Article Text

Abstract
Objective To assess the burden of paediatric traumatic brain injury (TBI) on neurocognition via a systematic review and meta-analysis.
Methods Studies that compared neurocognitive outcomes of paediatric patients with TBI and controls were searched using Medline, Embase, PsycINFO and Cochrane Central Register of Controlled Trials, between January 1988 and August 2019. We presented a random-effects model, stratified by TBI severity, time of assessment post injury and age.
Results Of 5919 studies, 41 (patients=3717) and 33 (patients=3118) studies were included for the systematic review and meta-analysis, respectively. Studies mostly measured mild TBI (n=26, patients=2888) at 0–3 months postinjury (n=17, patients=2502). At 0–3 months postinjury, standardised mean differences between TBI and controls for executive function were −0.04 (95% CI −0.14 to 0.07; I2=0.00%), −0.18 (95% CI −0.29 to –0.06; I2=26.1%) and −0.95 (95% CI −1.12 to –0.77; I2=10.1%) for mild, moderate and severe TBI, respectively; a similar effect was demonstrated for learning and memory. Severe TBI had the worst outcomes across all domains and persisted >24 months postinjury. Commonly used domains differed largely from workgroup recommendations. Risk of bias was acceptable for all included studies.
Conclusion A dose-dependent relationship between TBI severity and neurocognitive outcomes was evident in executive function and in learning and memory. Cognitive deficits were present for TBIs of all severity but persisted among children with severe TBI. The heterogeneity of neurocognitive scales makes direct comparison between studies difficult. Future research into lesser explored domains and a more detailed assessment of neurocognitive deficits in young children are required to better understand the true burden of paediatric TBI.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
Introduction
Globally, traumatic brain injury (TBI) affects three million children annually and is a leading cause of death and disability.1 Children with moderate to severe TBI experience deficits that persist into adulthood, affecting educational, employment and psychosocial outcomes.2 3 The Centers for Disease Control and Prevention identified poor understanding of the long-term consequences of paediatric TBI as an important gap resulting in inadequate care.4
Published studies exploring the neurocognitive effects of TBI vary in cognitive domains studied, severity of TBI assessed and timeframe for evaluation.2 5 The most recent meta-analysis reviewed data from 1988 to 2007 and reported that children with moderate to severe TBI had significant impairments in various cognitive domains (intellectual function, processing speed, attention, fluency, inhibition, problem-solving and memory).2 Since this publication, the classification of cognitive domains has been updated by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V).6 To date, no systematic review or meta-analysis on TBI neurocognitive changes has used this new classification. Determining the burden of paediatric TBI on neurocognition using the updated cognitive domains will allow for a better understanding of this vulnerable population and facilitate future research in this area.
We aimed to summarise evidence from January 1988 to August 2019 and perform an updated systematic review and meta-analysis on neurocognitive outcomes of children with TBI. We purposed to compare them with controls (either healthy or with single-system orthopaedic injury) in the DSM-V cognitive domains: complex attention, executive function, learning and memory, language, perceptual-motor function, and social cognition.6 In addition, we hypothesised that there are worse outcomes in children with TBI compared with controls, for any severity (mild, moderate or severe) across one or more of the six defined cognitive domains, across any time-point.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.7 This study is registered with PROSPERO (International Prospective Register of Systematic Reviews; CRD42020152680).
Selection criteria
Studies containing elements of the Population Exposure Comparator Outcome (PECO) format were searched.8 We defined the population as children 18 years or younger. We defined the exposure, TBI, as ‘an alteration in brain function, or other evidence of brain pathology, caused by an external force’ and graded by the Glasgow Coma Scale (GCS), where mild, moderate and severe TBI correspond to GCS scores 13–15, 9–12 and 3–8, respectively.9 10 The control group comprised healthy children and those with single-system orthopaedic injury. Single-system orthopaedic injury refers to an isolated lower extremity orthopaedic injury without injuries to other body systems.11 We chose to include both control groups because the literature search revealed that many studies used either group as a comparator. Specifically, for hospital-based studies, single-system orthopaedic injuries were often used as the control group. When data from both control groups (healthy and single-system orthopaedic injury) were available, the healthy group was preferentially selected. Neurocognition is defined as ‘the neural processes involved in the linking and processing of information, and comprises traditional neurocognitive domains found throughout the literature on TBI’.6 We matched the neurocognitive outcomes to DSM-V cognitive domains: complex attention, executive function, language, learning and memory, perceptual-motor function, and social cognition. We defined the outcome as a change in neurocognition at the following time-points: <24 hours, 0–3 months, 3–6 months, 6–12 months, 12–18 months, 18–24 months and >24 months. We included studies where the sample size for TBI in each severity group was at least 30 to prevent selection bias that may be present in small studies.12 We included papers published from 1988 to 2019.2 Only randomised controlled trials, cohort, case–control and cross-sectional studies were included. Systematic reviews were used to verify that relevant studies were included and were not used as part of the final set of studies analysed. Studies were excluded if they studied non-TBIs, were not peer-reviewed or not in English.
Search strategy
The literature search was conducted on 26 August 2019 via Medline, Embase, Cochrane Central Register of Controlled Trials and PsycINFO, in accordance with Cochrane Handbook guidelines.13 The search strategy was developed with input from a medical librarian and peer-reviewed by an independent search strategist. It was piloted in Medline using medical subject headings (MeSH) and refined using key articles found in preliminary searches.14 15 The Medline (Ovid interface) search strategy was consistent across all databases (online supplemental table 1). Strategic search terms included paediatric, child, adolescent, traumatic brain injury, head injury, cognition and neurocognitive disorder. We hand-searched the reference list of systematic reviews and meta-analyses for relevant articles that were missed by the above search. We ensured there were no concurrent studies by searching PROSPERO, ClinicalTrials.gov, International Standard Randomised Controlled Trial Number registry, WHO International Clinical Trials Registry Platform and European Union Clinical Trials Register.
Supplemental material
Top measures per neurocognitive domain
Data collection
Covidence (Veritas Health Innovation, Australia, V.1499) was used. Studies were first screened by title and abstract, with only PECO elements, and subsequently screened by full text where the eligibility criteria were applied. Reasons for each exclusion were recorded. Two reviewers independently screened each article during both stages. Conflicts were resolved by a third independent reviewer or through discussion. Neither of the reviewers were blinded to journal titles, study authors or institutions. Outcome estimates in the form of group data were sought. Two independent reviewers extracted the data using a standardised form on Microsoft Excel (Microsoft, USA). Studies that met the inclusion criteria but did not provide a detailed breakdown (eg, studies that comprised data spanning children and adults) were included if the authors provided the data after we contacted them. Differences in the data extracted were resolved through discussion. The standardised form included all variables of interest (online supplemental table 2). Measures used to assess neurocognition were each assigned a cognitive domain, based on DSM-V.
Common measures per neurocognitive domain against CDE recommended measures
Summary measures
For the systematic review, we performed a narrative synthesis on the various outcome measures and their usage over time. Standardised mean differences (SMDs) were calculated between TBI and control groups for each study. Later, all SMDs were pooled using a DerSimonian and Laird method of inverse variance random-effects model.16 SMDs from individual studies and pooled results are presented in forest plots with 95% CI. All statistical analyses were done using Comprehensive Meta-Analysis V.3 (Biostat, USA).
Heterogeneity assessment
The I² statistics quantified heterogeneity between studies.17
Publication bias
Publication bias was evaluated using Egger’s test and funnel plots.18
Data analysis
Results from each outcome measure within each neurocognitive domain were analysed separately. Each domain-wise analysis was stratified by TBI severity and time-point. We used each assessment as a unique data point as each patient may be assessed using different measures at different time-points. To avoid within-subject correlation, no overall pooling was done. Outcome estimates were then compared longitudinally within each TBI severity. Mean (SD) was extracted from all included studies. If studies reported the outcome as median (IQR or range), mean (SD) was estimated manually.19 We chose the most frequently used outcome measures (used three or more times in independent studies) in each cognitive domain and calculated the SMD effect sizes. We then stratified our data and presented this in a forest plot according to TBI severity and time-point.
Meta-regression
Meta-regression by age (0–5 and 5–18 years old)2 was performed to evaluate differences in cognitive deficit between the two groups.
Risk of bias
We assessed the risk of bias (RoB) using the Scottish Intercollegiate Guidelines Network criteria for randomised controlled trials, cohort and case–control studies, and the National Heart, Lung, and Blood Institute tool for cross-sectional studies.20 21 An overall rating of high quality, acceptable, low quality or unacceptable was given to each study, evaluated by two independent assessors.
Published protocol
The protocol is available online.22
Results
Study selection
Among 5919 articles screened, 41 studies met the inclusion criteria and 33 were used in the meta-analysis (figure 1, online supplemental table 3). The excluded studies are listed in online supplemental table 4.
Study characteristics and design
The 41 studies (total patients=3717) included in the systematic review were published between 1992 and 2018, with an increase in publications on learning and memory and on complex attention in 2012 (online supplemental figure 1).11 s1–s40 Participants were recruited from the USA, Canada, Australia, Sweden, Switzerland and the Netherlands (online supplemental table 3). Twenty-four studies (58.5%) measured mild TBI,11, s1–s4, s6, s12, s15–s17, s19, s21–s25, s28–s31, s33, s38–s40 seven studies (17.1%) measured moderate TBI,s7, s14, s18, s26–s27, s36–s37 six studies (14.6%) measured severe TBI,s5, s8, s9, s20, s32, s34 while two studies (4.9%) measured both mild and severe TBIs10–s11 and two studies (4.9%) measured both moderate and severe TBI.s16, s35 There were 26 cohort studies,11 s4, s10–s15, s17–s19, s21–s25, s28–s31, s34–s36, s38–s40 14 cross-sectional studiess1, s2, s5–s9, s16, s20, s26–s27, s32–s33, s37 and 1 case–control study.s3 There were 26 prospective studies11 s3–s4, s8–s14, s17–s19, s21–s22, s25–s26, s28–s31, s34–s36, s38–s39 and 15 retrospective studies.s1–s2, s5–s7, s15–s16, s20, s23–s24, s27, s32–s33, s37, s40 Study setting was split between 26 hospital-based,11 s4, s8–s14, s17–s25, s29, s31, s33–s36, s38–s39 11 register-based,s2, s5–s7, s15–s16, s26–s28, s30, s40 2 clinical-baseds32, s37 and 2 referral-based.s1, s3 There were different numbers of studies reporting on each time-point, the most frequently reported being 0–3 months for mild and moderate TBI and 6–12 months for severe TBI (online supplemental table 5). Seventy-two different outcome measures were used across all cognitive domains. The most common measures used in each domain are documented in table 1.

PRISMA flow chart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. TBI, traumatic brain injury.

{kind=link}
{kind=link}
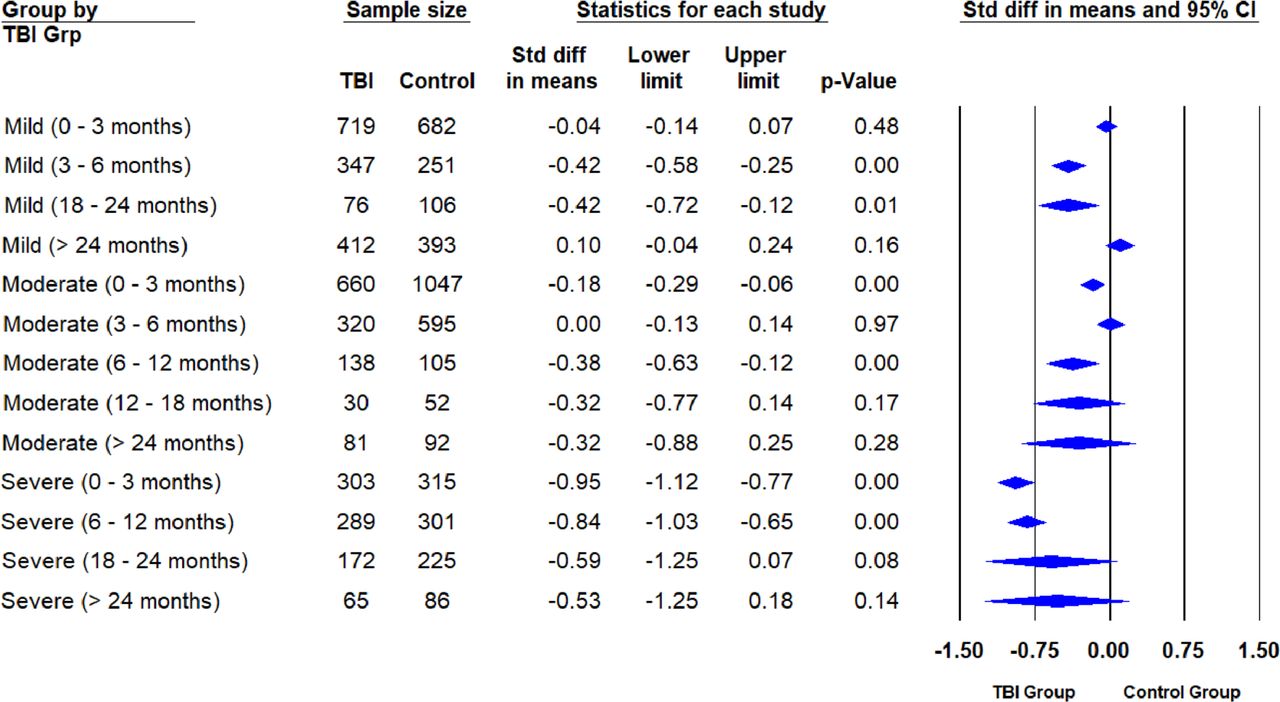
Forest plot of executive function stratified by TBI severity and time-point. Effect sizes in SMD are compared between TBI and control groups where deficits favouring the TBI group are negative and deficits favouring the control group are positive. SMD, standardised mean difference; Std diff, standardised difference; TBI, traumatic brain injury.
Outcome measures reported
Overall, 33 (80.5%) of 41 studies (total patients=3118) employed outcome measures that were used three or more times in other studies and were included in the meta-analysis.11, s2–s10, s13–s14, s16–s23, s25–s31, s34–s35, s37–s40 The number of studies with common outcome measures within each cognitive domain was 14 (77.8%) for complex attention, 20 (74.1%) for executive function, 15 (62.5%) for learning and memory, 6 (35.3%) for language, 5 (50.0%) for perceptual-motor function, and 5 (83.3%) for social cognition. The common measures used for each domain were the Wechsler Intelligence Scale for Children (WISC) for executive function (n=12, 44.4%), complex attention (n=7, 38.9%), language (n=5, 29.4%) and perceptual-motor function (n=4, 40.0%), the California Verbal Learning Test (CVLT) for learning and memory (n=7, 29.2%), and the Emotional and Emotive Faces Task (EEFT) for social cognition (n=5, 83.3%), where n refers to the number of publications. A shift in common measures used was noted in 2008, while WISC was used consistently from 1992 through 2015 (online supplemental figure 2).
Complex attention
Estimates for complex attention showed worse outcomes in mild TBI at <24 hours (SMD=−0.36, 95% CI −0.70 to –0.01), with resolution by 3–6 months (SMD=−0.13, 95% CI −0.35 to 0.09) (online supplemental figure 3). Heterogeneity was substantial between studies with results at <24 hours (I²=72.3%, p=0.003); however, heterogeneity was low for studies examining outcomes at 3–6 months (I²=33.7%, p=0.197) (online supplemental table 6). The funnel plot showed no evidence of small-study effects, supported by Egger’s test (p=0.948) (online supplemental figure 4). There were no estimates for moderate to severe TBI in the domain of complex attention.
Executive function
Pooled estimates for executive function showed a dose-dependent relationship between TBI severity and outcomes. At 0–3 months, the SMD was −0.04 (95% CI −0.14 to 0.07), –0.18 (95% CI −0.29 to −0.06) and −0.95 (95% CI −1.12 to –0.77) for mild, moderate and severe TBI, respectively (figure 2). This pattern was similar at 6–12 months, 18–24 months and >24 months. Patients with mild TBI showed resolution at >24 months (SMD=0.10, 95% CI −0.04 to 0.24), while those with severe TBI continued to show worse outcomes at >24 months (SMD=−0.53, 95% CI −1.25 to -0.18). Heterogeneity was low at 0–3 months for studies involving mild (I²=0%, p=0.948), moderate (I²=26.1%, p=0.188) and severe (I²=10.1%, p=0.349) TBI and at >24 months for mild TBI (I²=0%, p=0.909) (online supplemental table 7). There was considerable heterogeneity at >24 months for severe TBI (I²=78.5%, p=0.031). Small-study effects were shown by funnel plot, supported by Egger’s test (p<0.005) (online supplemental figure 5).
Learning and memory
Pooled estimates for learning and memory also showed a dose-dependent relationship. At 0–3 months, SMD was −0.21 (95% CI −0.28 to –0.14), −0.22 (95% CI −0.41 to −0.03) and −1.00 (95% CI −1.18 to –0.83) for mild, moderate and severe TBI, respectively (online supplemental figure 6). In patients with mild TBI, this resolved by >24 months (SMD=−0.05, 95% CI −0.25 to 0.15), while those with severe TBI showed worse outcomes at 18–24 months (SMD=−0.79, 95% CI −0.97 to –0.60). Heterogeneity was low at 0–3 months for studies of mild (I²=30.7%, p=0.078) and moderate (I²=0%, p=0.396) TBI, at >24 months for mild TBI (I²=0%, p=0.996), and at 18–24 months for severe TBI (I²=0%, p=0.476) (online supplemental table 8). Heterogeneity was moderate at 0–3 months for severe TBI (I²=56.0%, p=0.006). Small-study effects were shown by funnel plot, supported by Egger’s test (p<0.001) (online supplemental figure 7).
Language, perceptual-motor function and social cognition
Overall pooled estimates for language, perceptual-motor function and social cognition showed no change with mild TBI at all time-points. Where data were available for severe TBI, deficits were shown across all time-points. Data for effect sizes, heterogeneity tests and publication bias can be found in online supplemental figures 8-13 and online supplemental tables 9–11.
Summary of findings
The dose-dependent relationship of TBI severity and adverse outcomes was seen across all domains. It was observed at 0–3 months for executive function and for learning and memory. In patients with mild TBI, only executive function remained affected at 18–24 months. Patients with severe TBI consistently showed worse outcomes in all cognitive domains across all time-points.
Meta-regression by age
Meta-regression was performed accounting for TBI severity and age. Data stratified by age (0–5 and 5–18 years old) were only available for executive function. Out of the 20 studies included in the meta-analysis for executive function, 2 (10.0%) studies included patients <5 years old,s13, s34 16 (80.0%) studies included patients 5–18 years old,s4, s6–s8, s15–s18, s21–s22, s25, s30, s33 and 2 (10.0%) studies did not report ages.s3, s19 Severe TBI (as compared with mild) and young age <5 years were both independently associated with poorer executive function scores (−0.62, 95% CI −0.77 to −0.47; and −0.39, 95% CI −0.56 to −0.21). Across all severities, young age <5 years was clearly associated with poorer executive function scores (online supplemental table 12).
Risk of bias
RoB assessments (online supplemental tables 13–15) showed that studies were generally well designed and directly applicable. All had a quality rating of ‘fair’. However, three assessments (5.8%) rated two cohort studies as not having comparable comparison groups.s22, s40 In most studies, the demographics of the control groups were comparable with the TBI groups (online supplemental table 16). Three assessments (5.8%) indicated that two cohort studies lacked a clear method of TBI assessment.s13, s19 Thirteen assessments (46.4%) over eight cross-sectional studies showed <50% participation rate.s1–s2, s5–s6, s8, s16, s32–s33
Discussion
In this systematic review and meta-analysis, we demonstrated that greater neurocognitive deficits are associated with greater injury severity. This dose-dependent relationship was evident in executive function and in learning and memory. These domains were well studied, contained common outcome measures and supported by sufficient studies to observe such a trend. Our results showed that the longer the time from injury, the less the cognitive deficit, in keeping with the anticipated course of recovery.23 24 Neurocognitive deficits in executive function remain for extended periods, up to 18–24 months for mild TBI and >24 months for severe TBI.
Impact of mild TBI findings
Our findings challenge the notion that mild TBIs ‘tend to resolve within weeks or days after the injury with complete resolution typically by 3 months’,6 which guides mild TBI return-to-play protocols. Currently, many patients do not receive follow-up care despite remaining symptomatic. As such, formal follow-up may be beneficial for these patients.25 Mild TBI resulted in deficits in complex attention, executive function, and learning and memory. For the remaining domains of language, perceptual-motor function and social cognition, our review did not show worse outcomes in patients with mild TBI, across all time-points. This was similar to several small-group findings.26–28
Impact of moderate and severe TBI findings
For patients with moderate TBI, deficits in executive function and in learning and memory were found at 0–3 months and resolved by 12–18 months. Children with severe TBI were better studied with domains spanning from executive function, language, learning and memory, to perceptual-motor function, with worse outcomes across all time-points. Although acute management of severe TBI is guided by established treatment algorithms, there is limited evidence to guide rehabilitation.29 30 Our study demonstrated a significant cognitive decline in patients with severe TBI across multiple domains, highlighting the urgent need for coordinated efforts to guide high-quality rehabilitation in children with severe TBI.
Age stratification
There were greater deficits in patients 0–5 years old compared with patients 5–18 years old. The younger the child, the more vulnerable the developing brain is to trauma.31 The postnatal brain continues to undergo development and refinement, with sensitive periods of critical growth.32 Because brain maturation is not linear, TBI that occurs during periods of marked plasticity can severely blunt the developmental trajectories of these young children and devastate their potential, resulting in long-term physical, cognitive, psychological and emotional impairments.33 This confirms previous findings and highlights the importance of timely and effective TBI management and rehabilitation to mitigate the poorer prognosis in this vulnerable group.34 Postinjury, the young child’s brain is constantly remodelling to encode new learning experiences.35 Key drivers of effective rehabilitation include training-based interventions that induce neuroplasticity, enriching the child’s learning environment and enhancing interactions between the child and the caregivers.36 A multidisciplinary team is often needed to provide the injured child with physiotherapy, occupational therapy, and balance, psychological and cognitive therapy.37
Discrepancy in outcome measures
Excluding learning and memory, we found that the measures commonly used in the other domains had important discrepancies with the current Common Data Elements (CDE) workgroup recommendations (table 2).38
This highlights an important need for researchers to use common platforms. Considering the trend in measures used after 2005 (online supplemental figure 2), the most common measures used by studies and CDE recommendations, we recommend that WISC be considered for measuring complex attention, executive function, language and perceptual-motor function, CVLT for learning and memory, and EEFT for social cognition. The use of CDE will help comparison of outcomes to improve long-term neurocognitive outcomes in children with TBI.
Strengths and limitations
Our study has several strengths. We employed cognitive domains that categorise neurocognitive deficits well. We pooled the most common outcome measures used per domain to better elucidate the true neurocognitive burden. A wide range of time-points allowed us to track trends consistently. We also attempted to stratify the neurocognitive outcomes by age. However, we recognise that this study has important limitations. First, the use of MeSH terms was limited as there were no MeSH terms related to social cognition. Second, the use of DSM-V cognitive domains excluded factors that may be indirectly related to cognition. Social aggression, for example, may not directly affect cognition, but may affect decision-making and social function. Third, the criteria of a minimum sample size of 30 excluded studies with small samples sizes. The purpose was to reduce bias from small studies, but we recognise that important data could be missed out in the process. Fourth, we chose to focus on common measures within each domain for the meta-analysis, assuming that these outcome measures are truly representative of each neurocognitive domain.38 Due to the lack of available data, we were also unable to account for the impact of important confounders, specifically that of deprivation on children who may not have the benefit of early education at baseline, nor received robust neurorehabilitation postinjury. This would be especially pertinent for children <3 years old with significant brain plasticity, since injuries at this age could devastate subsequent developmental trajectories. Lastly, a large number of the studies included in the meta-analysis were from North America and Australia. Future work with a global representation will be needed to confirm our findings.
Sources of heterogeneity in the included studies were from demographic, physiological, clinical and methodological factors. Demographic heterogeneity is from multiple background differences including parental and child education and psychological and emotional factors that make up a child’s environment. Clinical heterogeneity results from different mechanisms of injury, severity, acute management and assessment of children with TBI. Performing a meta-analysis using the random-effects model, subgroup analysis or meta-regression is a way to account for heterogeneities. We used the random-effects model but could not perform a robust meta-regression or subgroup analysis due to non-availability or inadequate data on the above-mentioned factors. However, we managed to do meta-regression using age by categorising into age groups of ≥5 or <5 years old.
Conclusion
This study highlights the true global burden of TBI on neurocognition and demonstrates a dose-dependent and time-dependent relationship between TBI severity and outcomes. Severe TBI causes long-term devastation in multiple cognitive domains. The younger the child, the greater the brain’s neuroplasticity at the point of injury, and therefore the greater the devastation. An important discrepancy was shown between recommended measures for cognitive assessment and current scales used by researchers. Future research into lesser explored domains and assessment of neurocognitive deficits in young children are required to better understand the long-term consequences of paediatric TBI.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Acknowledgments
We would like to thank Miss Peggy Fong, chief librarian at KK Women’s and Children’s Hospital, Singapore, for tirelessly helping us with the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MSLG and S-LC coordinated the study. MSLG, DSHL and S-LC developed the search strategy and registered the protocol. MSLG, DSHL, JLG, SSMG and S-LC reviewed the studies. MSLG, DSHL, S-LC and JLG extracted data from the studies and conducted risk of bias assessments. RS conducted the statistical analyses. MSLG, RS, JHL and S-LC performed the data interpretation. MSLG drafted the manuscript. S-LC, MSLG, JHL, RS, DSHL, JLG and SSMG helped to revise the manuscript. All authors read and approved the final manuscript.
Funding This review is financially supported by the Academic Medicine – Enhancing Training, Healthcare, Outcomes and Standards (ETHOS) Duke-NUS Medical Student Fellowship (AY2019-AY2020). Duke-NUS was not involved in the design of the protocol and analysis plan of the review and will not provide input on the interpretation of the results.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.