Article Text

Statistics from Altmetric.com
Introduction
At various times in history, technology has led to abrupt and far-reaching changes in how societies communicate: printing with moveable type in the 15th century; broadcasting in the 19th century and early 20th century; electronic transfer of information in the late 20th century; and machine learning with robotic systems in the 21st century. In that context, it is timely to reflect on the past, present and future trajectory of knowledge relating to medicine and what might be lost and gained as science and society increasingly enter the digital age. Here, the topic of interest is multiple sclerosis.
Multiple sclerosis in 2020: a synopsis
Broad consensus on the pathogenesis of multiple sclerosis was reached in the late 1980s, the application of which has since yielded significant advances in therapy. In 2020, a reasonable formulation would consider multiple sclerosis to involve a distinct geographical distribution resulting from the interplay of environmental and genetic aetiological factors; inflammatory and degenerative disease mechanisms working in sequence or in parallel expressed as an evolving phenotype characterised by intermittent and then progressive symptoms and signs leading to gradual accumulation of disability; clinical features and their pathological substrate represented by various surrogate laboratory biomarkers; the availability of therapies that modify the course of the illness but varying in their risks and benefits making for complex prescribing algorithms; and, underpinning the whole scientific endeavour, the wish to settle the hopes and fears for their future of affected individuals.
Digital technology and artificial intelligence
Digital technology uses binary rather than continuous analogue variables to detect patterns in large datasets, far outstripping the capacity of human agency for memory and analysis. Artificial intelligence develops systems that function according to preset rules but, primed by training datasets, generate their own information, learn from experience and adapt in order to achieve goals through deep learning. The boundaries of artificial intelligence are provisionally mapped in advance but the intermediate steps and eventual direction taken may be unpredictable and surprising. Lee Sedol was astonished by the seemingly incomprehensible but, as it turned out, inspired move 37 when Alpha Go systematically defeated the world expert in a game judged more complex than Deep Blue’s victories at chess over Gary Kasparov. Together, digital methods and artificial intelligence promise rapid advances in the speed and precision of analysis. One stated aim in biomedicine is to personalise medicine so that individuals are treated with bespoke drugs that match genomic determinants of pathology and pharmacological responses in the individual thus achieving optimum efficacy and safety for expensive medicines. There is no doubt that future technology will fill gaps and illuminate issues that now are ‘seen through a glass darkly’ (to paraphrase St Paul’s first letter to the Corinthians: chapter 13; verse 12). But the digital age will also challenge the relationship of information to knowledge and the nature of human agency.
Reasoning: concepts from the history and philosophy of science
Knowledge is a construct based on truth, resulting from inductive and deductive reasoning, which is verified, set in an historical context, formulated as language and in images, and communicated in groups. This attempt at a definition leans on the collective wisdom of older writers: Francis Bacon (1561–1626), Rene Descartes (1596–1650), John Locke (1632–1704), John Stuart Mill (1806–1873) and Claude Bernard (1813–1878). Philosophers in the ‘age of enlightenment’ argued that blind-faith in what was taught, ‘scholasticism’, was fraught with danger and that knowledge depended on evidence and reasoning. Furthermore, as reasoned by JS Mill, advancing the sciences and arts involves a partnership between ‘those who are living, those who are dead and those who are yet to be born’.
Francis Bacon argued for a ‘bottom-up’ model in which nothing is known or assumed in advance. All ideas and beliefs are assembled by induction from observations of the senses, the analysis of experience leading by stages to truthful conclusions. He advocated limiting the desire for knowledge to that which is practical: ‘if men had consulted experience and observation, they would have had facts and not opinions to reason about and might ultimately have arrived at the knowledge of the laws which govern the material world’. Bacon accepted that observations of the senses are not infallible and must be free from errors of the ‘tribe’ (seeing more than actually exists), the ‘den’ (reasoning disturbed by personal foible), the ‘forum’ (thought distorted by clever words), and the ‘theatre’ (ideas doggedly rehearsing prevailing dogma). Baconian logic was further developed by Locke: ‘five or six friends meeting in my chamber, and discoursing on a subject very remote from this, found themselves quickly at a stand[still] by the difficulties that arose on every side’. Their topic on that occasion was the nature of morality and religion but one consequence of the deliberations was a consideration of how the human mind uses empirical observation and natural philosophy to acquire knowledge. Ideas stem from the perception, memory and association of experiences which are then abstracted, ordered, rearranged and connected by reason and understanding into knowledge. This liberates the human mind to escape from doctrinal orthodoxy and blind trust: ‘the floating of other men’s opinions in our brains makes us not one jot the more knowing…external objects furnish the mind with ideas of sensible qualities; and the mind furnishes the understanding with the ideas of its own operations’. Locke argued that words get their meaning by representing ideas in our mind and that language is central to the formulation of beliefs.
Rene Descartes favoured the ‘top-down’ deductive school of reasoning, taking as his starting point: ‘I think, therefore I am [cogito, ergo sum]’. Consciousness and ideation are the basis of all knowledge. Ideas are disaggregated into simple questions and each is then further verified. Truth must not be selective through ignoring awkward issues. Descartes’ deductive method is valuable in its emphasis on hypothesis but vulnerable in that everything depends on the authority of thinking. By prioritising ideation and innate knowledge, deductive Cartesian logic risks the conclusion that the external world is inferred not real, a conundrum that the Baconian school avoids by starting with the authority of experience and material evidence.
Claude Bernard was concerned with the methodology of advancing scientific knowledge. He was comfortable with both inductive and deductive reasoning but argued that hypothesis must be verified or disproved experimentally by systematic elimination of individual components until one factor is shown to be causative through having determined that it is essential.
From this potted history of reasoning and method, it follows that the current state of knowledge in multiple sclerosis has benefited from the collective wisdom of inductive, deductive and deterministic enquiry.
The treatment of multiple sclerosis
By any standards the story of multiple sclerosis culminating, to date, in the licencing of 13 brand name drugs that, to a greater or lesser extent, modify the course of the disease is one of great success for scientific reasoning (figure 1). During the last two decades it has been shown that the frequency of relapse can be reduced; the accumulation of disability slowed; a prolonged state reached in which there is no evidence for disease activity; and existing disability partially reversed. Experience has shown that the first treatments to be introduced (beta interferons: six brands; and glatiramer acetate: two brands) are relatively safe but only modestly effective. The four more recently licenced oral therapies (cladribine, dimethyl fumarate, fingolimod and teriflunomide), acting through different mechanisms, offer convenience and somewhat improved efficacy, set against a slight increase in adverse effects profile. Three therapies are now licenced that, given intermittently by the intravenous route, confer much greater efficacy but with significant adverse effects profiles (alemtuzumab, natalizumab, ocrelizumab). In recognising that, at present, safety is being traded for increased efficacy, selecting among the menu of options and deciding which drugs to make available and use in clinical practice involves complex decision-making for physicians, licencing authorities and reimbursement agencies. The infrastructure needed to manage prescribing and meet the costs of drugs is significant. While not free from criticism, it is important to understand that the pharmaceutical companies marketing these medicines are seen to reap profits that seem excessive but are defended on the basis that the research and development costs and expenditure on clinical trials, together with losses on products in which unproductive investments were made, justify these prices. That there appears to be a cartel with costs largely equilibrated at the higher end of the profit margin seems undeniable. But discussion of capitalist economics belongs elsewhere.

A personalised representation of the relative safety and efficacy of licensed drugs for relapsing–remitting multiple sclerosis, using a design introduced by the author in 1999.
The situation with respect to progressive disease is less reassuring. Treatment for this currently disenfranchised group is roughly at the stage where matters stood for relapsing–remitting disease 15 years ago. There is often detectable efficacy in clinical trials involving patients who have entered the progressive phase of the disease using medicines licenced for relapsing–remitting multiple sclerosis. But it is altogether another matter whether this signal is useful for the individual, or merely something to be exploited for marketing reasons. That said, one drug is licensed for early primary progressive multiple sclerosis (ocrelizumab). Others have been evaluated without success (sodium channel blockers) or show some promise in progressive forms of multiple sclerosis (simvastatin, ibudilast, mitoxantrone and siponimod, in ascending order of perceived efficacy).
Success in the introduction of treatments for multiple sclerosis applies the concept, based on inductive and deductive reasoning with systematic deterministic examination, that the pivotal mechanism driving the pathogenesis of multiple sclerosis involves the migration (over and above normal immune surveillance) of T and B lymphocytes into the nervous system setting up a cascade of events ultimately leading to regional loss of myelin, astrocytic reactivity and axonal degeneration. Each of the medicines shown to be effective in multiple sclerosis thus far fits this model: drugs that trap T and B cells in solid lymph tissue; those that deplete lymphocytes in the circulation and elsewhere; interventions that prevent cellular migration into the brain and spinal cord; and those that non-specifically suppress immune reactivity and inflammatory processes. In turn, the adverse effects profiles, predicted and unexpected, can now be understood in terms not only of non-specific immune suppression but through the stochastic perturbations that follow immune cell depletion and reconstitution, and the consequences of inhibiting physiological surveillance of the central nervous system for maintaining the latency of persistent virus infection.
Multiple sclerosis as an immunological disease
The immune-centric hypothesis for the pathogenesis of multiple sclerosis has its own story. This begins with characterisation of the natural history and its separation into relapsing–remitting and progressive phases, either in sequence or evolving independently. Starting in the 1970s, these clinical accounts were supplemented by laboratory methods detecting the physiological consequences of (often subclinical) demyelination; the number and distribution of individual lesions; and the debris from areas of inflammation and degeneration. This led to the development of diagnostic criteria that combined clinical and paraclinical features, and their systematic revision as it became expedient to bring forward the point of diagnosis to the earliest at which this could safely be made in the interests of timely institution of treatment. No less important was consensus on an objective system for measuring disability. For all their limitations, the functional systems and expanded disability status scales have stood the test of time and not been displaced despite many complementary or directly competitive proposals. It is often forgotten that John Kurtzke (1926–2015) introduced these scales in the 1950s for the specific purpose of evaluating the clinical efficacy of isoniazid in multiple sclerosis: the treatment failed, but the scales survived.
Studies on the aetiology of multiple sclerosis also contributed to ideas on the immunological basis for tissue damage in multiple sclerosis. In 1972, Caspar Jersild and Arne Svejgaard (1937–2016) described an association between the HLA system and multiple sclerosis. Before long it was established that the class II HLA antigen DR2 and, later, its phenotypic and molecular subtypes DR15/DQ6 and DRB1*1501/DQB1*0602 confer the primary risk. The significance of this finding became apparent when Rolf Zinkernagel and Peter Doherty demonstrated that antigen in the form of small peptide sequences is presented by cells of the immune system held in the pockets of major histocompatibility complex molecules.
Many decades of work had already been expended on more directly considering the pathogenesis of multiple sclerosis based on evaluation of the neuropathology. The most perceptive analysis of the 19th century was provided by Eduard Rindfleisch (1836–1908) who pointed out (in translation) that: ‘three types of changes occur in parallel…first the alterations of blood vessels [inflammation]…secondly the atrophy of the nervous elements [neurodegeneration]…and third the metamorphosis of the connective tissue [sclerosis]’. What Rindfleisch could not answer was which of these components drives the pathogenesis. Opinions differed. Jean-Martin Charcot (1825–1893) in Paris emphasised the astrocytic response: ‘the predominant part accorded to the vessels…is anything but demonstrated…the concomitant hyperplasia of the reticulated fibres of the neuroglia constitutes the initial, fundamental fact, and necessary antecedent…the degenerative atrophy of the nerve elements…merely plays an accessory part’. Otto Marburg (1874–1948) drew attention to the degenerative element: ‘more axons are destroyed than generally believed…secondary degeneration is defined by the complete destruction of nerve fibres in the direction of their projection’. James Dawson (1870–1927) in Edinburgh focused on the inflammatory component: ‘sites of predilection are related to the vessels…the majority of areas in disseminated sclerosis arise on the basis of an inflammatory reaction’.
Although implications for the pathogenesis may have been overstated and the dividend never fully realised, one important contribution to concepts on the pathogenesis of multiple sclerosis came from animal models in demonstrating that clinical and histological features reminiscent of the human disease could be transferred in rodents using primed immune cells.
The final piece of evidence substantiating the pivotal role of the inflammation in the pathogenesis of multiple sclerosis followed the introduction of MRI and correlation of the observed changes with various neuropathological features. While not yet complete in terms of each and every component of the inflammatory, glial, neuronal and axonal pathology, what did soon emerge is that the earliest change in the evolving new lesion is leakage of the blood–brain barrier; and that this is associated with intense perivascular lymphocyte infiltration.
By the late 1990s, about a decade after starting to test the immunological doctrine of multiple sclerosis in clinical trials, it could reliably be stated that three mechanisms underlie the natural history of the diseases: inflammatory mediators are responsible for the transient and fully reversible symptoms; demyelination leads to the persistent clinical deficits; and axonal degeneration results in progressive disease (figure 2). Knowledge has since been refined and the gaps are closing on what is not yet understood or adequately managed. Against this background, the question now arises of how will matters advance in the digital age?

The relative contribution of pathological processes across the three phases of the clinical course of multiple sclerosis.
Knowledge in the digital age
The application of digital technology in medicine is set to benefit from two resources. First, building on laboratory methods pioneered in genomics, a range of screening methods will increasingly be used to characterise the epigenome, the proteome, the transcriptome, the microbiome, the virome and the spectra of variation in many other cellular compartments and body fluids. Increasingly these will be comprehensive and free from concerns of quality control. Second, databases involving large numbers of individuals who have been meticulously phenotyped will be created and tapped in order to generate information that is beyond the analytical powers of human agency and necessarily requiring digital methods to detect patterns that lie within these data. Starting with the European Database for MUltiple Sclerosis system introduced by Christian Confavreux (1949–2013), Europe has been prominent in the development of such systems. Several other collective systems are being expanded and used worldwide. By way of example, the MSBase neuroimmunology register now lists details of 71 532 cases, gathered by 678 members working in 143 clinics from 36 countries and has in place 55 sub-studies.
Using these resources, new knowledge will emerge from inductive, deductive and deterministic reasoning. But what are the issues ripe for resolution? As modern essayists have noticed, we are set to live in times that remind us of the ancient metaphor of the hedgehog and the fox, ‘πόλλ' οἶδ' ἀλώπηξ, ἀλλ' ἐχῖνος ἓν μέγα’, told by Archilocus (680–645 BC): loosely ‘the hedgehog is concerned about one big thing and works it out; the fox thinks about many things and modifies its activities accordingly’. Attitudes to what lies ahead vary. At one level the digital age is exciting and sure to deliver convenience, liberation and universal gain as smart technologies accelerate change and provide super-intelligence. But, for others, as a world is created in which there are machines that make machines that make machines that may lack in-built conscience or moral guidance, human agency will be sidelined. Expertise will increasingly be confined to systems and society will have to confront the Faustian deal whereby privacy and intelligibility have been traded for efficiency. The existential risk will loom of an extreme event that takes mankind over a horizon into space where nothing can be understood or influenced. In the language of artificial intelligence, this doomsday situation is termed the singularity catastrophe—a term borrowed from astrophysics to describe the collapse of mass into a state of infinite density, the black hole. Whether one is optimist or pessimist, at the very least some consideration of the immediate future and the implications of digital technology for the ethics of medicine deserve consideration.
Ethics in the digital age
At present the ethics of engaging people in medical research conforms to the ‘conduit—container’ model. This has as its fundamental premise the duty to make clear to individuals what their participation entails and thereby to obtain consent for their involvement. This assumes capacity and respects autonomy. Within reason, those who give consent waive their rights and forfeit any later feelings of regret. Those obtaining consent are protected from blame if unforeseen events unfold. The process is tick-box and primarily serves the needs of legislation. It is endorsed in the General Data Protection Regulations which, among other constraints, enforce the right for human intervention in all decisions, and require that systems using personal data are both accessible and intelligible to registrants. It takes rather little to sense that, as these systems become more and more sophisticated, capacity will increasingly be compromised. Furthermore, as any user of ‘secure’ internet systems will have experienced, anonymity and privacy are not fully protected. Present legislation restricts the use of data if their analysis is deemed potentially intrusive, such as compromising insurance or other privacies. The fertility of databases will become increasingly limited if each new use requires reconsent. Participants not able for whatever reason or unwilling to be reconsented are progressively disenfranchised and the surviving sample of those complying with serial requests increasingly biassed. In short, compliance with legislation and ethics presents considerable difficulties in the digital age as any investigator struggling with current administrative requirements will attest. It may take longer to obtain ethical approval than to conceive, carry out and analyse a study. Faced with so many inhibitions, only the most resolute may persist.
As a consequence, some philosophers and medical ethicists now argue for a more liberal system dubbed the ‘agency’ model of communicative transaction. Here it is the intention to explain the purpose of research that matters rather than the detailed itinerary or slavish transfer of technical information. Without being unduly legislative, this does not abrogate the investigator from responsibility and it calls for a high level of accountability. The agency model recognises that the level of confidentiality applied is sensible but not unduly rigid. Self-evidently a liberal system of this kind based on the nuances of language and interpersonal communication risks paternalism, assumes surrogate capacity, requires high professional standards and is founded on trust. Under such a system, the artificially intelligent machine would have difficulty obtaining informed consent.
Knowledge and multiple sclerosis in the digital age
Inductive reasoning is well placed to tackle big but simple questions such as the identification of susceptibility factors. Deductive reasoning is applicable to unravelling the focused but more nuanced issues of pathogenesis. Success with discovering new treatments requires the deterministic approach. Putting the important consideration of ethical constraints aside, several issues that currently appear problematic will prove tractable through the use of digital technology. Knowledge relating to multiple sclerosis is set rapidly to advance.
With liberal but responsible use of databases rich in ‘-omic’ information, examination of blood, urine and cerebrospinal fluid will provide liquid biopsies and identify biomarkers that replace existing criteria and diagnose multiple sclerosis well before it has manifested. Quantitative analysis of these fluids will indicate the amount and dynamics of disease activity. No longer will the mysteries of the Lange curve, or the hidden secrets of oligoclonal bands be concealed. Inductive reasoning will identify prognostic clinical and laboratory markers applicable to newly diagnosed cases in order to anticipate the natural history and inform prescribing decisions. The rate at which the ability to image an increasing spectrum of tissue components affected in multiple sclerosis will shrink the gap between neuropathological and radiological detail. Learning what to register and what to ignore, intelligent machines will increasingly scrutinise radiological images and histology to detect features that inform concepts and evolution of the pathogenesis beyond resolution of the human eye. Building on the separation of neuromyelitis optica from the main body of multiple sclerosis and the features of demyelinating disease associated with anti-myelin oligodendrocyte glycoprotein antibodies, and the cross-sectional characterisation of histological subtypes, further heterogeneity of the clinical phenotype will emerge with implications for selection of therapies. And the ambiguous state of knowledge with respect to environmental factors will clarify the role of gender, smoking, Epstein-Barr virus exposure, vitamin D deficiency and obesity; identify as yet unimagined risk factors and triggers; and define epistatic interactions with the genome.
Taking the long view, as artificial intelligence increasingly dominates routine decision-making some will see these developments as certain to iron out errors of the human eye in ‘reading’ laboratory data; and set to remove imperfections arising from the whimsicality of human behaviour that delay diagnosis and introduce inequalities of clinical management. Those who regard medicine as an art in which integrity and experience modulate the interaction between individual patient and physician may be less sanguine as to whether the clever machine will understand what it sees and act in the interest of the individual rather than slavishly obeying the data.
Genomics in the digital age
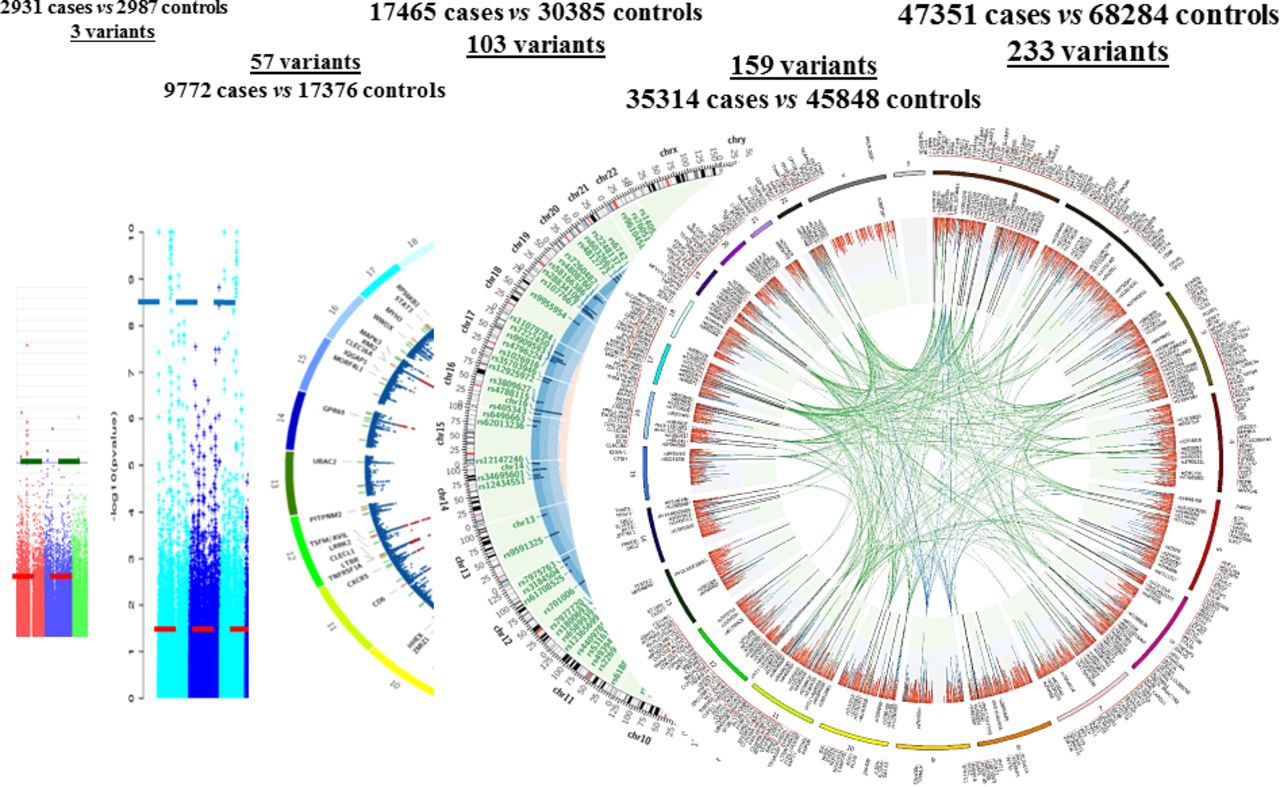
Already a start has been made with genomics. By 2020, the International Multiple Sclerosis Genetics Consortium (IMSGC) had access to 62 616 samples of DNA from patients in 13 countries within Europe, and the USA, Canada, Australia and New Zealand, many of whom had been phenotyped clinically and radiologically. These were matched by an even larger number of controls made available from other databases of people with unrelated medical conditions, and healthy controls. In its first 16 years, as these numbers grew, IMSGC studies identified risk variants that lie within and outside the major histocompatibility complex: three new markers in 2007; a total of 57 in 2011; 103 in 2013; 159 in 2017; and 233 in 2018 (figure 3).
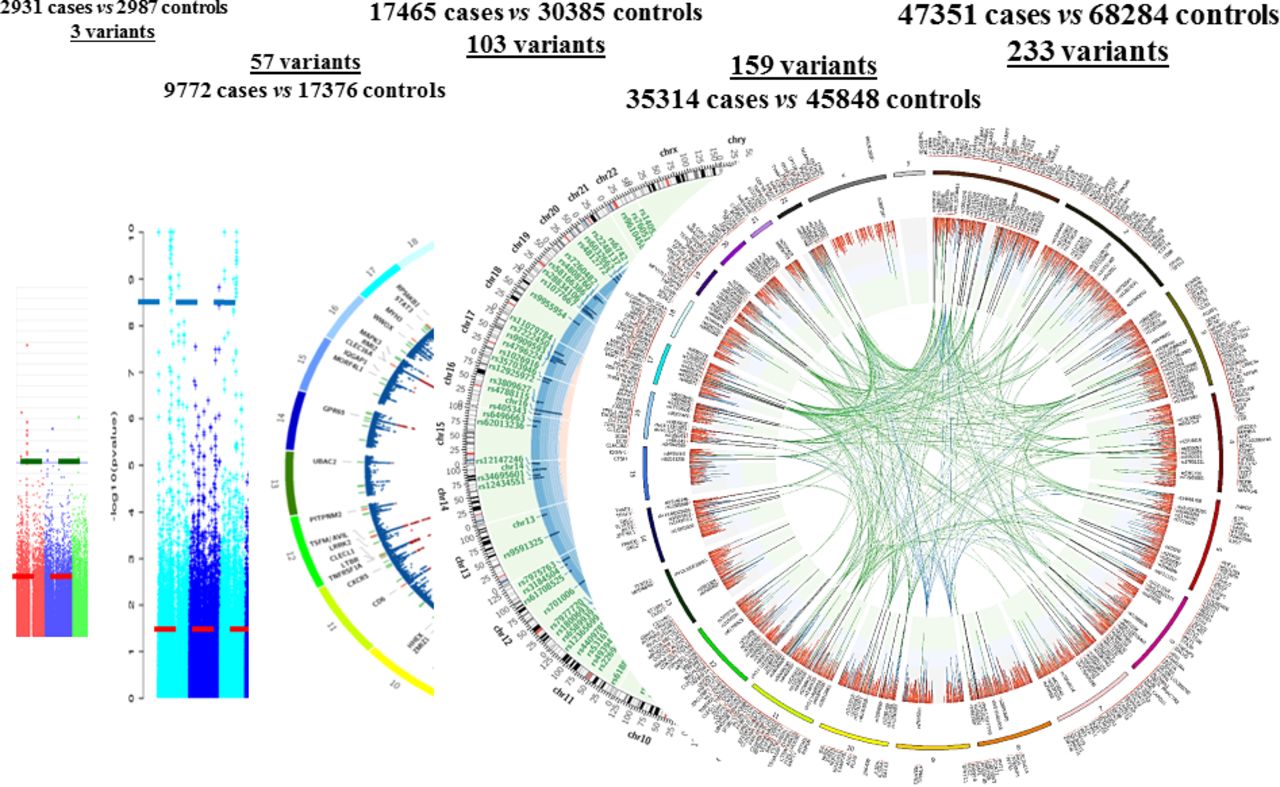
Plots for the list of genetic variants identified as conferring susceptibility to multiple sclerosis from 2005 to 2018.
At an early stage in the evolution of this knowledge it became clear that there is a strong immunological theme to the biological significance of the genes considered to underlie the association of risk variants with multiple sclerosis. By the time that 57 variants had been identified, there was remarkable coverage of implicated genes involved in the proliferation and interaction of cellular components of the adaptive immune system. That principle has broadly been maintained with all subsequent analyses, including the first reliable assessment of minor alleles with frequencies <1% which identified four novel risk variants based on the assessment of 32 367 cases and 36 012 controls from Australia, Europe and USA tested for 118 350 intermediate or rare variants: T cell homeostasis and regulation, IFNγ biology and NFκB signalling were all implicated. Independent pathway analyses using the resource available to IMSGC continue to emphasise the influence on T and B lymphocytes, monocytes and the common components of the adaptive and innate immune repertoire in 47 351 cases and 68 264 controls tested for 538 826 single nucleotide polymorphisms.
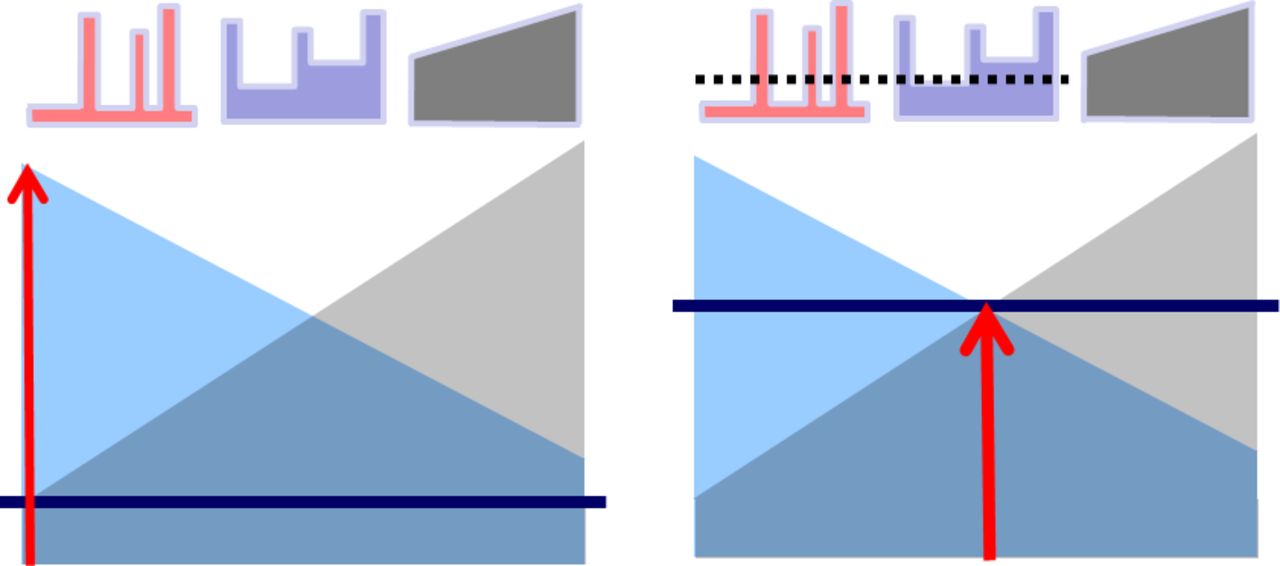
The current IMSGC project focuses on whether there are genetic variants that influence progression and disability. This complements a similar study developed by a Scandinavian consortium that lies within IMSGC (designated ‘MultipleMS’). Three answers may emerge: fully independent risk factors exist for susceptibility and progression; risk factors only confer susceptibility and, depending on the genomic load, these drive disability and progression; risk factors exist independent of susceptibility that vary the threshold for neurodegeneration but require the trigger of an inflammatory insult (figure 4). The last seems most likely but currently lacks evidence: comparison of the 10% with low and 10% with high multiple sclerosis status scores (n=640 of each), and analysis of another 750 cases with extreme phenotypes, aged >60 years and disease duration >10 years, using the Multiple Sclerosis Severity Score as a continuous variable hints at genes affecting severity and the clinical course but without any markers reaching genome wide significance. The present IMSGC experiment will extend these approaches and with much greater power than existing analyses.

The relative contribution of inflammation and axon degeneration in multiple sclerosis. Left panel: in relapsing–remitting disease, the threshold for degeneration is high and it takes a greater degree of inflammation, or longer, to expose the degenerative diathesis. Right panel: in primary progressive multiple sclerosis the threshold for degeneration is much lower and it takes less inflammation to initiate degeneration; or as argued by the late Christian Confavreux, the early parts of the natural history are so shortened as to be amputated from the degenerative phase.
While genetic analysis may illustrate the extent to which digital technology can accelerate the gain of knowledge, many other ‘-omic’ screens are in progress or planned; and there can be little doubt that their analyses, individually and interactively, will open unforeseen windows on the aetiology, mechanisms, heterogeneity and basis for treatment in multiple sclerosis.
Disability in the digital age
Progression correlates with accumulation of disability in multiple sclerosis and patients with physical impairments will be much advantaged in the digital age through the availability of smart technology. Telecommunications and the worldwide web reduce social isolation and maintain employment for those in whom daily travel and physical activity are restricted. In 2020, the relative ease of global home-based communication and its importance in maintaining human contact have been made abundantly clear. Without belittling the losses, impairment, disability and handicap are to some extent subjective experiences conditioned by prior activities, interests and inclinations of the person with multiple sclerosis. If the everyday mechanics of daily living present difficulties, clever devices and aids, including the use of robotic nurses and carers, will increasingly be used to compensate for physical activities. But rehabilitation in the digital age should aspire to more than clever systems for coping. The biology of disability and progression and the impact of regenerative medicine also need to be addressed. Already the cell and molecular basis for progression are being illuminated. The relative roles of adaptive and innate immunity evolve over time with the development of B cell meningeal follicles, an increase in cortical lesions and the impact of mitochondrial abnormalities. These herald gathering momentum of the degenerative process, switch in the course from intermittent to progressive, and the steady accumulation of irreversible disability.
The spread and expansion of cortical receptor zones after damage to their projecting pathways, and molecular changes in ion channel distribution on naked axons that restore aberrant conduction of the nerve impulse, indicate the potential for plasticity and adaptation. Recovery also follows remyelination, first depicted if not fully appreciated in 19th century Paris and shown to restore conduction and function in an experimental context in the 1970s and beyond. These studies brought into focus work on the cellular architecture of the central nervous system pioneered by Rudolph Virchow (1821–1902), Santiago Ramon y Cajal (1952–1934), Camillo Golgi (1843–1926) and Richard Bunge (1932–1996). In 1983, Martin Raff described methods for culturing in vitro cells of the glial lineage and, from his laboratory and elsewhere, followed description of oligodendrocyte precursors in the adult rodent and human nervous systems and the demonstration of their accumulation but suspended behaviour in the lesions of multiple sclerosis.
Increasingly, the principles emerging from work on cellular and molecular features of the evolving lesion in multiple sclerosis are being formulated into potential therapies. Until now, the focus has been on suppressing a pivotal step in the disease process: a necessary but not sufficient ideal. For at least two decades, patients, their advocates and researchers have aspired to the more ambitious aim of both limiting and repairing the damage. The two may not be unrelated. Remyelination is likely to be a multistep process: protection from further waves of injury, clearance of debris, preparation for repair, proliferation and differentiation of oligodendrocyte precursors, engagement with axons and wrapping with new myelin. Loss and gain of myelin, depicted by alterations in the magnetisation transfer ratio, has been claimed for drugs currently licensed or being evaluated in the treatment of relapsing–remitting multiple sclerosis: natalizumab, alemtuzumab and pioglitazone. Yet more promising is evidence for reduction in the latency of visual evoked potentials, extrapolating evidence from animal models, in association with remyelination using clemastine (an anti-histamine with anti-muscarinic activity). Other medicines are being assessed for the ability to promote remyelination: anti-LINGO, fingolomod, nimodipine, metformin with or without fasting, bexarotene and nanocrystalline gold.
The hurdle may not be impossibly high if all that is needed is to nudge endogenous remyelination in the right direction. There is evidence that therapies, such as alemtuzumab and autologous haemopoietic stem cell transplantation, which deplete lymphocytes and allow replacement with a reconstituted immune cell repertoire create an environment which, at least in vitro, shifts the maturation of oligodendrocyte precursors towards a myelinating phenotype and makes available supernatants containing growth factors that increase neuronal survival and axonal growth.
But a strategy that addresses both reduction in the immunological insult and increased restoration of myelinated axons with secure conduction may still miss useful therapeutic opportunities, especially as the disease processes evolve. The distinction between therapies that target cells and mediators of the adaptive and innate immune systems, those that act systemically and drugs that reach compartmentalised pockets of tissue destruction will all come into prominence. As the number of approaches taken increases, the list of medicines and interventions for which efficacy is claimed based on one or more studies of varying quality and duration will grow. The story of multiple sclerosis is littered with well-intentioned but extravagant claims for a ‘breakthrough’ in treatment. This enthusiasm must be managed in a measured way so that complementary components of a therapeutic regimen are eventually defined that take on each and every vulnerable point in the pathogenesis of multiple sclerosis.
Personalised medicine in the digital age
It follows that the main deterministic challenge for multiple sclerosis in the digital age is to apply emerging knowledge to patients and personalise medicine so that, rather than decisions based on group effects, prescription is linked to biomarkers that predict enhanced efficacy and reduced morbidity for the individual. The concept is not new. William Osler (1849–1919) wrote: ‘The good physician treats the disease; the great physician treats the patient who has the disease’. Douglas Black (1913–2002) argued that ‘medicine is for the individual’ and he expounded the philosophy that what can be done is not necessarily what should be done. It will be for immunologists to dissect in more detail the cellular intricacies of the adaptive and innate immune response and to determine which cell type should ideally be targeted, alone or in combination, to achieve a sufficient therapeutic response. But whatever emerges from these deductive studies will need to be evaluated in deterministic clinical trials that raise the bar on efficacy already achievable using the more potent end of the disease-modifying therapy spectrum, and take as their outcomes complete and prolonged suppression of disease activity with reversal of existing disabilities. This will require a shift in strategy that neurologists have been slow to adopt.
The available evidence already indicates that it makes poor sense to start with modestly effective medicines and delay scaling-up until these are demonstrably insufficient and patients irretrievably committed to progressive disability. The mantra should be: ‘to wait is too late’. It is equally illogical to expect that neuroprotective therapies (once these have been identified) will stabilise or prevent disability without also suppressing inflammatory disease activity. Much better is a strategy that starts with treatment sufficient to interrupt core mechanisms and stop disease activity, complemented by maintenance therapies, neuroprotection and encouragement of remyelination (figure 5). Probably nothing short of this combination approach, replacing escalation with induction, and addressing both the inflammatory and consequential neurodegenerative components will radically alter the long-term prognosis. The fate of Augustus d’Este (1794–1848), grandson of King George III of England (1738–1820), who, starting in 1822, first documented the inexorable progress of his disease from transient loss of vision to paralysis and dependence on others for all aspects of daily, needs routine relegation to the archives of history.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A future strategy for immunological treatment of multiple sclerosis: escalation followed by neuroprotection versus induction combined with maintenance and neuroprotection as combination therapy.
Knowledge and communication in the digital age
Knowledge is formulated and communicated as language. The world changed on 15 November 1454 when Johannes Gutenberg (1400–1468) first printed using movable type. Society moved on again in June 1978 when Seymour Rubinstein and Rob Barnaby allowed ‘everyman’ to be his or her own printer through the introduction of the MicroPro International Inc, Wordstar system. Smart technology now provides vocabulary and a thesaurus, improves semantics and syntax, suggests the vernacular and translates. It may struggle more with literary style including the judicious use of analogy, allegory, metaphor, proverb, rhetoric, prosody and imagination; and it may be some time before everyone laughs out loud at an intelligent machine’s sense of humour. Sir William Gowers (1845–1915) had a dry wit as illustrated by his son Ernest (1880–1966) recalling an American postgraduate student who spent a 3-month elective period at the National Hospital in London. When the visitor left for a month of further study in Vienna, he told Gowers that he planned to study disseminated sclerosis. Gowers responded that this was a topic he had been studying for 35 years, and he would be grateful if the young man would send him a postcard in due course with news of all he had discovered.
Information is evanescent and unstable, what is known being added to and forgotten in equal measure. The digital age will accelerate the availability of information and machine learning will use data to deduce knowledge. The use made of that knowledge involves human agency. The slavish work may be delegated, and hands-on physical work increasingly mechanised. Print may reduce as language is codified in yet more sophisticated and rapidly transferable systems. Thoughts may be sensed and transmitted. The opportunities and efficiencies of experimental and therapeutic medicine will undoubtedly benefit from these advances. But beyond inductive, deductive and deterministic reasoning, the currency of imagination, judgement, integrity, altruism and social conscience on which humanity depends will not go away. And for all the wizardry of the digital age, the person with multiple sclerosis will continue look to people practiced in the art of medicine for comfort and wisdom.
Acknowledgments
This article is based on the ECTRIMS Lecture given in Berlin on 10 October 2018. Many details are mentioned but in the interests of space not individually referenced. The missing citations will already be well known to readers of the journal and readily available from electronic sources. But it would be remiss not to mention the following: discussions with Professors Alasdair Coles, Robin Franklin and Stephen Sawcer; the work of the International Multiple Sclerosis Consortium especially the projects led by Phil de Jager, Stephen Sawcer, Chris Costapas and Sergio Baranzini; the several contributors to McAlpine’s Multiple Sclerosis (2005) and its six predecessors (1954–1998); George Henry Lewes, The history of philosophy (1867); Neil Manson and Onora O’Neill, Rethinking informed consent in bioethics (2007); The Royal Society (2017), Machine learning: the power and promise of computers that learn by example; and recent reviews including AJ Thompson et al, ‘Multiple sclerosis’, Lancet 2018; 391:1622–1636.
Footnotes
Correction notice This article has been corrected since it appeared Online First. Title has been changed from 'Review' to 'Occasional essay'.
Contributors The paper was conceived and written by the author with no other people involved other than those acknowledged.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.