Article Text

Abstract
Migraine and stroke are two common and heterogeneous neurovascular disorders responsible for a significant burden for those affected and a great economic cost for the society. There is growing evidence that migraine increases the overall risk of cerebrovascular diseases. In this review, based on available literature through a PubMed search, we found that ischaemic stroke in people with migraine is strongly associated with migraine with aura, young age, female sex, use of oral contraceptives and smoking habits. The risk of transient ischaemic attack also seems to be increased in people with migraine, although this issue has not been extensively investigated. Although migraine appears to be associated with haemorrhagic stroke, the migraine aura status has a small influence on this relationship. Neuroimaging studies have revealed a higher prevalence of asymptomatic structural brain lesions in people with migraine. They are also more likely to have unfavourable vascular risk factors; however, the increased risk of stroke seems to be more apparent among people with migraine without traditional risk factors. The mechanism behind the migraine-stroke association is unknown. In light of the higher risk of stroke in people with migraine with aura, it is important to identify and modify any vascular risk factor. There is currently no direct evidence to support that a migraine prophylactic treatment can reduce future stroke in people with migraine.
- migraine
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Migraine is a common primary headache disorder, affecting up to 20% of the general population.1 The incidence of migraine increases after the onset of puberty with an earlier age of onset in women. Approximately 90% of all patients have their first attack before the age of 50 years. Up to a third of those with migraine experience aura before or during an attack, characterised by reversible neurological symptoms, most typically visual disturbances but also sensory, language, brainstem or motor symptoms. Stroke is characterised by a sudden onset of neurological deficit of vascular origin typically occurring after the age of 50 years.2 3 Migraine and stroke differ widely regarding gender preponderance, age of onset, clinical presentation, outcome and treatment; however, accumulating evidence suggests that migraine is a risk marker for stroke. As migraine and stroke are common disorders, an association between the two conditions imposes substantial burdens on society.
We have reviewed available literature on the association between migraine and stroke, the possible underlying mechanisms and the clinical implications of this association.
METHOD
We searched PubMed without language restriction from 2011 up to March 2019, with the following search terms; ‘migraine AND (stroke OR ischaemia OR hemorrhagic OR cerebrovascular disease OR brain infarct OR transient ischaemic attack OR intracranial hemorrhage OR subarachnoid hemorrhage)’. This identified 1490 full-text articles. A subsequent exclusion process was done based on language (11 articles excluded), titles (821 articles excluded) and abstracts (164 articles excluded). Furthermore, the reference list of identified articles was cross-examined for relevant papers. The results from systematic reviews were preferentially reported to avoid repetition of data. In addition, relevant, original research studies were added, when necessary.
MIGRAINE AND STROKE
Migraine and the risk of ischaemic stroke
Numerous studies, including five meta-analyses,4–8 have linked migraine, particularly migraine with aura (MA), with increased risk of ischaemic stroke (table 1). The relative risk of ischaemic stroke is doubled in people with MA compared with migraine-free individuals. The risk of ischaemic stroke associated with migraine without aura (MO) is uncertain. The association between migraine and ischaemic stroke is stronger for women, women younger than 45 years, women who use oral contraceptives and women who smoke.4 5 9 Because the prevalence of migraine is three times lower in men than in women, the association is more uncertain for men.5 The risk is greater for those with active migraine (ie, migraine attack the last 12 months)10 and higher frequency of attacks9 11; however, there is no conclusive evidence that the severity of migraine attacks influence the risk of ischaemic stroke. Except older people with migraine who are currently smoking,12 migraine does not seem to be a risk marker for stroke in the older population, unless its onset is later in life.13 14 However, longer cumulative exposure to MA, as would be expected with early onset of migraine, is not associated with increased stroke risk in late life. With regard to functional outcome after ischaemic stroke, MA is associated with ischaemic stroke with good functional outcome (ie, modified ranking score from 0 to 1).15–17 The classification of migraine and specifically MA in population-based studies is challenging. However, the consistent findings of the association between MA and ischaemic stroke across various study designs and classification schemes make a systematic bias unlikely.
Summary of relative risk (95% CI) between migraine and ischaemic stroke in five meta-analyses of observational studies
Clinical implication
MA in women younger than age of 45 years and late onset of MA increase the risk of ischaemic stroke. Active migraine and increased attack frequency increase the risk of ischaemic stroke. The relationship between migraine severity and stroke risk is uncertain.
Migraine and the risk of transient ischaemic attacks
Even for experienced neurologists, a differentiation between migraine aura and transient ischaemic attack (TIA) is often challenging. This is particularly true for patients aged >60 years among whom TIA occurrence increases, whereas attacks of MA are more likely to become more atypical because they are not always followed by migraine headache.18 The sudden onset of TIA symptoms paired with the presence of vascular risk factors is the strongest difference from MA, which has a more gradual-processing occurrence of symptoms. The presence of a headache after transient neurological symptoms does not necessarily mean that these symptoms are consistent with a diagnosis of MA, because a migraine-like attack (with or without aura) can also be triggered by ischaemic vascular events.19 Although not extensively investigated, the risk of TIA seems to be increased in people with MA, but not in those with MO.20 Misdiagnosis of migraine aura as TIA may represent a limitation in the proper study of this association.
Clinical implication
A more detailed clinical workup is recommended for patients with known MA in whom their aura symptoms differ, are atypical or are accompanied with clinical signs of involvement of the basilar artery. The threshold for definitive tissue imaging of such patients with MRI should be low.
Cerebrovascular events triggering a migraine
The association between migraine and stroke is complicated by the fact that almost any cerebrovascular event (ie, ischaemic stroke, haemorrhagic stroke, subarachnoid haemorrhage, venous thrombosis) can trigger a migraine-like attack (with or without aura), which may lead to misinterpretation of the stroke event as ‘complicated migraine’.18 The increased frequency of migraine aura in later life may be the symptomatic expression of an underlying stroke risk factor (eg, hemosiderin deposition, arterial emboli, cardioemboli) rather than the aura itself increasing the risk of stroke.21–23 Most studies, particularly prospective studies, collect information on migraine status before the vascular event, and thus is not the mechanism behind the migraine-stroke association.
Migraine and the risk of haemorrhagic stroke
Several studies have evaluated the possible link between migraine and haemorrhagic stroke,8 15 17 24–26 and although some studies fail to find any association,5 7 27 there is increasing evidence suggesting that there is an association,8 15 17 24–26 particularly in women younger than 45 years.24 Although some studies found increased risk in people with MA,8 15 25 there is overall not sufficient evidence that the risk of haemorrhagic stroke is particularly increased for MA.17 24 26 The association between the use of oral contraceptives and haemorrhagic stroke in women with migraine is more uncertain.28 29 Due to very low number of outcome events, it is challenging to study the association between migraine and the different subtypes of haemorrhagic strokes (ie, intracerebral haemorrhage and subarachnoid haemorrhage). In contrast to ischaemic stroke, which is associated with strokes that result in low grade of functional impairment, haemorrhagic stroke suggests a stronger link with fatal events.25
Clinical implication
While women under the age of 45 years may be at increased risk of haemorrhagic stroke, the overall relationship between migraine and haemorrhagic stroke and the specific relationship between migraine subtypes and haemorrhagic stroke are uncertain.
MIGRAINE AND RISK OF CARDIOVASCULAR DISEASE
There is growing evidence of an association between migraine and other cardiovascular disorders including myocardial infarction, hypertension, venous thromboembolism and atrial fibrillation (AF),8 15 21 30–33 with stronger association in people with MA. An association between migraine and cardiovascular disease mortality has also been found.31 34 While the annual cardiovascular mortality risk for migraine is relatively low, the risk may accumulate when magnified across decades of individual migraine exposure.35 The QRISK3 algorithm was recently developed and validated to predict 10-year risk of cardiovascular disease in men and women aged 25–84 years.36 Migraine being included in this algorithm indicates its importance in the risk prediction of cardiovascular disease.15 Although evidence for a link between migraine and cardiovascular disease exist, it is still unclear whether migraine itself increases the risk or is a marker of another underlying cause. Improvement of aura with aspirin37 and migraine with warfarin38 has been observed in observational case studies; however, further research is necessary to confirm these effects. There is no evidence that controlling migraine attacks with preventive drugs can reduce cardiovascular risk.
Clinical implication
Current migraine guidelines do not recommend use of antithrombotic drugs in the prophylaxis of migraine, but clinicians should consider whether patients at particularly high risk of cardiovascular disease would benefit from such treatment.
MIGRAINE AND VASCULAR RISK FACTORS
The role of conventional vascular risk factors on the risk of cardiovascular events in people with migraine is controversial. Migraine, and particularly MA, is associated with an unfavourable cardiovascular risk profile and an increased 10-year predicted risk of coronary heart disease based on the Framingham Risk Score.39–41 Frequent headache and long-term migraine are associated with a poorer cardiovascular risk profile.40 Although people with migraine have an increased risk of ischaemic stroke in the presence of vascular risk factors, several studies have shown that the association between migraine and ischaemic stroke is apparent in people with low Framingham Risk Score.39 40 42 The few exceptions were a positive association with family history of cardiovascular disease, cigarette smoking and oral contraceptives.42 This agrees with reports that coronary and carotid arteries of individuals with active migraine are found to be less severely affected by atherosclerosis than individuals without migraine,43–45 suggesting a non-atherosclerotic mechanism behind the MA-ischaemic stroke link.
Clinical implication
Most migraine patients have MO and are of no or little increased risk of stroke, and they should be reassured instead of being frightened.46 People with MA are at increased risk of developing cardio/cerebrovascular disease, and while migraine prevention in people with MA has not been shown to reduce stroke risk, management of vascular risk factors in those with MA is important in reducing stroke risk. Comorbidities should be treated adequately (arterial hypertension, diabetes mellitus and dyslipidaemia). Migraine patients with aura should be advised to stop smoking, particularly if they also take oral contraceptives. Oral contraceptive use should be carefully discussed in women with MA because of the increased vascular risk. Their prescription should be contraindicated in women with MA and other comorbid vascular risk factor or congenital or acquired thrombophilia.47
MIGRAINE DRUGS AND RISK OF STROKE
Triptans and ergot alkaloids, two effective acute migraine treatments, have vasoconstrictive properties that may potentially increase the risk of serious ischaemic vascular events, including stroke.48 Available data link ergotamine overuse with increased risk of cardiovascular and cerebral ischaemic events, particularly in patients with pre-existing cardiovascular disorders who overused the drug.48 While there is no evidence to support cardiovascular safety issues for triptans,48 even not in patients with overuse, caution must be exercised when considering the use of triptans in patients with risk factors for cardiovascular disease and especially in those with established CV disease.49 It should be noted that the association between migraine and stroke is mainly driven by MA, while migraine specific drugs are used by people with migraine regardless of aura status. For these reasons, use of migraine specific drugs is unlikely to explain the increased stroke risk in migraine.50
Clinical implication
Clinicians should evaluate the baseline cardiovascular risk of patients before initiating migraine-specific medications. Ergotamines should not be used in patients with a history of ischaemic stroke, or any history of cardiovascular disease. Triptans, according to the label, are contraindicated in patients with stroke or TIA, as well as in unstable angina or after acute coronary syndrome.51 While there is limited evidence of their safety in patients with vascular disease and risk factors for CV disease, caution, clinical judgement and full disclosure to patients about the risk and mechanism of the risk must be communicated.48 Novel migraine-specific acute drugs, such as calcitonin gene-related peptide (CGRP) receptor antagonists and the serotonin-1F receptor agonists, whose mechanism of action involve modulating pain circuits, are promising because they cause less or no vascular side effects.52 There is currently no direct evidence to support that a migraine prophylactic treatment will reduce future stroke risk.20 53
MIGRAINE AND RISK OF PERIOPERATIVE STROKE
Perioperative stroke, defined as stroke occurring within 30 days of surgery, is a highly relevant surgical complication, associated with increased mortality rates and serious long-term morbidities. Patients with migraine receiving surgery under general anaesthesia are found to have a higher 30 day risk of ischaemic stroke than those without migraine (adjusted OR 1.75, 95% CI 1.39 to 2.21), suggesting that migraine should be included in the risk assessment for perioperative ischaemic strokes.54 The association between migraine and perioperative stroke was strongest in patients with MA and in those without cardiovascular risk factors. Surgical patients with migraine are also more likely to be readmitted to the hospital, most of these readmissions appear to be related to pain.55
Clinical implication
Physicians should know of the increased risk of perioperative ischaemic stroke in patients with migraine, and include migraine in the preoperative risk assessment.
MIGRAINE AND NEUROIMAGING
Cerebral blood flow
Characteristic perfusion patterns have been identified in people with MA, with perfusion deficit not limited to a specific vascular territory and only a moderate increase in time to peak. This contrasts to the findings in acute ischaemic stroke, which is characterised by hypoperfusion restricted to a single vascular territory in combination with a marked increase of time to peak.56 Compared with controls, people with migraine have been found to have higher parenchymal cerebral blood flow in the migraine attack-free period, particularly basilar artery flow, supporting the presence of sustained vascular differences in patients with migraine even outside of a migraine attack.57 Some studies have reported a higher frequency of incomplete circle of Willis in people with migraine compared with controls,58 in particular for the posterior circulation and in patients with MA, while others have failed to find this association.59 60 Arterial spin labelling is a new MR sequence increasingly being used in clinical practice to differentiate MA from stroke. It assesses brain perfusion without contrast injection, and can therefore be used to evaluate children, pregnant women or to perform serial imaging.61 Migraine have been found to increase individual vulnerability to ischaemic stroke during the process of acute brain ischaemia, and might represent a potential new therapeutic target against occurrence and progression of the ischaemic damage.62
Clinical implication
Although new imaging techniques have emerged, they are not part of routine diagnosis in people with migraine.
Silent structural brain lesions
Migraine is not considered to have long-term consequences for brain function,63–65 and current guidelines suggest that people with migraine with a normal neurologic examination does not require routine MRI. Only for patients with atypical headache, a recent change in headache pattern, other symptoms (such as seizures) or focal neurologic symptoms or signs, MRI of the brain is recommended. A source of concern for both physicians and patients are clinically silent structural brain lesions that are often revealed on MRI. These lesions are not specific to migraine, and the exact aetiology and clinical significance remain uncertain.66–68 Neuroimaging studies indicate that migraine is a risk factor for silent brain lesions such as white matter hyperintensities (WMH) and silent infarct-like lesions (table 2).66 67 69–74 Data point towards a clear association with MA, whereas the link to MO is more controversial.66 69 70 75 Some studies have also failed to find any association between MA and silent brain lesions.76 77 Traditional cardiovascular risk factors and specific antimigraine medication do not modify the association between structural brain lesions and migraine.67 75 Comparison of data across different studies is difficult, as different definitions of silent brain lesions are used, a clear distinction between migraine subtypes may be difficult, and migraine-related variables such as attack frequency, duration and type of aura are not always reported.
Key studies reporting risk of silent structural brain lesions in people with migraine
White matter hyperintensities
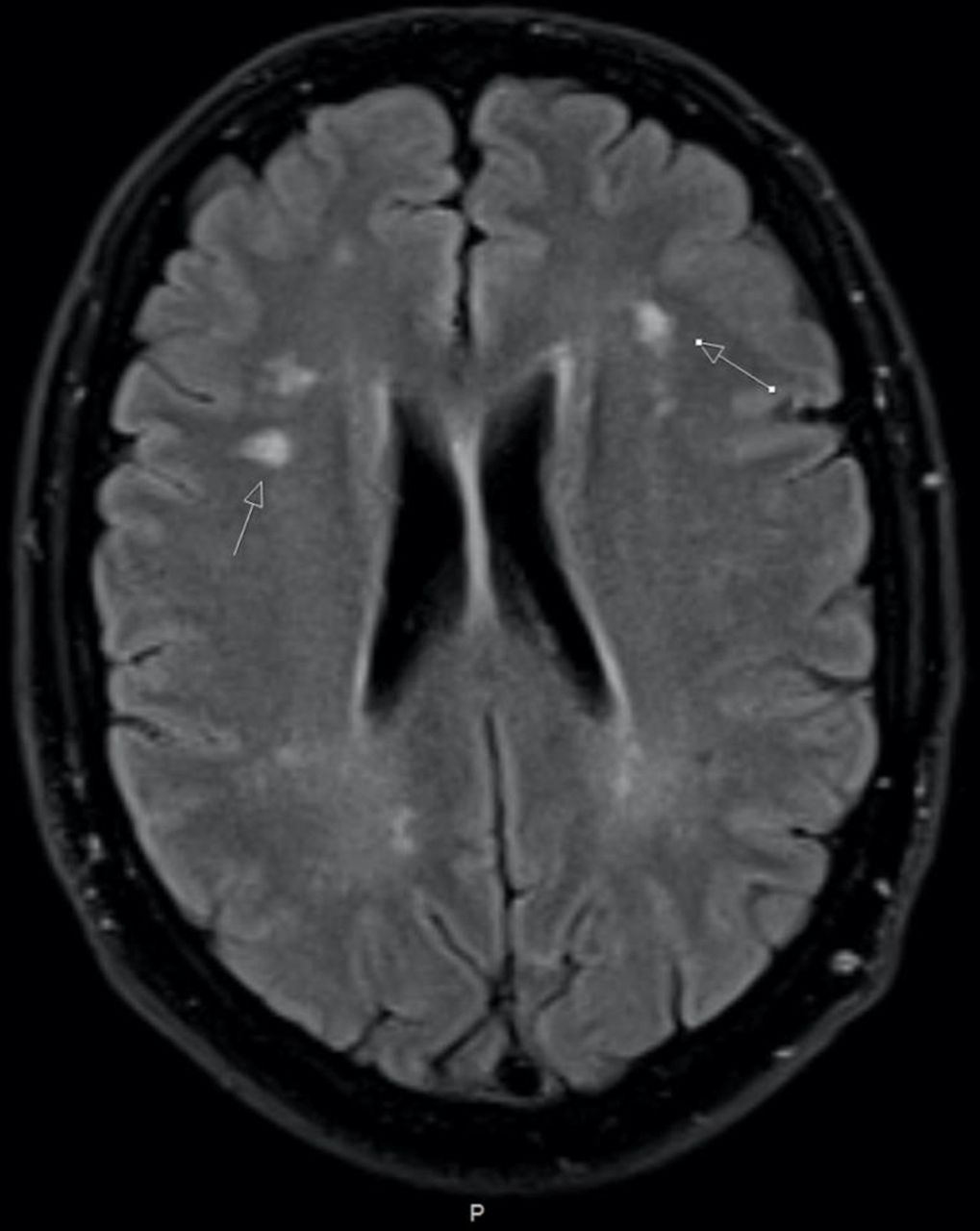
White matter hyperintensities (WMH) are typically multiple, small punctate hyperintensities in deep or periventricular white matter, often seen on T2-weighted images (figure 1) .63 Several studies have found increased risk of WMH in people with migraine,66 67 70 74 78 with higher risk in those with more frequent and severe attacks.66 74 The relationship between WMH and type of headache is uncertain, as some studies have found increased risk of WMH in people with severe headache (migraine and non-migraine headache),70 79 others have found increased risk for women with any migraine (MA and MO)66 78 and others for MA only.67 There are also studies that have failed to find any association between MA and WMH.73 The presence of WMH is associated with several haemodynamic parameters, including increased central blood pressure, greater aortic stiffness and decreased resistance in intracranial arteries.74 80 The impact of migraine on structural brain lesion progression over time is uncertain, as studies on this association show conflicting results.71 72 Although WMH have been associated with increased risk of stroke, dementia and death,63 results from longitudinal studies show no increased risk of cognitive decline in people with migraine (both MA and MO).64 70 71 81
{kind=link}
Multiple white matter hyperintensities in a patient with migraine with aura seen on fluid-attenuated inversion recovery magnetic resonance image.
Silent infarct-like lesions
Silent infarct-like lesions are MRI or CT signal abnormalities defined as non-mass brain parenchymal defects with the same intensity as cerebrospinal fluid and without symptoms.82 Overall, silent infarct-like lesions are reported as being more common in people with migraine than controls,67 particularly for MA. There is an increased risk of silent infarct-like lesions in the posterior circulation territory, particularly in the cerebellum.69 75 83 Some studies also report silent infarct-like lesions in individuals with migraine located outside the cerebellum.70 73 Despite the elevated risk of ischaemic lesions in the cerebellum, people with migraine are found to have normal cerebellar functions.65 Migraine is not associated with the progression of infarct-like lesions over time.71
Clinical implication
Despite the association between MA and silent structural brain lesions, the mechanisms and practical consequences remain unclear. It is unknown whether presence of these lesions increases the likelihood of a subsequent stroke event among patients with MA. Currently there is no evidence that structural brain lesions require different treatment or prophylactic strategies for patients with migraine and stroke.
Unruptured cerebral aneurysms
Uncertainty exists regarding the association between unruptured cerebral aneurysms and their role in headache aetiology. It is estimated that 3%–6% of the population over the age of 30 has an intracranial aneurysm, most often asymptomatic.84 Current evidence suggest that the 1-year prevalence of MO is significantly higher in patients with unruptured intracranial aneurysms than in controls.85 86 Shared genetic mechanisms and common cardiovascular risk factors, such as hypertension and smoking, might play a role in the association between migraine and unruptured cerebral aneurysms.84
Clinical implication
Data on the safety treatment of migraine with triptans and ergotamines in the setting of unruptured cerebral aneurysms are limited. It appears that much of the hesitancy and concern is excessive and unwarranted.84
Reversible vasoconstrictor syndrome
Reversible vasoconstrictor syndrome (RVCS) is a rare, but an increasingly recognised clinical radiological syndrome, characterised by severe acute headache and multifocal constrictions of cerebral arteries, resolving spontaneously within 3 months. The clinical hallmark is severe, often recurrent thunderclap headache that may be isolated or associated with seizures and transient or persistent focal deficits.87 Brain imaging may be normal or reveal cortical subarachnoid haemorrhage, intracerebral haemorrhage, arterial dissection, ischaemic stroke or posterior reversible encephalopathy syndrome. It mainly affects young adults with a strong female preponderance. Whether migraine increases the risk of RVCS remains unknown, but a prior history of migraine is frequently reported in subjects with RVCS.
Clinical implication
Although most people with migraine will never have an episode of RVCS, this vascular condition can manifest with isolated headache that can be easily mistaken for a severe migraine attack, and with aura, secondary to the vascular condition.87 Advances in neuroimaging have facilitated an earlier and more accurate diagnosis, but the role of the physician is crucial in identifying among many people with headache, those who require more extensive investigations.
SMART syndrome
Stroke-like migraine attacks after radiation therapy (SMART) syndrome is a rare, reversible neurologic complication that appears months to years after radiotherapy of brain tumours.88 It is characterised by migraine-like headache, seizures and subacute hemispheric neurological impairment. The typical MRI findings are increased T2 hyperintensity in previously radiated location and gyral gadolinium enhancement in the same region evident within 1 week of neurological symptoms.89 Usually it affects the temporoparietooccipital regions, suggesting these areas may be more vulnerable to radiation than others. SMART syndrome is most often seen in young adults, but may occur in both adults and children. The condition is usually self-limiting and gradually resolves over the course of several weeks.
Clinical implication
As clinical and radiological features of SMART syndrome might be confused with recurrent tumour or subacute stroke, clinicians should be able to recognise this complication as a timely diagnosis can avoid unnecessary testing and alleviate patient anxiety.
MIGRAINE, STROKE AND SPECIAL CONCERNS IN WOMEN
Migraine is a predominantly female disorder, affecting women with a ratio of approximately 3:1 to men. The highest 1-year prevalence of migraine is between ages of 25 and 55 years, and it is estimated that 22%–37% of women will experience migraine during their reproductive years.28 As the association between migraine and ischaemic stroke is particularly strong in women with MA under the age of 45,42 certain aspects during a woman’s life need to be considered.
Migraine and oral contraceptives
Migraine is particularly prevalent in the fertile period when women opt for oral contraception. While the risks of venous thromboembolism in users of oral contraceptives are well established, the risks of cardiovascular arterial diseases are more uncertain.90 The safety of oral contraceptives in women with migraine remains controversial. Numerous studies report increased risk of ischaemic stroke in women with migraine who use oral contraceptive.28 Stronger associations are found for MA and in those with additional vascular risk factors.91 Particularly smoking combined with the use of oral contraceptives in young women with MA increase risk of ischaemic stroke.9 The risk of stroke in women taking oral contraceptives seems to correlate with the dose of oestrogen contained in the formulation.92 93 Caution should be warranted when interpreting the data on the risk of stroke in women with migraine using oral contraceptives28 94; as migraine is often not diagnosed according to ICHD criteria, many studies do not distinguish between MA and MO, and the dose classification of oral contraceptives is often heterogeneous. Studies evaluating the effect of oral contraceptive use on the risk of haemorrhagic stroke is conflicting, and no firm conclusions can be made.28 29
Clinical implication
For most women, modern oral contraceptives are safe and highly effective methods of contraception. Despite the overall low risk of stroke from oral contraceptives, certain subgroups of women, particularly those who have MA, are older than 35 years, smoke cigarettes or have other stroke risk factors, may be at higher risk.90 One should look for an underlying genetic or acquired coagulopathy in those with previous thromboembolism or risk factors for an underlying coagulopathy (eg, family history of thromboembolism, spontaneous abortion, history of malignancy). Type of oral contraceptive should also be taken into consideration, as the oestrogen content differs between products. New onset of migraine aura, new onset MO in temporal relationship to starting oral contraceptive, development of unusual aura symptoms or prolonged aura may necessitate further evaluation or cessation of oral contraceptives.
Migraine and pregnancy
The physiological changes during pregnancy, such as venous stasis, oedema and hypercoagulability, combine to make pregnancy and postpartum period a time of increased risk of stroke.95 While most women experience improvement of migraine during pregnancy,94 migraine attacks may worsen or develop de novo in a small percentage. Women with menstrual migraine are more likely to experience improvement since the triggering factor (oestrogen fluctuation) is absent during pregnancy.91 The worsening usually occurs in the first trimester, and involves women suffering from MA rather than MO. Also de novo migraines during pregnancy mostly consist of MA.91 Women suffering from migraine are at increased risk for several complications during pregnancy including preeclampsia, gestational hypertension, pulmonary embolism, venous thromboembolism and cerebrovascular event such as ischaemic stroke and cerebral haemorrhage.96 97 Pregnant women with migraine are more likely to have vascular risk factors, including hypertension, diabetes and smoking.97 The risk is particularly evident in those women not showing remission or amelioration of migraine attacks.96
Migraine and hormone replacement therapy
There are insufficient data to support a further increased risk of ischaemic stroke in women with any type of migraine who are using hormone replacement therapy.91
Clinical implication
After menopause, MA in itself is not a contraindication for the use of hormone-replacement therapy, but stroke risk related to the therapy itself should be considered.98
POTENTIAL MECHANISMS LINKING MIGRAINETOSTROKE
The precise mechanisms by which migraine is linked to stroke are unknown and possibly multifactorial.
Cortical spreading depression
The migraine aura is central to the association between migraine and stroke since the increase in the relative risk of ischaemic stroke is doubled only in MA, in most studies. Cortical spreading depression, the electrophysiological mechanism believed to underlie migraine aura, is an intense depolarising wave of neuronal and glial membranes that spreads slowly across the cerebral cortex.99 In cortical spreading depression neuronal activation is accompanied by brief hyperperfusion that lasts for 1–2 min, followed by neuronal suppression and hypoperfusion that persist for 1–2 hour and corresponds to a 20%–30% reduction of cerebral blood flow.100 Under normal circumstances, the reduction of cerebral blood flow is insufficient to cause cell damage; however, on rare occasions, the hypoperfusion may be severe enough to cause ischaemia. The origin of cortical spreading depression in humans remains unclear, but in animals, it can easily be evoked by many acute triggers such as electrical or mechanical stimulation, hypoxia, ischaemia, embolism and various substances including air bubbles, cholesterol, crystals or endothelin.99 101 MA is associated with a lower triggering threshold for cortical spreading depression, making the migraine-susceptible brain more vulnerable to cerebral ischaemia.102
Clinical implication
If results from animal experiments can be translated into clinical practice, drugs suppressing cortical spreading depression may protect people with MA at risk of stroke. A broad range of substances can modulate cortical spreading depression, such as analgesics, sedatives and N-methyl-D-aspartate (NMDA) receptor antagonists, preventive medications and neuromodulation technologies including transcranial magnetic stimulation and vagal nerve stimulation103–106; however, there is currently no evidence that they can prevent stroke in patients with migraine.
Vascular system
Alterations in endothelial and arterial function, which predispose to atherosclerosis and cardiovascular disease, have been suggested as an important link between migraine and vascular disease. However, the available evidence is inconsistent. While several studies support an alteration of arterial function among people with migraine, findings on the endothelial function are more uncertain.101 107 Most studies on markers of endothelial dysfunction also show conflicting results (c-reactive protein, cytokines, nitric oxide, endothelin-1, markers of coagulation and thrombosis, and number of endothelial progenitor cells).108–110 Heterogeneity among the studies might explain the inconsistency, as the studies have different inclusion and exclusion criteria, do not differentiate between migraine status, exclusion of subjects with elevated cardiovascular profile and generally small number of participants. Most studies have a cross-sectional design, and thus, a cause-effect relationship between migraine and the vascular system cannot be established. Migraine usually starts in early adulthood, at an age in which arterial wall pathologies are rare. The evidence of atherosclerosis leading to vascular events is not supported in people with migraine. Time may be an important aspect when evaluating the interplay between migraine, vascular risk factors and cardiovascular disease.111 As migraine is an intermittent disorder with fluctuating frequencies during the lifespan, repeated assessments of the vascular health status might be necessary to assess whether migraine leads to vascular pathologies that eventually increase the risk of cardiovascular disease. It is possible that active migraine is not associated with atherosclerosis in the beginning, but that over time people with migraine have a faster development of vascular pathologies.
Clinical implication
The study of systemic vascular function is a promising tool for non-invasively investigating the vascular health of people with migraine. Elucidating a relationship between the vascular system, migraine and stroke has the potential for generating therapeutic targets that could significantly reduce vascular disease in this population.
Shared genetic factors
The genetic component of migraine is demonstrated by familial clustering of common migraine, and an estimated heritability of 42%.112 A shared genetic susceptibility to migraine and stroke has been reported in genome-wide analysis studies (GWAS), with stronger overlapping for MO than MA, and for large artery and cardioembolic stroke than for small vessel disease.112 113 The genetic overlap does not address the findings from population-based studies, of stronger associations between MA and stroke. GWAS studies have contributed to an increased focus on the vascular components in the risk of polygenic migraine; however, current evidence does not support a strong genetic component for the link between MA and stroke. Several genetic syndromes characterised by the occurrence of both migraine and stroke also suggest a genetic connection. This applies to rare diseases such as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), familiar hereditary migraine, retinal vasculopathy with cerebral leukodystrophy and mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS). Gene mutations possibly increase the vulnerability to stroke by facilitating ischaemic depolarisation.114
Clinical implication
Genetic factors could confer a susceptibility to migraine and stroke; however, these are rare disorders and cannot justify most cases of migraine and stroke. Genetic testing is currently not part of routine diagnostic evaluation for migraine, except in circumstances where migraine may be a presenting or inherent feature of a genetic stroke syndrome such as CADASIL or MELAS.
Specific clinical aspects linking migraine and stroke
Migrainous infarction
According to the International Classification of Headache Disorders version 3 (ICHD-3), migrainous infarction is defined as an attack of prolonged aura (>60 min), with for that patient typical aura symptoms, with neuroimaging signs of an infarct in a relevant area and the stroke is not attributed to another disorder.115 A migrainous infarct is a rare event, comprising only <0.5% of all ischaemic strokes.116 The exact pathomechanism is unknown, but a possible explanation is that decreased blood flow during the aura phase reaches ischaemic levels. Support for this is provided by studies showing that migrainous infarcts are most often located in the posterior circulation, and the reduction in cerebral blood flow associated with visual aura is most prominent in the posterior circulation.75 117 The diagnosis of migrainous infarcts is complicated by clinical and experimental evidence showing that ischaemic cerebral events can trigger migraine-like attacks118 and lead to misinterpretation of the stroke event as ‘complicated migraine’.50 Thus, controversy exist regarding whether a migrainous attack is the cause or a symptom of the ischaemic lesion.
Clinical implication
Migrainous infarction is by definition a diagnosis of exclusion, and should not be diagnosed without an extensive work-up to exclude other causes.
Patent foramen ovale
The foramen ovale may remain permanently open or be functionally open due to transient increases in atrial pressure, causing a right to left shunt. Circulatory bypass of normal pulmonary filtering via patent foramen ovale (PFO) may allow venous blood to communicate directly with the arterial system, which may lead to ‘paradoxical emboli’ and ischaemic stroke. Studies have shown that small particles, air bubbles and substances circulating in the venous blood can cause cortical spreading depression, and it is plausible that PFO might trigger both migraine aura and ischaemic stroke. Several observational studies report that people with MA have a higher prevalence of PFO, and that migraine is more prevalent in patients with PFO.119 120 It is still unclear if there is a causal relationship or a co-existence of these two conditions. Several observational studies suggested that closure of PFO significantly reduces attack frequency in migraine patients121–126; however, three prospective placebo-controlled trials did not support these results.127–129 Spontaneous right to left shunts have been associated with persistence of migraine attacks (MA and MO) beyond the age most patients normally cease having attacks; however, they were not associated with increased risk of ischaemic brain lesions.130 Migraine attacks are likely heterogeneous, and in addition to the phenotype of the headache (migraine with or without aura)129 it has been suggested that physiological factors (ie, size of PFO, presence of right to left shunt at rest and presence of atrial septum aneurysms), and platelet-inhibition effectiveness (thienopyridine responsiveness)131 should be considered when deciding if people with migraine would benefit from PFO closure.
Clinical implication
For young patients with cryptogenic stroke, examination of an existing PFO is part of routine diagnostic evaluation. The decision of PFO closure should be based on stroke prevention and not on potential beneficial effect on migraine. In asymptomatic PFO, primary prevention with antiplatelet drugs is not indicated, regardless if the patient has migraine. Migraine should not be considered an indication for PFO screening, unless there are unusual, atypical or frequent aura symptoms associated with attacks and a personal or family history of thromboembolism.
Arterial dissection
Cervical artery dissection (CeAD) is the most common identified cause of stroke in the young and middle-aged, and it is associated with both migraine and ischaemic stroke. CeAD may trigger secondary migraine attacks, thought to be caused by hypoperfusion or substances released by injured endothelium triggering cortical spreading depression and migraine aura. Common biological pathways have been suggested for migraine and CeAD, including shared genetic susceptibility and endothelial dysfunction.113 The main symptoms of CeAD are cervical pain and headache. In the acute phase, headache seems to be more frequent in people with migraine compared with those without a history of migraine.132 Both migraine and dissection-related stroke patients have in common young age at presentation and relatively few traditional vascular risk factors compared with the general stroke population. The association between migraine and CeAD seems to be stronger for MO, for men and for the younger age groups.133 Among patients with CeAD, being an individual with migraine had no influence on the occurrence of cerebral infarction, on the type of dissection (vertebral or carotid), the number of dissected vessels or on the clinical outcome, or occurrence of complications. In follow-up studies of patients with CeAD, mostly with ischaemic manifestations, people with migraine may experience improvement or even cessation of migraine attacks.87 This may be due to a potential migraine prophylactic effect of aspirin, given as prophylactic treatment after CeAD.
Clinical implication
A diagnosis of CeAD should be considered in people with migraine if they complain of unusual headache features with regard to triggers (exertion, trauma), mode of onset (thunderclap), location (cervical pain) or duration (>72 hours) or unusual aura features. The diagnosis must also be considered in persons without previous migraine history that present with new-onset headache or focal neurological symptoms.
Atrial fibrillation
An association between migraine and AF has been reported in several studies,15 21 with stronger associations in people with MA. The risk of having incident AF was stronger in women in one study,15 and in men older than 60 years in another study.21 As older people with MA seem to have increased risk of cardioembolic stroke,134 it is possible that the stroke is secondary to undiagnosed paroxysmal AF. Several case reports and case series have reported the incidence of AF during a migraine attack, with autonomic dysfunction playing a role in the pathophysiology of both migraine and AF.135 136 The hypothesis is supported by AF ablation procedures that have shown tendencies to reduce migraine symptoms and frequencies.137
Clinical implication
Searching for AF is part of routine stroke work-up. Older people with MA should also be evaluated for paroxysmal AF.
SUMMARY
Migraine and particularly MA have been consistently linked with increased risk of ischaemic stroke. An increased risk has also been observed for haemorrhagic stroke and cardiovascular disease. The precise pathophysiological mechanisms for these associations remain unclear. However, MA is associated with circulating coagulation factors and systemic endothelial dysfunction that may increase the risk of arterial thrombosis and ischaemic stroke. Individuals with migraine, especially with aura, are also at an increased risk of comorbid conditions (eg, PFO) and complications (eg, arterial dissection) that can contribute to or cause ischaemic stroke. Moreover, changes in cerebrovascular reactivity and cerebral ischaemic threshold in people with MA may also increase the risk of ischaemic stroke, especially in circumstances of vascular stress (eg, arterial emboli). At the moment there are no reliable clinical, imaging or serum biomarkers that predict which individuals with migraine are at high risk of experiencing ischaemic stroke. Based on the current evidence, MA should be considered an important risk marker for stroke. Prospective cohort studies in women have also demonstrated that migraine is associated with any cardiovascular disease and cardiovascular mortality. Thus far, no migraine-specific pharmacologic interventions are recommended for the primary prevention of ischaemic stroke in people with migraine. In general, the acute treatment and the secondary prevention measures in patients with a history of TIA or stroke in those with a history of migraine do not differ from those without a history of migraine.
Future directions
Frequent migraine attacks appear to be associated with further increased risk of stroke, and future studies should investigate whether effective preventive treatment of migraine attacks reduce the risk of stroke. The differential effect of various preventive treatments on vascular outcomes (eg, anticonvulsants vs antihypertensive or CGRP monoclonal antibodies) should also be a focus for future research, especially in those with multiple vascular risk factors. It is also important to determine the various causal mechanisms underlying the increased risk of stroke in people with migraine, so that targeted strategies can be developed to prevent cerebrovascular events. We recommend that future studies should use diagnostic criteria for migraine, include aura status, and have clearly defined end-points. Markers of migraine severity, including frequency of attacks and frequency of aura, should be considered in the association between migraine and vascular disease. Prospective registries that deeply phenotype and genotype those with migraine and ischaemic stroke should identify genetic factors that are associated with an increased risk of stroke in subgroups of individuals with migraine.
Footnotes
Contributors LRØ and DWD conceived the study, critically reviewed the literature and drafted the manuscript. TK and SG critically reviewed and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DWD reports the following conflicts: Personal fees: Amgen, AEON, Association of Translational Medicine, University Health Network, Daniel Edelman Inc, Autonomic Technologies, Axsome, Allergan, Alder BioPharmaceuticals, Biohaven, Charleston Laboratories, Clexio, Dr Reddy’s Laboratories/Promius, Electrocore LLC, Eli Lilly, eNeura, Neurolief, Novartis, Ipsen, Impel, Satsuma, Supernus, Sun Pharma (India), Theranica, Teva, Vedanta, WL Gore, Nocira, PSL Group Services, XoC, Zosano, ZP Opco, Foresite Capital, Oppenheimer; Upjohn (Division of Pfizer), Pieris, Revance, Equinox, Salvia, Amzak Health. Speaking fees: Eli Lilly, Novartis Canada, Amgen, Lundbeck. Speakers Bureaus: None. CME fees or royalty payments: HealthLogix, Medicom Worldwide, MedLogix Communications, Mednet, Miller Medical, PeerView, WebMD Health/Medscape, Chameleon, Academy for Continued Healthcare Learning, Universal Meeting Management, Haymarket, Global Scientific Communications, Global Life Sciences, Global Access Meetings, Catamount, UpToDate (Elsevier), Oxford University Press, Cambridge University Press, Wolters Kluwer Health. Stock options: Precon Health, Aural Analytics, Healint, Theranica, Second Opinion/Mobile Health, Epien, Nocira, Matterhorn, Ontologics, King-Devick Technologies. Consulting without fee: Aural Analytics, Healint, Second Opinion/Mobile Health, Epien. Board of Directors: Precon Health, Epien, Matterhorn, Ontologics, King-Devick Technologies. Patent: 17189376.1-1466:vTitle: Botulinum Toxin Dosage Regimen for Chronic Migraine Prophylaxis without fee. Research funding: American Migraine Foundation, US Department of Defense, PCORI, Henry Jackson Foundation. Professional society fees or reimbursement for travel: American Academy of Neurology, American Brain Foundation, American Headache Society, American Migraine Foundation, International Headache Society, Canadian Headache Society.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.