. Hypertension, diabetes mellitus, ischaemic heart disease or hypercholesterolaemia was judged to be present when there was a history of treatment.
To establish a control database for BZR imaging, we also enrolled 10 healthy control subjects, aged 57±7 years, including 7 men and 3 women with no history of medical or psychiatric disorder or of taking BZR agonists. Among them, seven subjects, aged 56±8 years, including four men and three women, attended follow-up PET examinations. The interval between first examination and follow-up PET studies ranged from 38 to 45 months (mean 41±3 months).
PET measurements
We performed PET scans for each patient using an advance whole-body scanner (General Electric Medical Systems, Wauwatosa, Wisconsin), which allows for the simultaneous acquisition of 35 slice image with an interslice distance of 4.25 mm.21 After a transmission scan using germanium-68/gallium-68 (68Ge /68Ga), we performed a series of 15O-gas studies.21 We placed a small cannula in the left brachial artery for blood sampling. C15O2 and 15O2 were delivered continuously to the patient via a mask for the duration of the 5 min scan. Cerebral blood volume (CBV) was measured based on bolus inhalation of C15O via a 3 min scan. We obtained arterial samples manually during scanning. We measured the radioactivity of the radiotracer, oxygen content and haematocrit. We measured BP via an arterial catheter connected to a pressure transducer. Averaged BP values during C15O2 and 15O2 scanning were used as BP values on PET examinations and were used for the analysis in this study.
15O-gas studies were followed by 11C-FMZ studies.9–11 22 C-FMZ was synthesised by 11C-methylation of demethylated-FMZ (Hoffmann-La Roche, Basel, Switzerland). After intravenous injection of 370–555 MBq of 11C-FMZ into the right antecubital vein using an automatic injector for 60 s, a 50 min dynamic PET scan was initiated at the time of tracer administration.
We used the steady-state method to calculate cerebral blood flow (CBF), cerebral metabolic rate of oxygen (CMRO2) and oxygen extraction fraction (OEF).23 CMRO2 and OEF were corrected on the basis of CBV. We calculated the binding potential (BP) (non-displaceable) of 11C-FMZ using dynamic data and Logan graphical analysis with reference tissue, by using the time-activity curves obtained from the pons (the reference region).22 24
To obtain normal control values for 15O-gas PET variables, we performed 15O-gas studies with arterial sampling across seven normal volunteers (four men and three women), aged 47±7 (mean±SD), who underwent normal routine neurological examinations and MRI scans.
Data analysis
We used a classical region-of-interest (ROI) approach to analyse 15O-gas PET scans. We analysed 10 tomographic planes from 46.25 to 84.5 mm above and parallel to the orbitomeatal line, which corresponded to the levels from the basal ganglia and thalamus to the centrum semiovale.25 The ROI was placed on the CBF images. We then examined each image by placing a total of 10–12 circular ROIs 16 mm in diameter compactly over the grey matter of the outer cortex in each hemisphere. According to the atlas prepared by Kretschmann and Weinrich,26 we distributed ROIs for all 10 images across the MCA as well as the external border-zone regions.25 26 We transferred the same ROIs to the other images. We then calculated the mean hemispheric value for the hemisphere affected by arterial disease as the average of all circular ROIs.
As previously described, we analysed the FMZ-BP parametric images with a three-dimensional stereotactic surface projection technique.10 27 This method anatomically normalised individual PET data to standard brain data. Pixels were located on the outer and medial surfaces of both hemispheres using a standard stereotactic system. The highest surface pixel value was compared between patients and controls. We normalised pixel values of an individual’s image set to the mean cerebellar value before examination. We calculated the Z-scores for each surface pixel ([mean normalised pixel value for controls − normalised pixel value for the patient] / SD for controls) and used them to scale decreases in FMZ-BP. Therefore, a positive Z-score depicted a reduced FMZ-BP compared with the control group.
To quantitate the degree of abnormal FMZ-BP reduction in each patient, we used the stereotactic extraction estimation method to compute the BZR index (defined as (% pixels with Z-score >2) × (average Z-score for those pixels)) for the MCA distribution, as previously described.10 28 An increased BZR index corresponds to a decreased BZR level, and thus greater cortical neuronal damage.
The mean CBF value acquired among the 14 control hemispheres from seven healthy volunteers was 44.6±4.5 mL/100 g/min. We considered the hemispheric CBF values below the lower 95% limit (mean minus 13t0 .05SD) defined in healthy subjects (below 35.0 mL/100 g/min) to denote decreased CBF.
On follow-up, we calculated the total change in the BZR index or the other PET variable values in the MCA distribution with arterial disease by deducing the values attained at the first examination from those acquired on follow-up examination. In controls, the calculation was carried out using the mean of the bilateral hemispheric values of the BZR index. The mean±SD value of changes in the index among controls was 0.94±1.38. In patients, an increase in the index beyond the upper 95% limit (the mean plus 6t0 .05SD), as defined in normal subjects (above 4.32), was considered to be an increased BZR index (indicating an increase in neuronal damage) at follow-up.
Statistical analysis
The statistical analysis was performed using StatView (SAS Institute, Cary, North Carolina, USA). We compared the clinical backgrounds or BZR index values between the two groups using a Student’s t-test or a Fisher’s exact test, as appropriate. We compared BZR index values between examinations using paired t-tests. Relationships between variables were analysed using simple or multiple regression analyses. Differences in the relationship between BP at follow-up and BZR index across subgroups (those with or without decreased CBF at baseline) were evaluated by analysis of covariance. For all analyses, statistical significance was considered to be p<0.05, unless stated otherwise.
Results
Overall, the changes in the BZR index, CBF, OEF and systolic BP (SBP) during follow-up were 14.14±33.9, –0.41±6.73 mL/100 g/min, 1.28%±7.68%, and −5.1±21.7 mm Hg, respectively. Thirty-seven patients had an increased BZR index during follow-up.
After simple regression analysis, there was a significant negative linear relationship between changes in the BZR index and SBP at the follow-up PET examination (r=−0.238; p<0.05) (figures 1 and 2). SBP at the baseline examination was not correlated with changes in the BZR index.
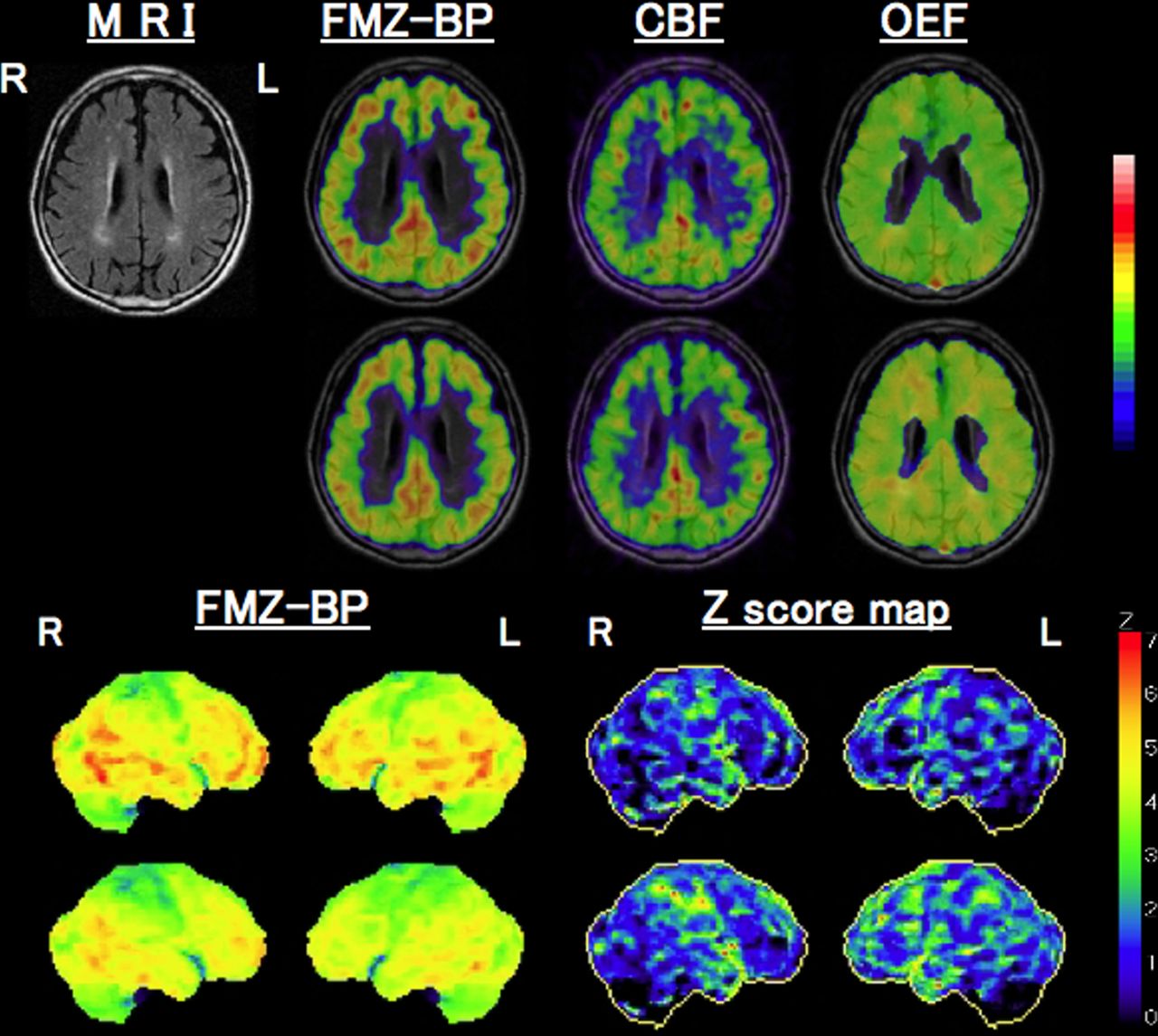
Representative images of decreased benzodiazepine receptor (BZR) expression in a patient with a right internal carotid artery occlusion and a left internal carotid artery stenosis (mild). Collateral pathways included the anterior communicating artery and leptomeningeal collaterals from the posterior cerebral artery. The first positron emission tomography study (first row) revealed a mild decrease in flumazenil-binding potential (FMZ-BP) in the right (R) hemisphere with internal carotid artery occlusion and subcortical ischaemic lesions (MRI), while cerebral blood flow (CBF) was decreased and the oxygen extraction fraction (OEF) was increased slightly. A follow-up 48 months later (second row) revealed decreased FMZ-BP and CBF with increased OEF in the R hemisphere. Mean hemispheric CBF decreased from 28.4 to 27.5 (mL/100 g/min), while OEF increased from 51.5 to 57.0 (%). Three-dimensional stereotactic surface projection images (3D-SSP images) and Z-score maps from the first (third row) and second (fourth row) examinations demonstrated a decrease in FMZ-BP in the R hemisphere, especially in the frontoparietal region. The BZR index increased from 35.9 to 103.1 between baseline and follow-up. The patient’s systolic blood pressure was 119 (mm Hg) at baseline and 107 at follow-up. Antihypertensive therapy was discontinued proximally to the follow-up examinations. The patient showed a mild attention deficit (a Mini Mental State Examination score of 26).

Scatter plot representing systolic blood pressure at follow-up versus changes of the benzodiazepine receptor (BZR) index at follow-up. The black line indicates a regression line for all patients. The dashed lines show the upper 95% limit of changes in the BZR index for the seven controls. CBF, cerebral blood flow.
Among patient characteristics (table 1), the interval between the first and follow-up PET studies was significantly correlated with changes in the BZR index (r=0.339; p<0.005), although patient age was not. We did not identify additional differences in changes in BZR index values between patients with and without male sex, symptom, cerebral ischaemic lesion, ICA disease, hypertension, diabetes mellitus, ischaemic heart disease, hypercholesterolaemia and cigarette use. No significant relationship was found between antihypertensive drug and changes in BZR index values.
Among PET haemodynamic variables at baseline, only CBF was significantly correlated with changes in the BZR index (r=−0.295; p<0.01). At follow-up, patients with decreased CBF values at baseline (n=39) showed a significant increase in the BZR index in the hemisphere with arterial disease, but not in the contralateral hemisphere (table 2). Patients without decreased CBF values at baseline (n=37) did not show significant changes in the BZR index in any hemispheres. Changes in the BZR index in the ipsilateral hemisphere among patients with decreased CBF values were significantly larger than those in patients without decreases.
BZR index values for hemispheres ipsilateral or contralateral to arterial disease
Multivariable linear regression analysis was used to investigate the association of changes in the BZR index with (1) CBF at baseline, (2) SBP at follow-up, and (3) the interval between the first and follow-up PET studies (table 3). Our analysis produced a model that included these three independent variables with a correlation coefficient of 0.518 for the changes in the BZR index (p<0.001). In our model, the CBF at baseline, SBP at follow-up, and the interval between the first and follow-up PET studies accounted for 10.1%, 5.3% and 11.5% of the variance in changes in the BZR index, respectively. The CBF at baseline and SBP at follow-up were negatively correlated with changes in the BZR index.
Multiple linear regression analysis with changes in the BZR index in the hemisphere with arterial disease as the dependent variable
The relationship between changes in the BZR index and SBP differed between patients with decreased CBF at baseline and those without (interaction, p<0.005) (figure 2). Larger significant increases in BZR index values were observed at lower SBP in patients with decreased CBF at baseline (r=−0.416; p<0.01), while smaller significant increases were observed at lower SBP in patients without decreases (r=−0.327; p<0.05) (figure 2).
In patients with decreased CBF at baseline, the relationship between changes in the BZR index and SBP at follow-up was also significant after adjustment for the interval between the first and follow-up PET examinations via multiple regression analysis (coefficient, −0.922; SE, 0.407; t=−2.265; p<0.05).
SBP at follow-up was negatively correlated with the changes (increases) in OEF during follow-up (r=−0.313; p<0.01) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Scatter plot representing systolic blood pressure at follow-up versus changes of the oxygen extraction fraction at follow-up.
At baseline, 41 patients were undergoing treatment via antihypertensive therapies. During follow-up, antihypertensive therapies were discontinued in two patients and started in two patients. SBP at follow-up was positively correlated with changes in the SBP at follow-up (r=0.535; p<0.001).
The separate analysis of the data for the 41 patients who were treated for hypertension at baseline showed similar results. Per a simple regression analysis, there was a significant linear relationship between changes in the BZR index and SBP at follow-up (r=−0.350; p<0.05), the interval between the first and follow-up PET studies (r=0.330; p<0.05), or CBF at baseline (r=−0.344; p<0.05). Using multivariable linear regression analysis, the CBF at baseline and SBP at follow-up were significantly correlated with changes in the BZR index, but the interval was not. Our analysis produced a model that included the CBF at baseline and SBP at follow-up with a correlation coefficient of 0.494 for the changes in the BZR index (p<0.005). In our model, the CBF at baseline and SBP at follow-up accounted for 12.1% and 12.3% of the variance in changes in the BZR index, respectively. The relationship between changes in BZR index and SBP differed between patients with decreased CBF at baseline and those without (interaction, p<0.005). Larger significant increases in BZR index values were observed at lower SBP in 19 patients with decreased CBF at baseline (r=−0.573; p<0.02), while smaller and non-significant increases were observed at lower SBP in 22 patients without decreases (r=−0.409; p=0.06).
Discussion
The present study demonstrated an association between low SBP at follow-up and increased damage to cortical neurons in patients with atherosclerotic ICA or MCA disease and no ischaemic stroke episodes at follow-up. Selective cortical neuronal damage at follow-up was indicated by an increase in the BZR index of the normal-appearing cerebral cortex in the affected hemisphere and was predicted by low SBP at follow-up. The relationship between increases in BZR index (selective neuronal damage) and SBP differed between patients with decreased CBF at baseline and those without decreases. Patients with decreased CBF at baseline and low SBP appeared to have an elevated risk of subsequent cortical neuronal damage.
In patients with atherosclerotic ICA or MCA disease, chronic reductions in cerebral perfusion pressure increased their risk for cerebral ischaemic damage.1–4 In patients with haemodynamic impairment, transient decreases in perfusion pressure may reduce perfusion below the penumbra threshold for minutes, which may cause selective neuronal damage without an overt stroke.8–11 Low BP might impair the long-term growth of cerebral collaterals.29 In patients with atherosclerotic ICA or MCA disease and no episodes of ischaemic stroke at follow-up, low SBP was associated with haemodynamic deterioration.13 In agreement with this, here we find that lower SBP was associated with a larger increase in OEF at follow-up, which is indicative of haemodynamic deterioration. Thus, low SBP may be associated with a sustained risk of ischaemic neuronal damage due to haemodynamic impairment in patients with atherosclerotic ICA or MCA disease. This may be especially true for patients with decreased CBF at baseline, because only small decreases in perfusion pressure may be required to reach the level of CBF below the penumbra threshold. The relationship between BP and the risk of selective neuronal damage in patients with decreased CBF may be different from that in patients without decreased CBF, and lower BP in this specific population may increase the risk of selective neuronal damage.
The separate analysis of the data for the 41 of 76 patients who were treated for hypertension at baseline also demonstrated that decreased SBP at follow-up was associated with increases in cortical neuronal damage at follow-up. Patients with hypertension with decreased CBF at baseline also appear to have an elevated risk of subsequent cortical neuronal damage when SBP at follow-up was low. In patients with antihypertensive therapies, BP levels measured at follow-up might reflect the target goal for BP control. Therefore, low target level of BP achieved might increase the risk of increased selective neuronal damage in such patients with decreased CBF.
The longer interval also contributed to the larger increases of BZR index, as a whole. Follow-up examinations in seven normal subjects, aged 56±8 years, demonstrated no significant change in Z index during follow-up (mean 41±3 months).10 Therefore, it seems unlikely that only simple ageing contributed to the observed declines in BZR binding over time. The interval was not correlated with changes in the BZR index in patients with hypertension, which suggested that the contribution of haemodynamic fluctuation or deterioration to neuronal damage might be more significant in patients with hypertension treatments than in patients without. We can provide two possible mechanisms other than haemodynamic mechanism due to decline in SBP. First, chronic oligaemia (CBF below 35.0 mL/100 g/min in this study) might cause prolonged inhibition of protein synthesis, which might result in delayed neuronal death.10 Second, long-term neuronal degeneration secondary to neuronal damage at baseline might develop during follow-up.6 In patients without hypertension, the effect of these two mechanisms might be stronger than the decline in SBP.
The treatment of hypertension is generally beneficial to patients with atherosclerotic major cerebral artery diseases.30 However, the level to which BP should be lowered to achieve maximal benefits among patients with atherosclerotic major cerebral artery disease remains unknown. The present study suggests that low SBP may increase the risk of cortical neuronal damage in hemispheres with decreased CBF. It is controversial whether BP controlled to lower levels is associated with a reduced risk of recurrent stroke in patients with atherosclerotic major cerebral artery disease and haemodynamic impairment.31–34 Further studies may be required to determine the optimal BP management in patients with atherosclerotic major cerebral artery disease.
The clinical correlations of the decline in BZR binding over time in this sample were unclear from the present study. Some patients developed new cortical symptoms, which were associated with regional cortical neuronal damage, as described previously.8 Although previous cross-sectional studies have demonstrated selective cortical neuronal damage manifested as a decrease in BZRs, which was associated with subtle cognitive impairment,14–16 follow-up studies including systematic neuropsychological tests are needed to correlate variable cortical dysfunction with regional differences of neuronal damage.
Limitations
The present study has some limitations which warrant discussion. First, BP was obtained only during a single visit, which may have led to a misclassification of ongoing BP levels. BP levels measured at follow-up were associated with increases in cortical neuronal damage, while BP levels measured at baseline or averaged at baseline and during follow-up were not. Although the timescale during which selective neuronal damage occurs is unknown, using BP measured during the follow-up period might allow for analysis of the relationship between selective neuronal damage and BP more proximally to the time of an ischaemic event. Furthermore, in the present study, we were unable to correct for partial volume effects. Decreases in cortical FMZ binding might at least partly reflect increases in cortical atrophy due to ischaemic tissue damage (ie, neuronal loss and partial volume effects), as well as decreases in tissue BZR expression, although we could have more explicitly measured this. It may be ideal that the data are analysed after corrections of PET data for atrophy based on coregistration of MR and PET scans. Lastly, normal control subjects were younger than our patients. Using the reported time-related slopes for CBF versus age (about −6% per decade),35 the adjusted CBF cut-off values in the present study became 31.6 mL/100 g/min, with an age difference of 16 years between patients and controls. Using this cut-off value, the results in the present study were unchanged (data not shown).
Conclusions
In patients without ischaemic stroke episodes at follow-up but with decreased CBF due to atherosclerotic ICA or MCA disease, low SBP at follow-up may be associated with increases in cortical neuronal damage at follow-up.
Acknowledgments
We thank the staff of the Department of Neurology and the Department of Neurosurgery, Shiga General Hospital, for providing clinical assistance.
References
Footnotes
Contributorship statement HY designed the study, contributed to PET imaging, analysed the data, wrote the first draft of the manuscript and modified all subsequent drafts. SK and CO contributed to PET imaging, contributed to interpretation of the data and contributed to all drafts of the manuscript. MT and KK performed PET scanning, analysed the data and contributed to all drafts of the manuscript.
Funding This study was funded by the Japan Society for the Promotion of Science KAKENHI (Grant numbers 17K09814, 26461323).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All protocols in this study were approved by the Shiga General Hospital Institutional Review Board, the Human Study Committee. All experiments were performed in accordance with the Declaration of Helsinki and Good Clinical Practice.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.