Article Text

Abstract
Cerebral microbleeds (CMBs) are defined as hypointense foci visible on T2*-weighted and susceptible-weighted MRI sequences. CMBs are increasingly recognised with the widespread use of MRI in healthy individuals as well as in the context of cerebrovascular disease or dementia. They can also be encountered in major critical medical conditions such as in patients requiring extracorporeal mechanical oxygenation. The advent of MRI-guided postmortem neuropathological examinations confirmed that, in the context of cerebrovascular disease, the vast majority of CMBs correspond to recent or old microhaemorrhages. Detection of CMBs is highly influenced by MRI parameters, in particular field strength, postprocessing methods used to enhance T2* contrast and three dimensional sequences. Despite recent progress, harmonising imaging parameters across research studies remains necessary to improve cross-study comparisons. CMBs are helpful markers to identify the nature and the severity of the underlying chronic small vessel disease. In daily clinical practice, presence and numbers of CMBs often trigger uncertainty for clinicians especially when antithrombotic treatments and acute reperfusion therapies are discussed. In the present review, we discuss those clinical dilemmas and address the value of CMBs as diagnostic and prognostic markers for future vascular events.
- cerebrovascular disease
- stroke
- cognition
- MRI
Statistics from Altmetric.com
Introduction
Cerebral microbleeds (CMBs) are a radiological construct and appear as hypointense foci visible only on MRI.1 CMBs have received increasing interest over the past two decades. They can be observed in individuals with stroke and cognitive complaints and in healthy individuals. In daily clinical practice, the presence and numbers of CMBs often trigger uncertainty for clinicians especially when antithrombotic treatments are considered.
In this review, we will critically analyse the knowledge accumulated and advances about CMBs and will focus our discussion on the nature of these MRI-defined lesions, their potential role as diagnostic and prognostic markers, and when and how CMBs should influence our management.
CMBs are radiological constructs, but what is their histopathological nature?
Cerebral MRI: from image acquisition to image analysis
CMBs are small (2–10 mm diameter) round or ovoid hypointense foci with associated blooming with enhanced visibility on MRI sequences sensitive to susceptibility effects.2 3
Image acquisition parameters
Local magnetic field inhomogeneities caused by paramagnetic iron in CMBs result in signal loss on some MRI sequences. T2*-weighted gradient echo, usually acquired as two-dimensional axial images with 3–5 mm slice thickness at 1.5 T, is the traditional sequence used to detect CMBs but several parameters can influence their depiction (figure 1).2 3 A low flip angle, long echo time and long repetition time increase the sensitivity to susceptibility effects.2 The susceptibility effect and signal-to-noise ratio increase with higher magnetic field strength (eg, 3 T or 7 T compared with 1.5 T).4–8 Increasing the spatial resolution by acquiring three dimensional sequences improves CMB detection.5 Susceptibility-weighted imaging (SWI) is derived from gradient echo pulse sequences with additional postprocessing steps to improve contrast resolution. It is usually acquired in three dimensions to increase spatial resolution and has flow compensation in all three planes to reduce artefacts. SWI has increased sensitivity and reliability for CMBs compared with T2*-weighted gradient echo but requires longer acquisition time.9 Fast acquisition of SWI using a parallel imaging technique results may improve detection.10
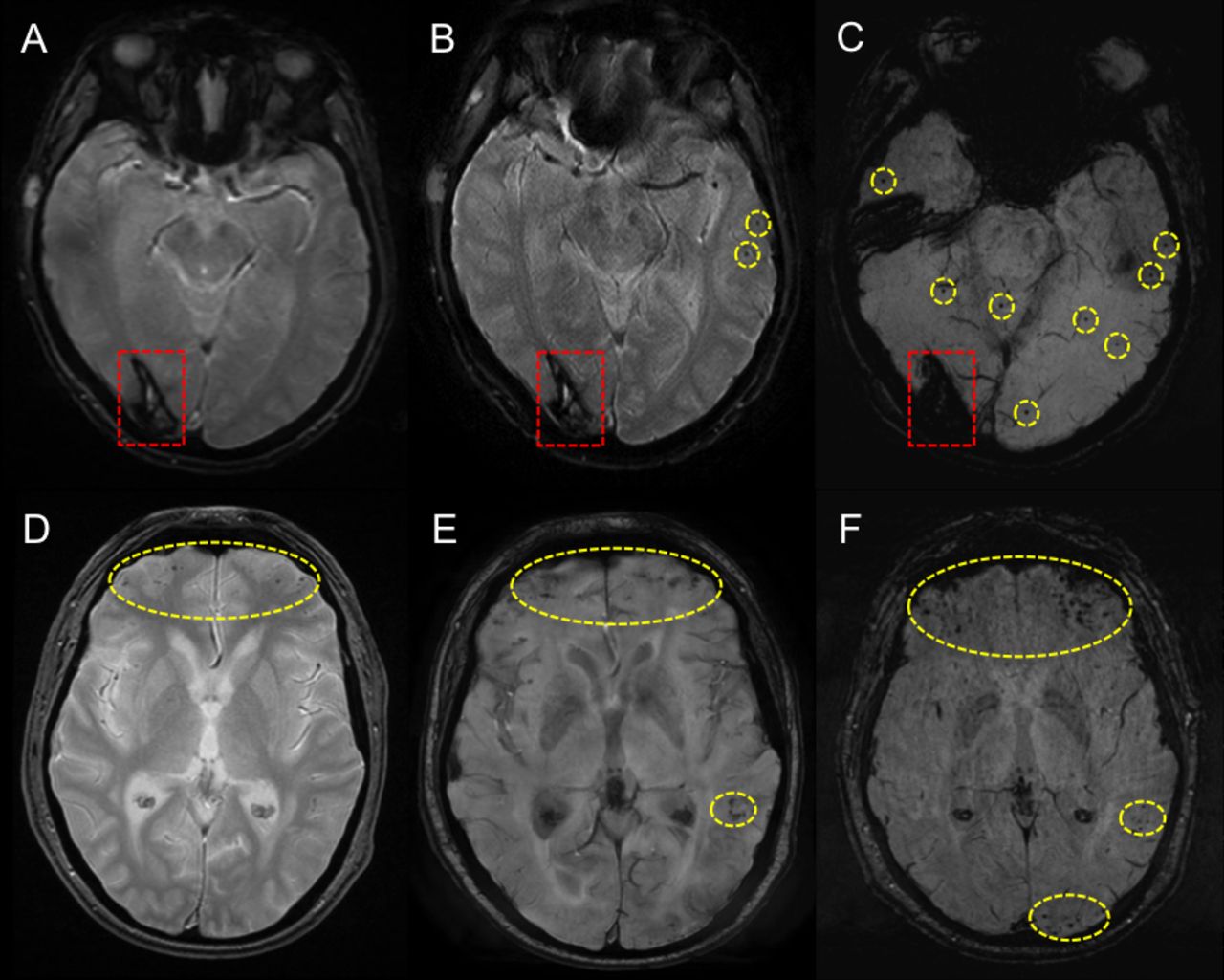
Influence of sequence and magnetic field strength on CMB detection. Effects of sequence and magnetic field strength on CMB detection in two patients with spontaneous intracerebral haemorrhage (A–C and D–F). (A) Axial T2*-gradient echo at 1.5 T shows a right occipital intracerebral haemorrhage (red rectangle) but no CMBs, (B) axial SWI at 1.5 T shows two left temporal CMBs (yellow rings) and (C) axial minimum intensity projection SWI at 3 T shows multiple CMBs in the temporal and occipital lobes and cerebellar vermis (yellow rings). (D) Axial T2*-gradient echo at 1.5 T shows a few CMBs in both frontal lobes and the left temporal lobe (yellow rings), (E) axial SWI at 1.5 T shows more CMBs in the frontal and left temporal lobes plus left occipital lobe CMBs (yellow rings) and (F) axial SWI at 3 T shows more CMBs with increased conspicuity in the frontal and left occipital lobes (yellow rings). CMB, cerebral microbleed; SWI, susceptibility-weighted imaging.
Image analysis
Some structures or lesions exhibit susceptibility effects that can mimic CMBs (eg, curvilinear small cortical vessels, iron deposits in the basal ganglia, diamagnetic calcifications and artefact from bone-air interfaces in the temporal and inferior frontal lobes) and must be excluded first. CMBs are most frequently identified and quantified using visual assessment. The Microbleed Anatomical Rating Scale and Brain Observer MicroBleed Scale provide structured approaches for assessing CMBs.11 12 These scales have been developed using T2*-weighted GRE at 1.5 T but less is known about inter-rater agreement using SWI and at higher field strengths. Semiautomated and fully automated approaches are potentially useful for quantifying CMBs given the time required and inter-rater variability of visual rating. Several methods have been described using lesion intensity and/or geometry to detect CMBs, resulting in sensitivities for CMBs ranging from 50% to 89%.13–15 However, the small size of CMBs, their potential mimics and anatomical distortions due to background brain lesions (such as macrohaemorrhages or tumours) limit specificity, resulting in many false positives that need to be removed by visual inspection. Machine-learning methods may minimise the number of false positives using high-level features.16 However, such methods are challenging since they need large precisely labelled data sets for training and a large number of participants with varying underlying pathologies imaged on different MRI systems.
Recent advances and novel approaches
Ultra-high field 7 T MRI is a promising technique for studying CMBs. 7 T MRI detects more CMBs than 3 T or 1.5 T, particularly smaller CMBs.6 The high spatial resolution of 7 T MRI allows detailed assessment of CMBs as well as microvessels structure and function, which may help establish a pathophysiological link between CMBs and small vessel diseases (SVDs). However, the increased artefacts at 7 T MRI, especially near the skull base, may hinder its use. Quantitative susceptibility mapping (QSM) permits quantitative measures of tissue susceptibility, such as iron and calcium, using GRE phase data.17 The total magnetic susceptibility of a CMB is relatively consistent across imaging parameters18 and independent of field strength.Therefore, QSM may provide a more consistent method for quantifying CMB burden within and across studies, and detecting longitudinal change than assessing their number on T2*-weighted GRE or SWI.4
Histopathological correlates and mechanisms of brain injury
Understanding of the histopathological correlates of CMBs was initially lacking. The advent of MRI-guided neuropathological examinations, in the context of cerebrovascular diseases, helped bridge this gap, confirming that the majority of CMBs correspond to recent or old microhaemorrhages.19 20 Recent microhaemorrhages can be identified by intact or lysed extravasated red blood cells on standard H&E-stained sections. In the subacute phase (>24 hours after extravasation) red blood cells lyse and are transformed into blood-breakdown products in the form of haematoidin or haemosiderin and are taken up by macrophages (figure 2). Chronic microhaemorrhages can be identified by focal clusters of haemosiderin-laden macrophages on H&E that stain positive for iron. The presence of iron in old microhaemorrhages contributes to enhanced visibility on MRI.20–22 A combined in vivo MRI-ex vivo MRI-histopathology study in cases with cerebral amyloid angiopathy (CAA) revealed that due to this ‘blooming effect’ lesions that measured only a few hundred μm on H&E were still detectable on T2*-weighted clinical in vivo MRI.21 That said, conventional MRI routinely used in clinical practice likely underestimates total CMB burden.21 23 24 Other lesions, such as microaneurysms, fibrinoid necrosis and haemorrhagic microinfarcts are thought to account for a small subset of MRI-detected CMBs20 21 (figure 2).

Histopathological examples of cerebral microbleeds (CMBs), mimics and associated vessel abnormalities. Examples of acute (A), subacute (B), and an iron-positive old microbleed (C) on H&E-stained sections in cases with cerebral amyloid angiopathy (CAA). Examples of fibrinoid necrosis (D), vessel calcifications (E), and an iron-positive haemorrhagic microinfarct (F) that can appear as microbleeds on T2*-weighted MRI. Examples of vessel abnormalities that have been associated with microbleed formation include fragmentation of the wall including loss of amyloid β (Aβ) in a case with CAA (G), loss of smooth muscle cells (SMCs) in a case with hypertensive arteriopathy (H), and fibrin extravasation into the wall and surrounding parenchyma (I). All scale bars indicate 250 µm.
Besides an increased understanding of the histopathological correlates of MRI-observed CMBs, ex vivo MRI-guided histopathological evaluation of CMBs has provided clues for their potential pathophysiological mechanisms. In patients with sporadic CAA, CMBs are almost exclusively found in the cortical grey matter, predominantly in posterior brain regions where CAA is often more severe.25 Serial sectioning of individual CMBs revealed that the majority originate from penetrating cortical arterioles and are the result of advanced CAA. Interestingly, vessels involved in microbleeding had an abnormal appearance, including dilation and fragmentation of the wall, loss of both smooth muscle cells and amyloid β (Aβ), and fibrin extravasation.25 26 Collectively, these histopathological findings suggest that CAA-affected blood vessels may undergo extensive remodelling prior to bleeding. Whether this process is in part immune-mediated is currently under investigation and has implications for the interpretation of haemorrhagic amyloid-related imaging abnormalities in the context of anti-Aβ immunotherapy.27 Whether similar pathophysiological mechanisms play a role in the formation of CMBs in deeper areas of the brain in cases with hypertensive arteriopathy is currently incompletely understood and awaits further (preferably MRI-guided) histopathological investigations.28 29
Experimental animal models of CMBs provide further information on their formation and impact on brain function. CMBs can be induced either as individual (eg, collagenase microinjection, laser-irradiation) or disseminated lesions (eg, stroke prone and CAA models, cyclodextrin nanoparticles injection, lipopolysaccharides injections and specific diet models inducing hyperhomocysteinaemia). While CMBs do not exert immediate mechanical mass effect on adjacent tissue,30 31 they trigger an early and persistent peri0lesional microgliosis and astrogliosis, responsible for delayed dendrite degeneration and neuronal death.32–34 These secondary brain damages are mediated by the leakage of blood-derived molecules in the parenchyma that promote inflammation and are indirectly responsible for delayed neuronal toxicity.35
CMBs in daily practice
CMB location as marker of the nature of underlying SVD
CMBs are helpful to evaluate the underlying microangiopathy and its severity.36 37 The spatial distribution of CMBs tends to parallel the different anatomical distribution of CAA (mainly affecting cortical and leptomeningeal vessels) and vascular risk factors-related degenerative small vessel changes (ie, arteriolosclerosis that mainly involves the vasculature supplying the supratentorial deep grey nuclei and white matter), and is thus considered a useful MRI biomarker to differentiate these two main forms of sporadic SVD (figure 3).2 36 38 Strictly lobar CMBs are used for CAA diagnosis within the modified Boston criteria.36 They have a high positive predictive value for CAA even in individuals without spontaneous intracerebral haemorrhage (sICH) presentations in a hospital-based setting (specificity 90%).39 However, in the absence of an appropriate clinical context (ie, sICH, convexity subarachnoid haemorrhage, transient focal neurological episodes and cognitive impairment) the overall specificity is low, as lobar CMBs can be found also in the absence of CAA.39 An international collaboration is underway to update and improve the diagnostic test accuracy of the Boston criteria for CAA and provide external validation of the criteria in a large sample.40

{kind=link}
{kind=link}
{kind=link}
Lobar CMBs and deep CMBs share distinct underlying causes and stroke risks. CMBs, cerebral microbleeds; CSO, centrum semi-ovale; cSS, cortical superficial siderosis; EPVS, enlarged perivascular spaces; ICH, intracerebral haemorrhage; IS, ischaemic stroke; WMH, white matter hyperintensities. Estimated risks of first ever strokes and recurrent strokes are adapted from general population based studies and stroke cohorts, respectively (adapted from Akoudad et al, Charidimou et al, Charidimou et al and Imaizumi et al).49 64–66
In the appropriate clinical context (ie, sICH, lacunar stroke, cognitive impairment), strictly deep CMBs are generally thought to be associated with hypertension-related SVD (ie, arteriolosclerosis).38 However in this context, to date no studies have evaluated the diagnostic performance of deep CMBs for the presence of underlying arteriolosclerosis.
Patients with mixed CMBs are of interest since they may exhibit the presence of a severe and diffuse form of arteriolosclerosis or the combination of both CAA and arteriolosclerosis, especially in the elderly.37 41 42 In this context, an underlying hereditary SVD (eg, CADASIL)43 should also be considered, especially in younger patients and if other relevant clinical and radiological features coexist.
The cerebellum may be affected by both types of SVD. In the sICH population, preliminary results suggest that cerebellar CMBs are a frequent finding (44%) and as in supratentorial CMBs they show different distribution patterns (strictly superficial vs deep/mixed cerebellar pattern) (figure 3).44Amyloid positron emission tomography (PET) may provide insights into the pathophysiology of CMBs. Pathology and Pittsburgh compound-B PET-based findings suggest that patients with sICH who harbour CAA as the dominant SVD type mainly show cerebellar CMBs restricted to the superficial cerebellar regions.44 45
CMB prevalence and progression in healthy elderly people
Reported prevalences of CMBs in elderly populations mainly vary according to the mean age of the population, and according to neuroimaging parameters. CMBs are relatively common in older individuals ranging from 5% to 35% in large population-based studies46–49 and cumulative incidences of new CMBs of approximately 7%–10% over a period of 3–4 years.50 51 The reported location of CMBs was predominantly lobar ranging from 48% in the Northern Manhattan Study to 70% in the Age, Gene/Environment Susceptibility–Reykjavik Study.46 47 Deep (ie, basal ganglia, thalami, deep white matter and infratentorial location) and mixed location CMBs (ie, lobar and deep) ranged from 32% in the Rotterdam Scan Study48 49 to 52% in the Northern Manhattan Study.47 Risk factors for CMBs in elderly populations largely differ according to the location of CMBs suggesting different underlying microangiopathies. Lobar CMBs are consistently associated with APOE status (ε4 and ε2) suggesting an association with CAA, even in elderly individuals without neurological disease.52
CMB prevalence and progression in patients who had a stroke
Patients with ischaemic stroke (IS) or sICH typically show higher prevalence and number of CMBs than stroke-free populations in part because they share a higher burden of vascular risk factors. CMBs are frequent among patients with sICH with an estimated prevalence of 60%53 and a recent meta-analysis reports that incident CMBs occur in approximately 40% of patients during a mean 27 months of follow-up after sICH.54 Presence and number of CMBs at baseline have been consistently reported as strong predictors of incident CMBs.54 55 In the context of IS, one patient out of three has at least one CMB.53 In such populations, around 5% of patients exhibit five or more CMBs.56 57 CMB prevalence is also particularly high in patients with genetic diseases of small blood vessels (eg, CADASIL,58 CARASIL,59 hereditary Dutch type CAA,60 COL4A1 mutations61 or other vascular conditions (eg, Moyamoya disease)62 and Fabry disease63.)
CMBs are prognostic markers of both haemorrhagic and ischaemic risks
CMBs are key markers of cerebrovascular risk, which vary according to their location and subgroup populations (figure 3).
In stroke-free individuals, the overall presence of CMBs is associated with a 5.5-fold and 2-fold increased risk of first sICH and first IS, respectively.64 Interestingly the location of CMBs is important: while lobar CMBs are associated with a fivefold increased risk of sICH, it does not seem to influence the IS risk. In contrast, deep CMBs are associated with a 6-fold increased risk of sICH and a 2.5-fold increased risk of IS.49
In patients with a history of sICH, the risk of recurrence depends on both the location of ICH and CMBs. After a lobar sICH, the presence of CMBs (whatever their location) quadruples the risk of recurrence.65 Annual risk of sICH recurrence is lower in patients with mixed (both lobar and deep) sICH and CMBs (5.1% per year), and deep sICH and CMBs (2% per year).65 66
In patients with a history of IS or transient ischaemic attack (TIA), while the presence of CMBs triples the risk of future sICH independently from other confounders, it also increases the risk of IS recurrence by 20%.56 However, we should keep in mind the limits of relative risk comparison since the annual absolute risk of IS is much higher than the absolute risk of sICH. CMBs should be considered as a marker of the severity of the underlying small vessels injuries rather than a specific marker of only future haemorrhagic risk. This double-edged sword gives rise to many clinical dilemmas especially around antithrombotic therapy.
CMBs and cognition
CMBs used to be considered silent, however, they are increasingly recognised as covert lesions.67 To what extent they contribute to cognitive impairment and dementia remains unclear. Two hypothetical mechanisms (that are not exclusive) are usually discussed: CMBs may have a direct lesional effect by disrupting strategic networks,68 69 or their impact on cognition may be the consequence of the underlying diffuse microangiopathy—deep perforating vasculopathy or CAA.70 Growing experimental data suggest that single or disseminated CMBs may be responsible for cognitive decline in rats and mice.33 34 71 72
In humans, capturing the clinical and aetiological complexity of cognitive impairment caused by heterogeneous cerebrovascular lesions (eg, white matter hyperintensities, lacunar infarcts, microinfarcts, large infarcts, cortical superficial siderosis) is a methodological challenge.73 In community-dwelling registries, data on CMBs are conflicting, with some studies showing they are independent predictors of cognitive impairment while others found that the associations with cognition disappears when other vascular brain injury markers such as white matter hyperintensities and infarcts are controlled for. In a systematic review including 8736 participants, CMBs were not associated with risk of incident dementia (OR 1.14; 95% CI 0.9 to 1.41), nor with risk of Alzheimer’s disease (HR 1.18; 95% CI 0.73 to 1.89). The lack of association in some studies may reflect that most individuals had a small number of CMBs, which therefore represent a modest contribution to overall disease burden. This does not preclude any effect of CMBs on dementia risk in a subset of high-risk individuals with more extensive or rapidly progressing lesions.67 In line with this hypothesis, some population-based studies reported that dementia risk was significantly increased in individuals with three or more CMBs.74
The relationship between CMBs and Alzheimer’s disease is intriguing. One patient with Alzheimer’s disease out of five has CMBs.75 Their anatomical distribution tends to be cortico-subcortical with a posterior predominance. The high prevalence of CMBs in Alzheimer’s disease can be explained by the presence of CAA and hypertension which play a role in the pathophysiology of the disease. In this context, CMBs could be a link between the amyloid cascade hypothesis and the neurovascular contribution to AD.76 The presence of CMBs and the quantity of lesions may have prognostic significance and affect cognitive profile.77 However, whether detection of CMBs translates into a clinically meaningful difference remains debatable.78
CMBs are not specific to cerebrovascular diseases or dementia
CMBs have been reported in a wide variety of diseases (see table 1 in the online supplemental file 1).
Supplemental material
CMBs and different antithrombotic regimens; data from randomised trials
Traumatic brain injury
Patients with traumatic brain injury frequently show punctate hypointensities visible on blood-sensitive sequences.79 80 Traumatic CMBs (also known as haemorrhagic diffuse axonal injury in this context) are associated with the severity of the injury, being a frequent finding especially in moderate-to-severe traumatic brain injury patients.81 82 However, a recent study described traumatic CMBs in approximately 30% of patients with mild traumatic brain injury.79 CMBs are consistently associated with poor clinical outcome, doubling the risk of disability at 1 month and 3 months after the injury.79 Traumatic CMBs are typically located in the corpus callosum and at the grey-white matter junction, and in general have a more radial and linear configuration following the perivascular spaces compared with the rounded CMBs that are usually associated with SVD.83 A combined in vivo MRI-ex vivo MRI-histopathology study found iron-laden macrophages in the perivascular space surrounding injured vasculature, suggesting that traumatic CMBs are a marker of traumatic vascular injury.79
Radiation induced
Ionising radiation therapy can cause vascular and parenchymal brain damage leading to CMBs, cavernomas, white matter disease and cerebral atrophy. Chronic radiation-induced endothelial damage leads to fibrinoid necrosis, vessel wall thickening, increased permeability and thrombosis. CMBs as markers of radiation-induced SVD are commonly seen following radiation therapy of paediatric brain tumours and occur in adults. Approximately 50% of children who have undergone cranial radiation treatment develop CMBs.84 In a cohort of patients with medulloblastoma, CMBs were identified in up to 67% of patients with a median latency of 2.8 years during follow-up.85 Young age at time of cranial irradiation is a critical risk factor for the development of CMBs.86 Radiation-induced CMBs have a preferential lobar distribution, and occur particularly in occipital lobes.86
Infective endocarditis
Occult cerebral lesions, in particular CMBs and acute ischaemic lesions, are frequent in infective endocarditis. In a prospective cohort of 130 patients with infective endocarditis who underwent a brain MRI before any surgical intervention, acute ischaemic lesions were observed in 52% and CMBs in 56%. These observations led to a modification in diagnosis and management in nearly one patient out of five.87 In a large cohort of neurologically asymptomatic patients, CMBs were present in 57% and the majority were located in cortical areas (85%).88 In the context of infective endocarditis, CMBs predict occurrence of intracranial haemorrhage, suggesting an increased vascular vulnerability.89 They might reflect blood–brain barrier disruption at the cortico-pial junction secondary to subacute inflammatory microvascular process or a pyogenic vasculitis. However, in this context, CMBs could also represent microemboli with an artery-to-artery embolic mechanism.
Critical medical conditions
In critically ill patients, a number of medical conditions have been associated with the presence of CMBs. In this context, CMBs usually diffusely involve the juxtacortical white matter and corpus callosum and spare the deep and periventricular white matter and the grey matter.90 Some authors suggest that in critically ill patients with respiratory failure one possible mechanism for CMB formation is hypoxaemia which might induce hydrostatic or chemical effects on the blood–brain barrier potentially leading to extravasation of erythrocytes.90 In line with this evidence, CMBs have also been reported with a similar spatial pattern in critically ill patients with COVID-19.91 Other critical medical conditions associated with the presence of CMBs are extracorporeal membrane oxygenation92 and sepsis.93Although one can’t rule out the existence of a chronic ongoing SVD in critically ill patients, these conditions should be considered as contributors to the formation of CMBs.
CMBs: useful biomarkers in the era of precision medicine?
Management of antithrombotic agents
The heightened risk of sICH marked by CMBs has raised concerns regarding antithrombotic treatment in patients with thromboembolic/vaso-occlusive diseases who have CMBs on MRI. Observational data have consistently reported greater rates of future sICH in antithrombotic users with CMBs compared with those without CMBs.57 94–97 Antithrombotic use has additionally been associated with prevalent CMBs in population-based studies.51 98 For instance, in cross-sectional analyses of the Rotterdam Scan Study, antiplatelet and vitamin K antagonist (VKA) users were reported to have a 1.7-fold98 and 1.3-fold51 increased risk of prevalent CMBs, respectively.
Although an association between incident CMBs and antiplatelet therapy has been reported in patients with sICH,55 this has not been consistently reported with anticoagulant therapy (either with VKA or non-vitamin K antagonist oral anticoagulants (NOACs)).51 99 100 These inconsistencies reflect methodological limitations imposed by the observational design of these studies, as well as the heterogeneity in study populations.
Several MRI subgroup analyses of randomised controlled trials (RCTs) have investigated the association between differing antithrombotic regimens and the formation of new CMBs over time in non-sICH populations. These are summarised in table 1. These trials have reported estimated annualised incident CMB rates of 3%–7%, without any apparent differences when comparing between differing antiplatelet monotherapy agents, dual antiplatelet therapy versus monotherapy, or NOAC treatment versus aspirin monotherapy.101–106
Four RCTs have assessed interactions between differing antithrombotic regimens and baseline CMBs for clinical outcomes (table 1). In patients with recent lacunar stroke participating in the SPS3 Trial (n=1278, 30% with CMBs) there were no significant interactions noted between baseline CMB presence and random assignment to combined aspirin/clopidogrel treatment compared with aspirin monotherapy for the outcomes of recurrent stroke and mortality over 3.3 years of follow-up.107 The RESTART Trial recently reported a 35% relative risk reduction in the composite (secondary) outcome of non-fatal myocardial infarction, non-fatal stroke and vascular death (p=0.025) in patients with sICH with concomitant thromboembolic/occlusive diseases who were randomised to antiplatelet therapy compared with no antithrombotic therapy, without potential for a meaningful increase in the primary outcome of recurrent sICH (adjusted HR 0.51; 95% CI 0.25 to 1.03).108 In the subgroup analyses of the 235 participants with CMBs from the RESTART Trial, neither the presence, burden or the location of CMBs influenced the effects of antiplatelet therapy on recurrent sICH.109
Interestingly in the PICASSO Trial, the risk of sICH was lower with cilostazol than aspirin (0.12%/year vs 1.49%/year; HR, 0.08; 95% CI 0.01 to 0.60) in participants with IS and baseline CMBs, but was not different between the two treatment arms (1.26%/year vs 0.79%/year; HR 1.60; 95% CI 0.52 to 4.90) in participants with prior sICH (p interaction=0.011).110 These preliminary observations require validation in a confirmatory trial. With regard to anticoagulation, there were no interactions identified between baseline presence, location or severity of CMBs and rivaroxaban 15 mg daily compared with aspirin for the outcomes of IS, ICH or mortality over 11 months of follow-up in NAVIGATE ESUS participants (n=3699, 11% with CMBs).111 In particular, there was no suggestion of a treatment effect for the outcome of sICH (participants with CMBs: HR 3.1, 95% CI 0.3 to 30.0; without CMBs: HR 3.0, 95% CI 0.6 to 14.7; interaction p=0.97).
The totality of the literature to date indicates that CMBs can serve as prognostic markers for heightened sICH risk in patients with cerebrovascular disease, but their presence does not seem to modify the effect of antithrombotic therapy on clinical outcomes. Hence, their use in guiding antithrombotic therapy decision making remains questionable. The net benefit analysis of antithrombotic treatment in patients with CMBs needs to also incorporate the future risk of ischaemic events. In fact, absolute rates of IS are reported to overshadow the absolute rates of sICH in IS/TIA populations, irrespective of the baseline severity of CMB burden or patterns suggestive of CAA pathology.56 57 It is particularly important to keep in mind that in the context of atrial fibrillation, rates of IS stratified by CMB severity and location that are reported in anticoagulated cohorts,57 97 are estimated to be ~threefold higher, should these patients be withheld anticoagulation. It has even been estimated that patients with IS/TIA with atrial fibrillation and CMBs may have greater net benefit from anticoagulant therapy than patients without CMBs, due to their much higher absolute IS rates.112 As CMBs mark a heightened risk of both ischaemic and haemorrhagic events, and the absolute rates of ischaemic events are much greater than haemorrhagic ones in non-sICH populations, the utility of incorporating them into risk scores (such as the HAS-BLED or HEMORR2HAGES) is then questionable and depends on the intended purpose of the scale. CMBs can provide additional insights when it comes to natural history and prognostication of future vascular events, and could influence more aggressive treatment of risk factors such as hypertension. However, the stroke community needs to exercise considerable caution to ensure that these emerging risk scores are not used to dissuade antithrombotic treatments, particularly in already undertreated populations such as atrial fibrillation. Current evidence does not justify withholding these evidence-based treatments from patients who had a stroke solely on the basis of CMBs on MRI. Whether the presence of CMBs can modify the effect of anticoagulation in sICH survivors with atrial fibrillation towards net harm has yet to be assessed in RCTs and remains uncertain. MRI substudies of several ongoing trials will ultimately provide more insights in this regard.113
Reperfusion therapies for acute IS and CMBs
The majority of patients enrolled in RCTs of intravenous thrombolysis (IVT) for acute IS did not undergo MRI before randomisation and therefore their CMB burden is unknown. In a meta-analysis of nine observational studies evaluating the safety of IVT for acute IS, the presence of at least one CMB was observed on pretreatment MRI in 23.4% (581/2479) of included patients, and was associated with a twofold increased risk of symptomatic ICH.114 Of note, the incidence rate of symptomatic ICH was not excessively increased in patients with ≥1 CMBs, (6.5%, 95% CI 4.8% to 8.9%) compared with patients without CMBs (4.4%, 95% CI 3.5% to 5.4%).114 However, in the very small subgroup of 15 patients (0.8% of included subjected) with >10 CMBs, symptomatic ICH incidence was disproportionately high reaching 46.9% (95% CI 22.8% to 72.5%).114 The former observations were reproduced in an individual patient data meta-analysis of 1973 patients with acute IS receiving IVT that reported the presence of ≥1 and >10 CMBs in 526 (26.7%) and 35 (1.8%) patients, respectively.115 The association between CMB presence (≥1) and symptomatic ICH failed to reach statistical significance (adjusted OR (aOR) =1.42, 95% CI 0.86 to 2.35), but a count of >10 CMBs was strongly related to increased odds of symptomatic ICH (aOR=3.65, 95% CI 1.17 to 11.42), remote parenchymal haemorrhage (aOR=9.09, 95% CI 3.25 to 25.40) and poor functional outcome (adjusted OR 3.99, 95% CI 1.55 to 10.22).115
Interestingly, a recent study using a multistep algorithm populated with data from clinical studies to estimate 3-month clinical and imaging outcomes in patients with acute IS with high CMB burden (>10 CMBs) treated with IVT reported the following findings: (A) the beneficial treatment effect of IVT on 3-month functional outcome was attenuated in patients with >10 CMBs compared with patients with ≤10 CMBs on pretreatment brain MRI; (B) IVT was related to an increased risk of mortality in patients with >10 CMBs; (C) IVT might be related to net harm in subgroups of patients with >10 CMBs defined by age, stroke symptom severity and treatment delay; nevertheless, (d) Routine pretreatment MRI to quantify CMB burden before IVT cannot generally be recommended, as long as it causes even a small additional treatment delay given the low general pretest probability of >10 CMBs (0.6%–2.7%).116 However, these inferences derived from observational data need to be treated cautiously. CMBs should be factored into a holistic individual-based risk-benefit analysis to determine treatment suitability, rather than serve as go/no-go criteria of themselves. The current American Heart Association guidelines for acute IS management advocate the following recommendations: (A) In otherwise eligible patients who have had a previously demonstrated small number (1–10) of CMBs on MRI, IVT administration is reasonable (class of recommendation IIa; level of evidence B, non-randomised); (B) In otherwise eligible patients who have had a previously demonstrated high burden of CMBs (>10) on MRI, IVT may be associated with an increased risk of sICH, and the benefits of treatment are uncertain (class of recommendation IIb; level of evidence B, non-randomised); (C) Routine use of brain MRI to exclude CMBs before IVT is not recommended (class of recommendation III; level of evidence B, non-randomised).117
There are limited observational data indicating that CMB presence on pretreatment brain MRI is not associated with increased risk of symptomatic ICH and adverse functional outcomes in acute IS due to large vessel occlusion receiving mechanical thrombectomy with or without IVT pretreatment.118 119 A recent meta-analysis including 598 patients with large vessel occlusion treated with endovascular reperfusion therapy reported that the pooled relative risk of ICH was 0.90 (95% CI 0.65 to 1.25) in patients with CMBs (18% of included patients) versus those without CMBs.120 In view of these considerations, it is recommended that CMB presence or burden should not represent an exclusion criterion for mechanical thrombectomy in patients with large vessel occlusion.
Lipid-lowering therapies and CMBs
Although statins have established safety and efficacy in primary and secondary stroke prevention, concerns arose about a possible increased risk of sICH.121 Independent of their cholesterol-lowering properties,122 pleiotropic effects of statins on coagulation and fibrinolysis have been discussed.123 However, data from clinical studies remain conflicting. A brain MRI substudy of an RCT documented that there were no statistically significant differences in the risk of incident CMBs between the rosuvastatin and placebo groups, while no significant interactions were detected between rosuvastatin use and APOE ε4 status regarding new CMBs.124 Similarly, statin pretreatment was not associated with CMB presence among patients who had an acute cardioembolic stroke who were anticoagulation-naïve.125 Finally, there are conflicting data regarding the potential association of statin pretreatment with CMB presence or burden in patients with acute ICH (spontaneous126 or anticoagulation-associated127). In view of the former associations, CMB presence or high burden on brain MRI should not be used to withhold statin therapy for otherwise eligible patients in the settings of primary and secondary stroke prevention. Lastly, there are scarce if any available data regarding the potential association of other lipid-lowering therapies (eg, fibrates, proprotein convertase subtilisin/kexin type 9 inhibitors) with incident sICH in patients with CMBs on baseline MRI.
Conclusion
Huge efforts have been made to better understand the meanings of CMBs over the last decades but important issues remain to be clarified in the future (table 2). CMBs are important markers of the nature of the ongoing microangiopathy and they highlight the fact that microangiopathies are not exclusively occlusive disease. The practical clinical value for their detection has yet to be further established. To date, they are not essential to tailor our therapeutic decisions but they provide precious insights for prognostication of future vascular events. In future trials targeting SVD progression, they also could be valuable biomarkers.
Research perspectives
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Lau_Puy
Contributors PL, MP, MR, SJvV, GT, AS and CC contributed to the conception and structure of the review, drafted the text and prepared the figures.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AS reports grants and personal fees from Daiichi Sankyo Inc., grants and personal fees from Bayer AG, grants and personal fees from Servier Canada Inc., grants from Bristol-Myers Squibb, outside the submitted work; CC reports grants and personal fees from Boehringer-Ingelheim (speaker fees), BMS (steering committee), French ministry of health (grant A3ICH trial).
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.