Article Text

Abstract
An increasing number of highly effective disease-modifying therapies for people with multiple sclerosis (MS) have recently gained marketing approval. While the beneficial effects of these drugs in terms of clinical and imaging outcome measures is welcomed, these therapeutics are associated with substance-specific or group-specific adverse events that include severe and fatal complications. These adverse events comprise both infectious and non-infectious complications that can occur within, or outside of the central nervous system (CNS). Awareness and risk assessment strategies thus require interdisciplinary management, and robust clinical and paraclinical surveillance strategies. In this review, we discuss the current role of MRI in safety monitoring during pharmacovigilance of patients treated with (selective) immune suppressive therapies for MS. MRI, particularly brain MRI, has a pivotal role in the early diagnosis of CNS complications that potentially are severely debilitating and may even be lethal. Early recognition of such CNS complications may improve functional outcome and survival, and thus knowledge on MRI features of treatment-associated complications is of paramount importance to MS clinicians, but also of relevance to general neurologists and radiologists.
- multiple sclerosis
- MRI
Statistics from Altmetric.com
Introduction
In the past decades, a number of new and successful disease-modifying treatments (DMTs) for multiple sclerosis (MS) have become available. These DMTs have different modes of action, and some represent a ‘first-in-class’ drug with a long-term safety profile still to be established. As several new drugs are currently in phase 3 trials, the number of available DMTs is likely to increase in the coming years. Recently approved DMTs for MS generally have an immunosuppressive potential that translates into an increasing efficacy, superior in clinical studies to the older injectable platform therapies such as glatiramer acetate or interferon beta.
Selection of DMTs based on potential benefits must be balanced with rare to frequent, and potentially serious, adverse events seen with the newer drugs.1 These adverse events include infectious and non-infectious disorders outside of, but often also involving, the central nervous system (CNS).2 In this review, we present and discuss the current data on the role of MRI in safety monitoring during pharmacovigilance of MS therapies, which aims at the early detection of CNS complications to facilitate the timely initiation of appropriate management and subsequently better outcome.3
The role of MRI in MS
The important role of MRI in the (differential) diagnosis of MS has irrefutably been established.4 With the increasing number of available DMTs for MS, MRI has become an important tool to assess and monitor treatment efficacy. More recently, the role of MRI in patients with MS has expanded to safety monitoring purposes including the detection of infectious and non-infectious adverse events affecting the CNS.3 As such, the application of MRI during pharmacovigilance of MS therapies (which should always be considered in the context of clinical vigilance and paraclinical tests) includes three major aims.
To detect treatment failure/loss of response in clinically stable patients by detecting new or enlarging lesions suggestive of active MS.3
To screen patients at risk of severe adverse events without new neurological symptoms for asymptomatic lesions suggestive of CNS adverse events.
To evaluate patients with new neurological symptoms to rapidly differentiate MS disease activity from CNS adverse events.
This review will focus on the latter two aims, with an emphasis on specific MRI findings that can be essential for diagnosis, as well as on risk factors and clinical signs in different infectious and non-infectious DMT related adverse events (see online supplemental file 1 for search strategy and selection criteria).
Supplemental material
Infectious adverse events
JC virus-associated diseases
JC virus (JCV)-associated diseases include a partially overlapping spectrum of entities, with progressive multifocal leukoencephalopathy (PML) being the most well known. Following primary infection, which is asymptomatic in most healthy persons, JCV remains latent or causes asymptomatic persistent infection in the gastrointestinal tract, kidneys, bone marrow and lymphoid tissue,5 although the relevant reservoir is still unknown. In immunocompromised patients, JCV may cross the blood brain barrier, possibly via infected B-cells,6 and cause a lytic infection of oligodendrocytes, astrocytes and neurons leading to PML.7 In addition, JCV can cause a productive and lytic infection of predominantly granule cell neurons, resulting in cerebellar atrophy and cerebellar symptoms, named granule cell neuronopathy (GCN).8 9 More rare JCV-associated diseases are JCV encephalopathy10 and JCV meningitis.11 Intraindividual acquisition of PML-type variants of the viral genome may be a prerequisite for CNS infection and tropism for oligodendrocytes, astrocytes or neurons during immunosuppression and may explain the different syndromes of JCV-associated diseases.7 12 JCV-associated CNS diseases have traditionally been reported in varied states of immunodeficiency such as HIV/AIDS.13 More recently, PML and GCN have been associated with general and selective immunosuppressive treatments of autoimmune diseases.14 PML can be difficult to diagnose and is often initially misdiagnosed.15
JCV in MS therapies
In MS pharmacovigilance, PML and GCN are the most relevant JCV entities. Among the DMTs, natalizumab is by far the drug most frequently associated with JCV-associated complications. Natalizumab is a monoclonal antibody against the α4-integrin adhesion molecule which inhibits transmigration of immune cells through the blood-brain barrier into the CNS and is used for the treatment of relapsing forms of MS.16 As of 2 March 2020, 832 confirmed cases of natalizumab-associated PML had been reported (>208.354 patients treated).17 PML has also been observed in patients with MS treated with fingolimod, dimethyl fumarate, alemtuzumab and ocrelizumab. As of 1 March 2020, 37 cases of PML have been reported in patients treated with fingolimod (>299 600 patients treated), 10 cases in patients treated with dimethyl fumarate (>445 000 patients treated), and one with alemtuzumab, without prior treatment with natalizumab.18–22 In addition, PML has been reported in patients treated with rituximab (a chimeric anti-CD20 monoclonal antibody leading to B-cell depletion), for example, for haematological malignancies or systemic lupus erythematosus, but not during off-label treatment for MS. In patients using ocrelizumab, a recently approved humanized anti-CD20 monoclonal antibody (>150 000 patients treated), only one case of PML has been reported that is not attributable to prior treatment with another DMT, although PML occurrence in this patient might have been confounded by immunosenescence and low baseline lymphocyte counts.23 Several cases of PML have been reported following natalizumab treatment cessation, one also following fingolimod cessation, and subsequent initiation of another DMT, and thus are considered the so-called ‘carry-over’ cases, attributed to the prior treatment with natalizumab or fingolimod. As the latency between discontinuation of natalizumab and development or recognition of PML can vary, the risk of ‘carry-over’ PML, poses an additional challenge for clinicians with regards to MS pharmacovigilance.24 25 Carry-over PML also brings the risk of aggravating PML disease course by initiation of a subsequent DMT prior to PML detection, especially lymphocyte depleting treatments. This may have been the case with a lethal case of carry-over PML in a patient receiving alemtuzumab following natalizumab.26
Several factors are associated with an increased risk for PML during natalizumab treatment. First, while the risk for PML is low in patients who are seronegative for JCV, this risk increases significantly in anti-JCV antibody positive patients and is even higher in those with a high anti-JCV antibody index.27 Furthermore, the risk for PML during natalizumab treatment is increased in patients who were previously treated with older immunosuppressive drugs (azathioprine, mitoxantrone, cyclophosphamide), as well as patients with a natalizumab treatment duration of >18 months.27 It has been suggested that extending dosing intervals of natalizumab reduces the risk of PML, although this risk is still not negligible.28 29
Another strategy for PML risk assessment has been introduced for patients treated with dimethyl fumarate and comprises regular monitoring of absolute lymphocyte count in peripheral blood, as low lymphocyte counts appear to be associated with the development of PML in these patients.21 30 However, PML may also develop in patients treated with dimethyl fumarate without significant lymphopenia,31 and current recommendations are based on a very limited number of cases and controls. So far, no specific method for risk assessment for PML development has been determined with fingolimod treatment. Older age might be a risk factor independent of the underlying therapy that causes PML.20 32 33
MRI pharmacovigilance
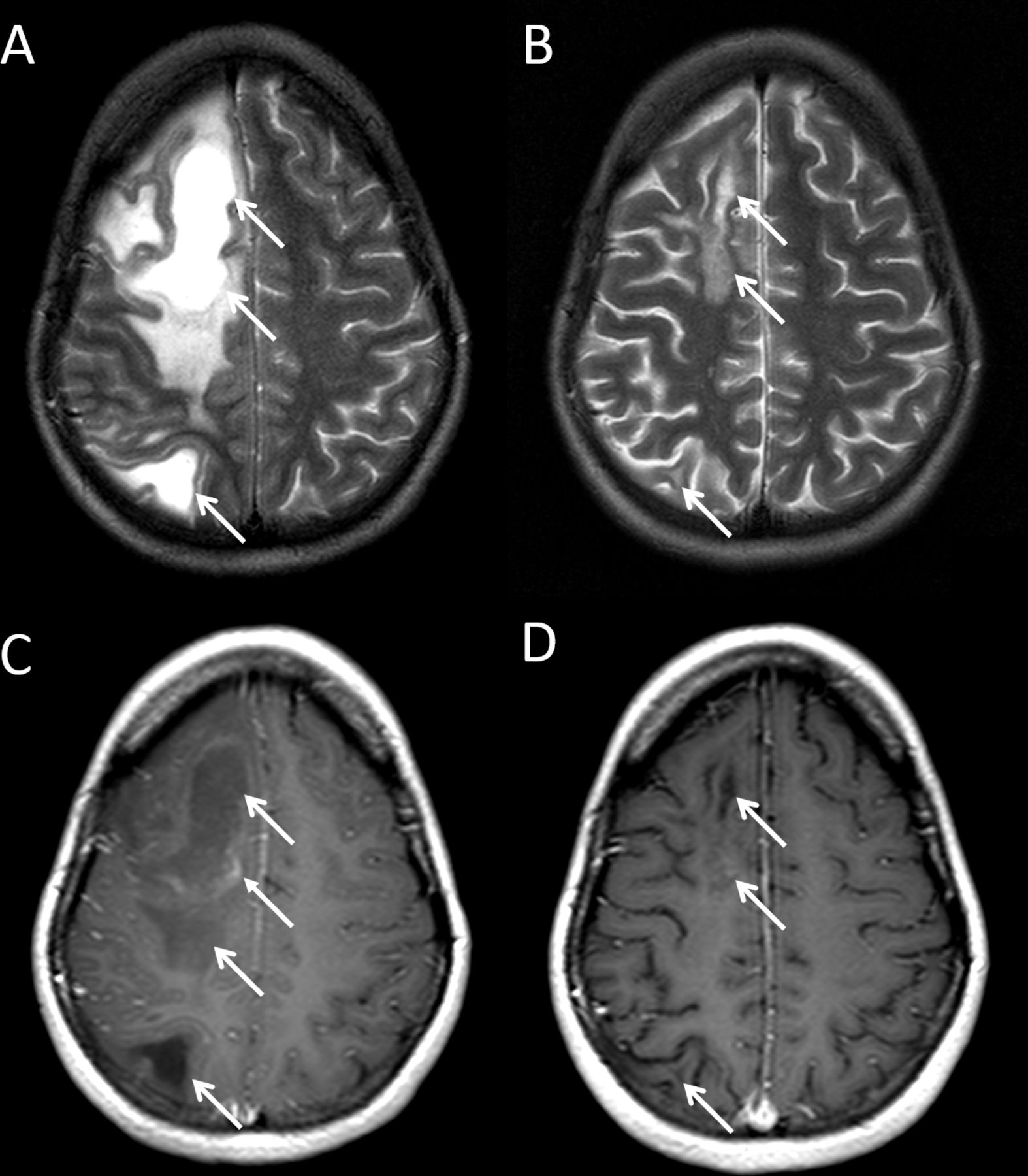
PML lesions typically present as T2 and fluid attenuation inversion recovery (FLAIR) hyperintense subcortical lesions with an isointense to hypointense signal on T1-weighted images (depending on disease stage and extent of demyelination) and are most frequently located in the frontal lobe followed by parietal and occipital lobe (figure 1, table 1).34 35 PML lesions frequently involve the cortical grey matter and may also be located infratentorial or in the deep grey matter.34 36 37 In addition, small punctate lesions with a perivascular distribution can be observed on T2/FLAIR sequences, which is regarded relatively specific for PML.36 38 Contrast enhancement is present in approximately one-third of the patients at PML diagnosis, generally with patchy enhancement in the border of the PML lesion, but small punctate enhancing lesions can also be observed.39 Diffusion weighted imaging (DWI) may reveal restricted diffusion associated with acute demyelination and thereby may assist in differentiating acute PML lesions from chronic or subacute MS lesion.40 GCN is characterised by progressive cerebellar atrophy on MRI either as a sole imaging finding, or concomitantly to classical PML lesions (figure 1, table 1).8 41

MRI of a patient with natalizumab-associated progressive multifocal leukoencephalopathy (PML) (A–D) and an MRI of a patient with signs of granule cell neuronopathy (GCN) concomitant to natalizumab-associated PML (E–H). Axial T2 (A), fluid attenuation inversion recovery (FLAIR) (B) and contrast enhanced T1 (C), and sagittal FLAIR images (D). Multifocal, confluent, T2 and FLAIR hyperintense lesions are visible in the frontal, parietal and temporal lobes, mostly located in the juxtacortical white matter extending in, and spreading through, the deep white matter. On T2, the lesions show a microcystic appearance. Parts of the lesions show a hypointense signal on T1. Axial FLAIR images prior to diagnosis (E, G) and at the time of PML with concomitant GCN diagnosis 3 months later (F, H). Note the appearance of cerebellar atrophy with bilateral dilated sulci on the follow-up images, with no infratentorial white matter PML lesions visible.
Basic MRI features of infectious and non-infectious adverse events during multiple sclerosis (MS) therapies
In patients at high risk for PML, expected efficacy and potential risks should be carefully weighed, also taking into account the expected efficacy and risk of an alternative treatment, and the risk of severe MS rebound following treatment cessation.42 For high-risk patients, enhanced pharmacovigilance is recommended including higher frequency (3–4 months) of MRI follow-up examinations.3 43 This recommendation is supported by the observational evidence that presymptomatic PML lesions could be detected in 78% of patients with natalizumab-associated PML during a period of approximately 5 months prior to symptom onset or formal diagnosis based on a positive MRI.44 Presymptomatic lesion detection leads to an improved survival and functional outcome,34 45 and frequent MRI surveillance leads to detection of significantly smaller PML lesion volumes and less disability at detection.43 Recent expert panel guidelines propose frequent MRI screening, every 3 to 4 months, using an abbreviated MRI protocol consisting of at least FLAIR, T2-weighted, and DWI sequences in patients at high risk for PML during natalizumab treatment, at the time of treatment cessation prior to introduction of a new DMT, and at least until 6 months after natalizumab discontinuation.3 46
This approach has been challenged,47 and indeed, asymptomatic PML lesion detection and differentiation from new MS lesions can be difficult, leading to a delay in diagnosis. Sensitivity and specificity of MRI for the diagnosis of asymptomatic natalizumab-associated PML on follow-up MRI of 91% and 100%, respectively, have been reported when using a standardised imaging protocol on the same MRI scanner and based on consensus reading by three neuroradiologists.37 When specifically testing the differentiation of asymptomatic PML from new MS lesions on MRI follow-up in a real-world natalizumab pharmacovigilance setting, a sensitivity of 74.2% and specificity of 84.7% with only a moderate inter-rater agreement was observed.48 This suggests the relevance of high neuroradiological expertise for the reading of surveillance MRIs, which should always be seen in the context of clinical and paraclinical information. The need for making an accurate differentiation between new MS lesions and asymptomatic PML lesions is further increased given the contradictory treatments. Incorrectly excluding PML will result in ongoing damage due to infection and, conversely, an erroneous suspicion of PML may lead to cessation of natalizumab and thus inadequate immunosuppression in a patient with MS disease activity.
In case of PML suspicion based on clinical symptoms and/or MRI results, the diagnosis of PML can be further established by demonstration of JCV DNA in CSF by PCR.49 However, JCV DNA can be undetectable in both asymptomatic as well as symptomatic patients, hampering a diagnosis of PML.25 50 51 Indeed, patients with smaller PML lesion volumes more frequently have a negative PCR,52 indicating that CSF in patients suspected for PML should be tested in reference laboratories with a very low limit of detection (around 10 cp/mL CSF). Furthermore, additional tests such as the assessment for the intrathecally produced anti-JCV antibody fraction or the lesion evolution on MRI may support the diagnosis in some cases.44 53–55
Herpesviruses
Herpes simplex virus (HSV) is an ubiquitous virus of the herpesvirus family. There are two subtypes, HSV-1 and HSV-2. HSV-1 is a common and highly contagious virus and the WHO has recently estimated that 67% of the human population under the age of 50 years is carrier of HSV-1 with the virus remaining latent in neural ganglia.56 HSV-2 is less frequent, but still a highly prevalent and almost exclusively sexually transmitted virus with the virus remaining latent in the sacral ganglia. Although rare, with an estimated incidence of 1 in 250 000 to 500 000 per year,57 herpes simplex encephalitis (HSE), predominantly caused by reactivation of the HSV-1 virus, is the most common cause for sporadic encephalitis that can occur in both immunocompetent and immunocompromised individuals. HSE carries a considerable morbidity and mortality. HSV PCR in CSF is used to confirm the diagnosis. Varicella zoster virus (VZV) also belongs to the family of herpesviruses, and has been reported to cause CNS infections, such as VZV encephalitis. Prompt initiation of antiviral treatment is essential.58
Herpesviruses in MS therapies
In 2013, Fine et al reported 20 cases of CNS herpesvirus infections in patients treated with natalizumab based on postmarketing reports received by the US Food and Drug Administration (FDA).59 Of these patients, 11 had HSE, 8 patients had meningitis (6 HSV and 2 VZV), 1 had meningoradiculitis (VZV), and 1 meningomyelitis (VZV). In other reports, VZV myelitis, meningovasculitis and retinitis associated with CNS vasculitis have been described in patients treated with natalizumab.60–62 Although it is difficult to assess the risk for HSV-related CNS disease, the authors found that the number of patients with HSE appears to be over-represented in patients treated with natalizumab when comparing to the background incidence. In addition, fingolimod treatment increases the risk for VZV infections, mostly herpes zoster but at least four cases of VZV encephalitis have been described.63–66 Therefore, vaccination is recommended for patients without varicella immunity before starting fingolimod.67 Fingolimod also appears to be associated with an increased risk for HSV infections with two cases of HSE reported.66 68 Recently, one case of HSE has been reported in a case treated with dimethyl fumarate with a marked decline in blood lymphocytes prior to HSE development.69 Finally, cladribine, ocrelizumab and alemtuzumab all increase the risk for mucocutaneous herpes infections (both HSV and VZV),70 71 but so far only two patients with MS who developed herpes infection of the CNS were reported in association with these drugs (herpes meningitis in a patient treated with alemtuzumab and HSE in a patient treated with ocrelizumab).72 73 Prophylactic acyclovir treatment is recommended for 1 month following initiation of each course of alemtuzumab (alemtuzumab Summary of Product Characteristics (SPC)).
MRI pharmacovigilance
Patients with HSE usually present with acute change in mentation or focal neurological deficits, sometimes in combination with fever and seizures. MRI typically shows lesions in the temporal lobe, although extratemporal abnormalities occur and can even be the only visible abnormality (55% and 15%, respectively, in one study; figure 2, table 1).74 Another study showed that in immunocompromised patients HSE can have a more atypical manifestation, showing more extensive brain involvement including atypical regions and excluding the temporal lobe on MRI, regularly with normal cell counts in the CSF, and a substantial increase of morbidity and mortality.75 With VZV infection of the CNS, MRI may show no abnormalities, vascular lesions (both haemorrhagic and ischaemic), vasculitis, meningitis, myelitis, non-specific abnormalities, or a combination of these (figure 2, table 1).62 76 As development and progression of CNS infection are probably always very rapid, regular MRI screening is not an option. Therefore, clinical vigilance and awareness of the risk of herpesvirus infections in patients treated with natalizumab, fingolimod, alemtuzumab and ocrelizumab, and with MRI as part of the diagnostic workup, may be warranted.

MRI of a patient with herpes simplex virus encephalitis during treatment with natalizumab (A–C) and a MRI of a patient with varicella zoster meningovasculitis during treatment with natalizumab (D–F). Axial fluid attenuation inversion recovery (FLAIR) (A), diffusion weighted imaging (DWI) (B), and contrast enhanced T1 (C). A lesion in the right parietal lobe is visible, showing a high signal intensity of both cortical grey matter and juxtacortical white matter on FLAIR images. The cortical part of the lesion shows a high signal intensity on DWI. On T1, the juxtacortical part of the lesion shows a low signal intensity and meningeal enhancement. Also note the swelling in and around the lesion. Axial FLAIR image 3 months prior to diagnosis (D), contrast-enhanced axial FLAIR at diagnosis (E), and contrast enhanced axial FLAIR 3 months following diagnosis and treatment with acyclovir (F). Several small nodular leptomeningeal lesions are visible in both frontal lobes. Similar lesions were visible infratentorial and on the spinal cord, and MR angiography showed signs of vasculitis.
Cryptococcus
Cryptococcus is an encapsulated yeast often found in bird excrements which may enter the human body via inhalation of spores, potentially causing serious pulmonary infections and/or meningoencephalitis. Cryptococcus neoformans is the type most commonly infecting humans, and is mostly observed in immunocompromised patients.77 It is believed that C. neoformans causes an asymptomatic focal pneumonitis following inhalation resulting in a latent infection, with a risk for reactivation on immunosuppression.78 In HIV-infected patients, cryptococcal meningitis predominantly affects patients with CD4 counts <100 cells/µL.79 Diagnosis is mostly based on a rapid cryptococcal antigen test in CSF.
Cryptococcus in MS therapies
In 2015, a case of cryptococcal meningoencephalitis was reported in a patient with MS treated with fingolimod,80 and until now 10 cases have been published.81 82 In addition, cases with disseminated cryptococcal infection with both a CNS and dermal and/or pulmonary involvement were reported.81 Immunosenescence appears to play an important role in the development of cryptococcal meningoencephalitis in fingolimod treated patients, with an increased risk for patients that are older, have a longer treatment duration (which induces immunosenescence-like changes), and have low CD4 counts.83 In natalizumab-treated patients, two cases of cryptococcal meningitis have been reported, one of whom died from immune reconstitution inflammatory syndrome within a week after initiation of antifungal therapy.84 85 Recently, a first case of cryptococcal meningitis has been described in a patient treated with dimethyl fumarate, despite normal absolute lymphocyte counts and absence of other risk factors.86
Several cases of cryptococcal meningitis have been reported in patients treated with rituximab, alemtuzumab and cladribine for other indications, such as leukaemia, rheumatoid arthritis, and organ transplantations, but so far not for MS.87–89 In these patients, a potential link with the drug is obscured by their comorbidities and additional treatments with other chemotherapies or immunosuppressive drugs, which contributed to the impaired immune status.
MRI pharmacovigilance
Patients with cryptococcal meningoencephalitis typically present with headache, fever and malaise. A recent study investigated imaging findings of cryptococcal meningitis in 114 HIV-negative patients and found 69% of patients showing characteristic lesions of cryptococcal meningitis on brain MRI.90 The most common findings were general signs of meningitis (either pachymenineal or leptomenineal enhancement), followed by dilated perivascular spaces, hydrocephalus, intracerebral nodules, and pseudocysts (figure 3, table 1).90 As cryptococcal meningoencephalitis tends to develop swiftly, it is unlikely that frequent MRI scanning would detect the disease in a presymptomatic stage. Therefore, awareness and clinical vigilance with respect to the occurrence of cryptococcal infections particularly in patients treated with fingolimod, natalizumab or dimethyl fumarate remains crucial, especially in older patients and those with a longer fingolimod treatment duration.

MRI of a patient with cryptococcal meningoencephalitis during treatment with fingolimod (A–D) and an MRI of a patient with central nervous system nocardiosis following treatment with alemtuzumab (E–H). Axial T2 (A, B) and contrast enhanced T1 (C), and coronal fluid attenuation inversion recovery (FLAIR) images (D). Non-enhancing T2 and FLAIR hyperintense lesions in the basal ganglia (cryptococcomas). Panel D shows spread of cryptococcomas through the mesencephalon into the pons. Axial FLAIR (E), diffusion weighted imaging (F) and contrast enhanced T1 (G), and coronal contrast enhanced T1 images (H). Multiple small brain abscesses with ring enhancement are visible in the supratentorial brain parenchyma, with surrounding oedema and some showing subtle diffusion restriction. Also note the spread of the abscesses infratentorial and in the spinal cord.
Listeria
Listeriosis is caused by the gram-positive anaerobic bacterium Listeria monocytogenes. The main route for infection is through contaminated food such as raw meat and fish, shellfish, uncooked vegetables, unpasteurized dairy products, and soft cheeses. Listeriosis is mostly reported with one of the three following presentations: bacteraemia, meningoencephalitis and maternofetal or neonatal listeriosis, and has a fatality rate of 20%–30%.91 Depending on the country, the incidence of listeriosis varies between 0.1 and 11.3/1 000 000, predominantly affecting immunocompromised patients, elderly, pregnant women and their fetuses, and neonates.91 In addition, listeriosis may present as self-limiting gastroenteritis in immunocompetent individuals, which likely is hugely underdiagnosed due to the non-specific symptoms.91
Listeriosis in MS therapies
Since 2008, several cases of listeria meningitis in patients with MS treated with alemtuzumab have been reported. A comprehensive series of 22 cases of listeriosis associated with alemtuzumab published in the literature and/or reported to VigiBase (an international database of suspected adverse drug reactions from the WHO) was reported by Holmøy et al in 2017.92 Although some cases lacked information on the indication for treatment, and on the clinical presentation and/or clinical outcome, at least 16 of the 22 patients were treated for MS (first or second cycle), 9 of whom presented with meningitis/meningoencephalitis, 2 with sepsis, and 5 with an unknown presentation, and at least 3 patients died.92 At the time of publication, approximately 11 500 patients with MS had been treated with alemtuzumab and thus, the authors calculated, the incidence of listeriosis appears to be around 0.1% (16/11 500).92 Following alemtuzumab treatment, CD4(+) and CD8(+) T cells and dendritic cells, crucial in controlling the infection, are rapidly depleted from circulation and cytokine release is impaired.93 94 Interestingly, in several of the reported cases, symptoms of listeriosis developed within days after or even during the alemtuzumab treatment cycle.92 Recently, two cases of listeria induced rhombencephalitis have been reported, one with dimethyl fumarate treatment and one with fingolimod treatment.95 96 Although, no cases of listeria meningitis have been reported in patients treated for MS with B-cell or lymphocyte depleting therapies such as rituximab, ocrelizumab and cladribine; five have been reported with rituximab for other indications.97
MRI pharmacovigilance
Brain MRI can reveal signs of leptomeningitis, lesions suggestive of encephalitis and abscess formation. Specifically, listeria can cause rhombencephalitis, affecting primarily the brainstem and cerebellum (table 1).98 Listeriosis develops rapidly, and as specific risk factors in alemtuzumab treated patients have not yet been identified and the incidence is low, MRI screening for CNS listeria infection is not justified. Prevention of listeriosis by adhering to a listeria-free diet starting 2 weeks prior to treatment, during treatment, and at least 1 month following an alemtuzumab treatment cycle, as recommended in the SPC, may prevent infection. In addition, cotrimoxazole is often prescribed as listeria prophylaxis for 1 month following initiation of each alemtuzumab cycle.99
Nocardia
Nocardiosis is caused by the gram-positive aerobic bacteria Nocardia, containing a total of 85 subspecies of which some are pathogenic. Most infections are acquired through inhalation or via traumatic skin lesions and generally occur as an opportunistic infection in immunocompromised patients, especially those with an impaired cell-mediated immune response.100 The most frequent clinical presentation is pulmonary nocardiosis; however, the disease can disseminate through haematological spreading and affects the CNS in up to 44% of patients.101
Nocardiosis in MS therapies
Until now, only two cases of nocardiosis during treatment of MS, both treated with alemtuzumab, have been reported, one with CNS nocardiosis and one with pulmonary nocardiosis.102 103 The patient with CNS nocardiosis presented with a tetraspastic syndrome 4 months after the first cycle of alemtuzumab and diagnosis was finally made through culture of intracranial abscess material acquired via biopsy, as broad screening of both blood and CSF returned negative.102 Patients treated with rituximab for other indications have also developed nocardiosis104; however, comorbidities and concomitant therapies may have contributed to the development of nocardiosis in these patients.
MRI pharmacovigilance
Most patients with CNS nocardiosis present with confusion, followed (in order of frequency) by weakness, speech impairment and headache and only rarely with meningism.101 The vast majority of patients with CNS nocardiosis show formation of a parenchymal abscess, evidenced by a ring-enhancing lesion on MRI (figure 3, table 1).101 However, space-occupying lesions can be invisible. In a minority of patients, the disease manifests as meningitis, with or without associated brain abscess.105 Due to the low incidence, MRI screening for CNS nocardiosis is not useful.
Non-infectious adverse events
Reversible cerebral vasoconstriction syndrome and posterior reversible encephalopathy syndrome
Reversible cerebral vasoconstriction syndrome (RCVS) is believed to be caused by segmental constriction of cerebral arteries which often is spontaneously reversible within 3 months after onset, and generally presents with thunderclap headache and, less frequently, with focal neurological deficits or seizures.106 RCVS is associated with the posterior reversible encephalopathy syndrome (PRES), which is characterised by headache, confusion, visual symptoms and seizures and is clearly associated with hypertension.107 Indeed, RCVS and PRES share overlapping pathophysiology.108 RCVS and PRES are both associated with autoimmune diseases, but also with immunosuppressive drugs. Almost half of patients with PRES have a history of autoimmune disease, and in at least half of patients with RCVS the disease was preceded by treatment with vasoactive drugs or childbirth.106 107
RCVS and PRES in MS therapies
The link between MS therapies and RCVS and PRES is anecdotal and includes several case reports. RCVS has been reported in two patients treated with fingolimod109 110 and one patient treated with interferon beta 1-a.111 Furthermore, PRES has been reported in patients treated with fingolimod,112 natalizumab113 and high-dose corticosteroids.114 However, VigiBase reports a total of 34 and 7 cases of PRES and RCVS, respectively, in patients treated with fingolimod and 9 cases of PRES in natalizumab treated patients.115 Although these numbers should be interpreted with caution and should not be used to calculate incidences in relation to DMTs, as no causal relation is proven and comorbidities may play a role, they do suggest that PRES and RCVS may complicate MS therapies more frequently than previously assumed.
MRI pharmacovigilance
RCVS can be complicated by stroke, subarachnoidal haemorrhage, or intracerebral haemorrhage which are reported in 39%, 34% and 20% of cases, respectively.116 In PRES, brain MRI may show vasogenic oedema in the parieto-occipital region (70%), often with a symmetrical bihemispheric distribution which is contrasting with PML (figure 4, table 1).117 RCVS and PRES show very similar findings on cerebral angiography: segmental narrowing and dilatation, often bilateral, resembling a string of beads. As RCVS and PRES follow a very rapid course, screening via MRI is not an option. However, clinical awareness and early detection and recognition of these conditions by MRI is important as eliminating the triggering factor (DMT for MS in this case) might improve the outcome.

MRI of a patient with posterior reversible encephalopathy syndrome as a consequence of glomerulonephritis secondary to treatment with alemtuzumab (A–D) and an MRI of a patient with primary central nervous system lymphoma during treatment with fingolimod (E–H). Axial fluid attenuation inversion recovery (FLAIR) (A, B) and T2 (C), and sagittal T2 images (D). The image shows bilateral, subcortical and more or less symmetrical, FLAIR and T2 hyperintense lesions characteristic of vasogenic oedema in the occipital, parietal and frontal lobes. Axial T2 (E, G) and contrast enhanced T1 images (F, H). Multifocal and bilateral T2 hyperintense lesions in the cerebellum, thalamus and nucleus caudatus, showing homogeneous contrast enhancement. The left cerebellar lesion shows significant mass effect.
Primary central nervous system lymphoma
Primary central nervous system lymphoma (PCNSL) is a very rare non-Hodgkin’s lymphoma, with an estimated incidence of 1.6 per 1 000 000 per year.118 Although the initial response to chemotherapy and radiation therapy is generally good, long-term prognosis is relatively poor. PCNSL has been reported with a higher incidence in immunocompromised patients, such as HIV/AIDS and immunosuppressive treatments, and in senescence.
PCNSL in MS therapies
Since the first report by Schweikert et al in 2009, accumulating case reports and case series suggest that PCNSL is a rare complication of natalizumab treatment.119 120 Remarkably, PCNSL has been reported in EBV positive and negative natalizumab-treated patients (at least three out of eight in the current case series were EBV negative), and following a relatively short treatment duration (<7 doses in all but one case).119 The mechanism by which immunosuppression may induce PCNSL in EBV negative patients remains to be elucidated. Diminished immunological surveillance by T-lymphocytes induced by natalizumab treatment may be involved. More recently, a case of T-cell PCNSL has also been described during treatment with fingolimod.121
MRI pharmacovigilance
In general, PCNSL is characterised by single lesions (63% of cases), predominantly located in the periventricular areas or deep grey matter, with homogenous contrast enhancement and mild oedema (figure 4, table 1).122 In immunocompromised patients, however, PCNSL more often presents with a multifocal pattern with central necrosis and ring enhancement.123 Screening for PCNSL by frequent MRI studies will not be effective given the low incidence and rapid evolution of PCNSL. Recognition of PCNSL on MRI, and discriminating PCNSL from tumefactive demyelinating lesions (TDL), is essential in view of the conflicting treatment options.
Neuroinflammation
(Re)activation of neuroinflammation in MS therapies
Following both the initiation and cessation of fingolimod, severe clinical deterioration accompanied by TDL has been reported.124–129 In addition, natalizumab treatment has been associated with TDL.130–133 Induced lymphocyte subset shift or rapid lymphocyte influx into the CNS and natalizumab neutralising antibodies have been suggested to play a role in TDL development with fingolimod and natalizumab, respectively.132 134 Furthermore, over a dozen cases have been reported showing a severe clinical and radiological MS disease activity 6 months following a first alemtuzumab cycle,135 136 which is likely preceded by an abnormal B-cell reconstitution and responds strongly to B-cell/humoral focused therapy (eg, plasmapheresis and rituximab).136 Interestingly, a case of autoimmune encephalitis 8 months following a second alemtuzumab cycle was reported more recently, again responding well to B-cell depleting therapy.137 138
MRI pharmacovigilance
TDL presents as a large, tumor-like, demyelinating brain lesion showing open-ring enhancement, in contrast to most malignant tumours and abscesses which often show closed-ring enhancement (figure 5, table 1). In addition, TDL often shows oedema and mass effect, which contrasts with PML.134 Given the rapid lesion evolution leading to symptoms, MRI screening specifically for TDL will not be useful. Early recognition of the typical MRI characteristics of TDL during DMT is essential, as cessation of therapy may be the best option.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI of a patient with tumefactive demyelinating lesions during treatment with fingolimod. Axial T2 (A, B) and contrast enhanced T1 images (C, D). A large demyelinating T2 hyperintense lesion in the right frontal, parietal and occipital lobes with significant mass effect and surrounding oedema is visible. The lesion shows a hypointense signal on T1 with contrast enhancement in the border of the lesion (A, C). Two months later the lesion has significantly deceased and no longer shows mass effect or contrast enhancement (B, D).
Drug reaction with eosinophilia and systemic symptoms
Drug reaction with eosinophilia and systemic symptoms (DRESS) is a severe drug-induced reaction, manifesting with eosinophilia, fever, lymphadenopathy and multiorgan involvement, sometimes including CNS vasculitis, encephalitis and intracranial haemorrhage, usually after 2–12 weeks of drug exposure.139 140 In March 2018, the Pharmacovigilance Risk Assessment Committee of the EMA noted that at least 12 patients experienced autoimmune encephalitis (later attributed to DRESS) during treatment with daclizumab, a humanised monoclonal antibody binding to CD25, which led to the withdrawal of daclizumab from the market by its manufacturer.141 MRI in these patients generally showed contrast enhancing lesions with a remarkable amount of vasogenic oedema.142 143 So far, no cases of DRESS syndrome have been reported in patients treated with other DMTs.
Cerebrovascular events with alemtuzumab treatment
Recently, the FDA released a safety communication on the occurrence of ischaemic or haemorrhagic stroke and cervical artery dissection in 13 patients treated with alemtuzumab.144 A recent study presented five of these cases, all showing intracranial haemorrhage on imaging very similar to haemorrhages with a hypertensive aetiology.145 The authors point out that alterations in hemodynamics are likely related in these patients as they are frequently observed during alemtuzumab treatment. The use of alemtuzumab has been restricted by the EMA pending a review of the drug.
Discussion
With the introduction of effective immunosuppressive treatment options for MS, serious side effects of DMTs affecting the CNS have emerged. These include reactivation of primary infection with common pathogens such as JCV, HSV, VZV and Cryptococcus; de novo infections with VZV, Listeria and Nocardia, and non-infectious complications including PRES, RCVS, PCNSL, neuroinflammation, cerebrovascular events and DRESS (table 2). Although the potential benefits of DMTs are generally considered to outweigh the risks for these adverse events on a population level, these complications can be severely debilitating and life threatening for the individual. Early detection and diagnosis are essential, as this allows for timely therapeutic interventions, which almost always will include cessation of the DMT. In addition, specific and early initiation of antibiotics, antiviral medication, antifungal treatment, immune suppression or antitumor treatment regimens may improve the outcome, thereby diminishing the risk of irreversible neurological sequelae and death.
Estimated risk of different disease-modifying treatments (DMTs) for infectious and non-infectious central nervous system adverse events in patients with multiple sclerosis
In addition to a detailed patient history and physical examination, suspicion of a CNS complication warrants brain MRI. Recognition of the specific MRI patterns of CNS complications is essential for a timely diagnosis and commencement of proper treatment. Moreover, different adverse events sometimes warrant contrasting therapeutic interventions which may even be detrimental when applied for a misdiagnosis (eg, corticosteroids in a patient with CNS infection when TDL is wrongfully suspected).
Regular brain MRIs as part of pharmacovigilance have been introduced for the follow-up of natalizumab-treated patients at high risk for developing PML, although the cost–benefit ratio is still a matter of debate.3 43 44 46 47 For example, the most recent risk stratification estimates that for patients who are anti-JCV antibody positive with an antibody index level of >1.5 and without prior immunosuppressive treatment, 2.6 and 10 per 1000 patients will develop PML in the third and sixth year of treatment, respectively.27 In other words, 385 or 100 patients need to be monitored before one case of PML develops in the third or sixth year of treatment. When performing a pharmacovigilance MRI four times a year, this would result in 1540 or 400 MRIs, respectively, and, in the Netherlands, €408 100, or €106 000, per patient with new natalizumab-associated PML (average cost of a brain MRI: €265). On the other hand, a recent study quantified the positive impact on clinical outcome of frequent MRI screening.43 The authors showed that MRI surveillance every 3 to 4 months led to a significantly lower increase in disability due to PML than those with MRI assessment every 6–12 months (median expanded disability status scale increase of 0.5 vs 2.25). Further studies into the cost effectiveness of MRI screening should further include prizing of reduction of disability and mortality as well as costs of medication. Regular brain MRI for pharmacovigilance of all other DMT related, non-JCV associated, adverse events affecting the CNS does not seem to be justifiable as these are rare and carry a low cost–benefit ratio. Clinical vigilance therefore remains paramount.
Acknowledgments
The authors wish to thank Luca Prosperini, Patricia Mulero, Alex Rovira, Lutz Achtnichts, Krassen Nedeltchev, Horst Penkert, Thomas Korn, and their patients for the imaging data of cases presented in this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it appeared Online First. Figure 4 has been corrected.
Contributors MTW and MPW provided the initial idea and outline of content for the manuscript. All authors contributed content and critically reviewed and edited the manuscript. MTW submitted the study and is responsible for the overall content as guarantor.
Funding The MS Centre Amsterdam is funded by a programme grant (14-358e) from the Stichting voor MS Research (Voorschoten, The Netherlands). CW received support from the Hertie foundation (P1150063). This work was supported in part by NIH grants R01 NS 047029 and NS 074995 to IJK.
Competing interests CW has received institutional fees for consultancy, speaking, or research from Novartis, Biogen, Sanofi-Genzyme and Roche; no personal fees within the last three years. CM has received consultancy or speaking fees from Actelion, Biogen, Merck, Novartis, Roche, Sandoz, Sanofi-Genzyme, Teva. IJK has received consultancy fees from Biogen, Regeneron and Agios Pharmaceuticals. JK has received consultancy fees from Merck-Serono, Teva, Biogen, Genzyme and Novartis. MPW has received consultancy fees from Biogen and Roche.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.