Article Text

Abstract
Objectives Long COVID is a major public health issue. Whether long COVID is comorbid with psychiatric disorders remains unclear. Here, we investigate the association between long COVID, psychiatric symptoms and psychiatric disorders.
Design Cross-sectional.
Settings Bicêtre Hospital, France, secondary care.
Participants One hundred seventy-seven patients admitted in intensive care unit during acute phase and/or reporting long COVID complaints were assessed 4 months after hospitalisation for an acute COVID.
Main outcome measures Eight long COVID complaints were investigated: fatigue, respiratory and cognitive complaints, muscle weakness, pain, headache, paraesthesia and anosmia. The number of complaints, the presence/absence of each COVID-19 complaint as well as lung CT scan abnormalities and objective cognitive impairment) were considered. Self-reported psychiatric symptoms were assessed with questionnaires. Experienced psychiatrists assessed Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition-based diagnoses of psychiatric disorders.
Results One hundred and fifteen (65%) patients had at least one long COVID complaint. The number of long COVID complaints was associated with psychiatric symptoms. The number of long COVID complaints was higher in patients with psychiatric disorders (mean (m) (SD)=2.47 (1.30), p<0.05), new-onset psychiatric disorders (m (SD)=2.41 (1.32), p<0.05) and significant suicide risk (m (SD)=2.67 (1.32), p<0.05) than in patients without any psychiatric disorder (m (SD)=1.43 (1.48)). Respiratory complaints were associated with a higher risk of psychiatric disorder and new-onset psychiatric disorder, and cognitive complaints were associated with a higher risk of psychiatric disorder.
Conclusions Long COVID is associated with psychiatric disorders, new-onset psychiatric disorders and suicide risk. Psychiatric disorders and suicide risk should be systematically assessed in patients with long COVID.
- COVID-19
- psychiatry
- depression
- behavioural disorder
Data availability statement
Data may be obtained from a third party and are not publicly available. Not applicable.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Long COVID is a lingering syndrome that affects patients after an infection by SARS-CoV-2.
Psychiatric disorders are frequent after COVID-19.
WHAT THIS STUDY ADDS
Four months after a hospitalisation for COVID-19, psychiatric disorders, significant suicide risk and psychiatric symptoms are associated with long COVID.
Psychiatric disorders are particularly associated with respiratory and cognitive complaints.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Patients with long COVID should benefit from psychiatric assessment.
Introduction
Following the outbreak of the COVID-19 pandemic in the early months of 2020—a period associated with a high number of deaths and issues about critical care—the persistence of an invalidating medical condition later named ‘long COVID’ was observed in many survivors of the infection. Long COVID, a lingering syndrome affecting 30%–80% of patients who have been infected with SARS-CoV-2, is now recognised as a major public health issue.1–3 For WHO, a post-COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months following the onset of COVID-19, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis.3 For the US Centers for Disease Control and Prevention, ‘post-COVID-19 conditions’ is an umbrella term for the wide range of health consequences that are present 4 or more weeks after an infection with SARS-CoV-2.4 For the British National Health Service, long COVID is defined by the presence of symptoms that develop during or after COVID-19, continue for >12 weeks after acute COVID-19 infection, and which cannot be explained by another cause.5 The most frequently reported long COVID complaints include persistent fatigue, respiratory complaints, cognitive complaints, muscle weakness, persistent pain, headache, paraesthesia and anosmia.2 6–10 Objective criteria have also been proposed for the definition of long COVID syndromes, such as CT lung scan abnormalities or objective cognitive impairment.11 12 To date, long COVID is mostly studied in patients who were not hospitalised for the acute COVID-19 infection.3
Psychiatric symptoms, such as insomnia, anxiety, depressive and post-traumatic stress symptoms, are frequent after an acute COVID-19.11–15 Interestingly, an association between psychiatric complaints and long COVID somatic complaints has been observed (eg, anxiety symptoms with respiratory complaints, cognitive complaints and depressive symptoms with respiratory complaints, myalgia and cognitive complaints15–18).
Beyond psychiatric symptoms, 20%–25% of patients are diagnosed with a psychiatric disorder 3–6 months after COVID-19.19–21 A recent systematic review22 showed that the pandemic provoked an additional 53.2 million cases of major depressive disorder and an additional 76.2 million cases of anxiety disorders worldwide. One community study based on electronic health records reported that long COVID features (defined by International Classification of Diseases 10th Revision codes diagnosis as proxy of each long COVID complaint) frequently co-occurred with anxiety and mood disorders.23 Beyond psychiatric symptoms, the comorbidity of long COVID with psychiatric disorders has to be studied, first because psychiatric disorders are associated with significant impairment in important areas of functioning and a higher suicide risk and second because they can be treated.
To our knowledge, there is only one clinical study24 that systematically assessed long COVID and comorbid psychiatric disorders. It reported an association between the number of long COVID symptoms and post-traumatic stress disorder (PTSD) 1–3 months after severe acute COVID-19. However, this study did not assess other psychiatric disorders and specific criteria of long COVID. Thus, the psychiatric side of long COVID (ie, the association between long COVID and psychiatric disorders) is not documented in terms of frequency and specificity of long COVID complaints and psychiatric disorders. This question is relevant since the diagnosis and treatment of psychiatric disorders could improve the prognosis of long COVID.
In the present study, a multidisciplinary team of clinicians systematically assessed a cohort of 177 patients in terms of somatic complaints and objective measures, psychiatric complaints and psychiatric disorders, as carried out by experienced psychiatrists. We hypothesised that a greater number of long COVID complaints would be associated with higher psychiatric burden. Moreover, we aimed to identify the specific long COVID complaints that would be particularly related to psychiatric burden.
Methods
Design
This was a monocentric cross-sectional study of patients initially hospitalised at the academic Hospital (CHU) of Bicêtre (Paris-Saclay University Hospitals/Assistance Publique-Hôpitaux de Paris (AP-HP)) for an acute COVID-19 during the first wave of the pandemic in France and who agreed to receive a somatic, psychological and psychiatric assessment as outpatients in the 4 months following hospital discharge.
Patient involvement
Patients recruited in the Bicêtre Hospital Multidisciplinary Assessment after COVID-19 (COMEBAC) study and their families were not directly involved in setting the research question or the outcome measures.
Participants and assessment procedure
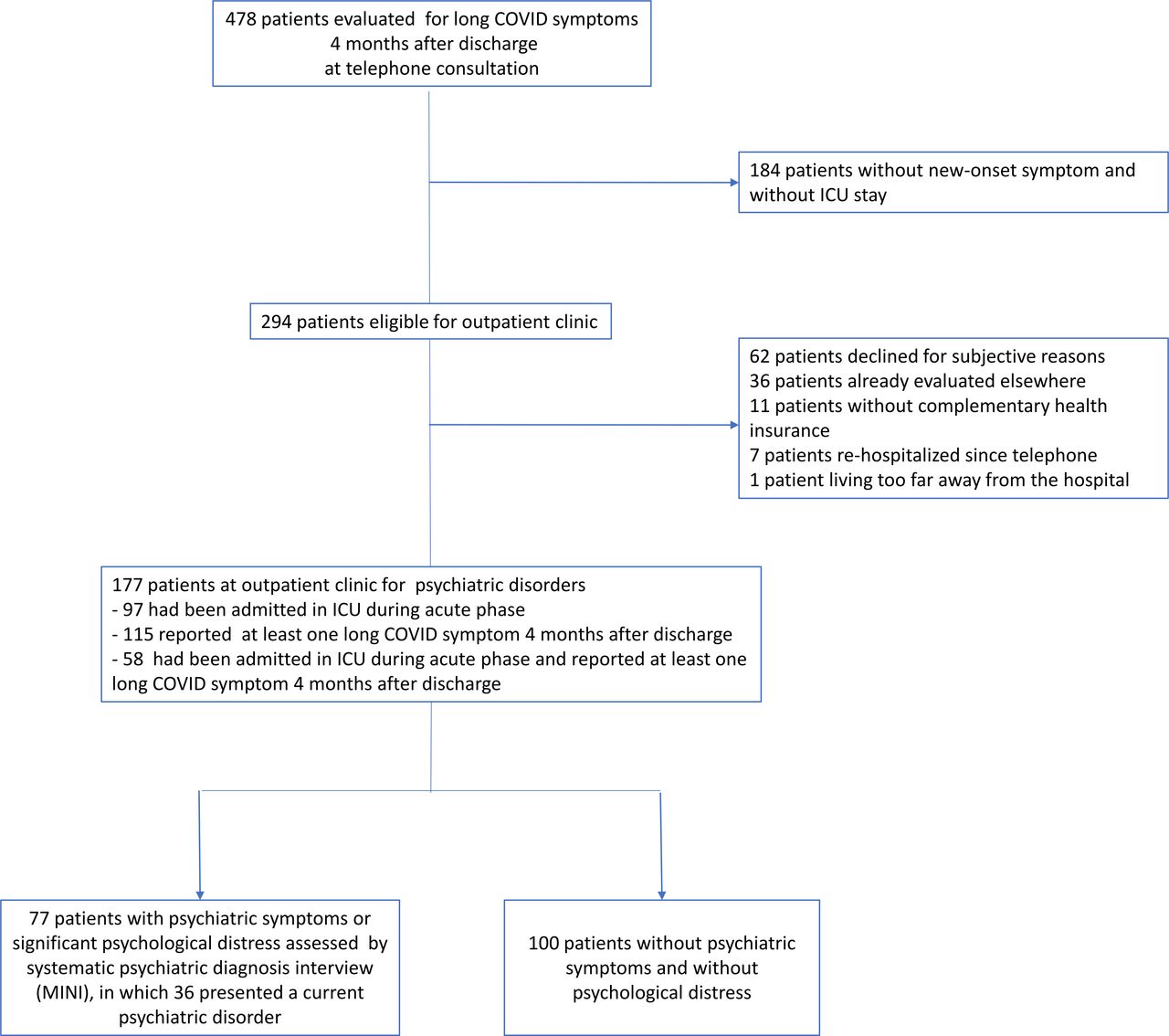
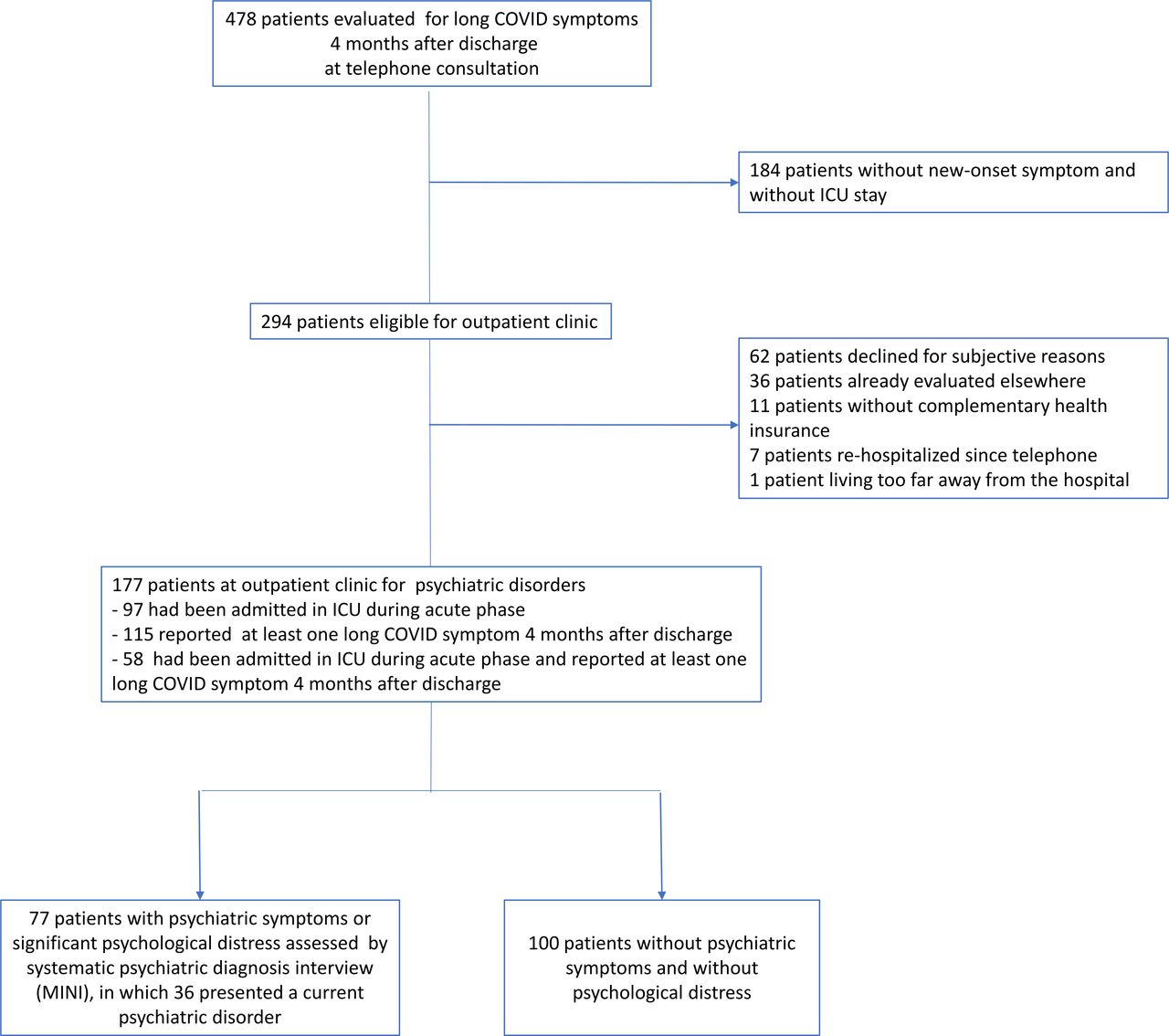
In total, 177 patients were included between 15 July 2020 and 18 September 2020 in the COMEBAC12 outpatient facility. The main inclusion criteria were: age ≥18 years old, hospitalised for >24 hours primarily related to COVID-19, with a SARS-CoV-2 infection admitted in intensive care unit (ICU) during acute phase and/or with at least one long COVID complaint (screened by telephone consultation 4 months after acute COVID-19). The patients benefited from a full multidisciplinary assessment in an outpatient facility. All patients were systematically assessed for their general medical condition, for long COVID complaints and associated objective criteria (ie, CT scan abnormalities and cognitive assessment) and for psychiatric disorders (see psychiatric symptoms and psychiatric disorders, in Methods section). The median length between hospital discharge and day hospital was 125 days (IQR 107–144 days). One hundred seventy-four of the 177 patients (98.3%) had a positive RT-PCR test. Details about the COMEBAC cohort are provided in a flow chart (figure 1).
{kind=link}
Flow chart of the Consultation Multi-Expertise de Bicêtre Après COVID-19 cohort. ICU, intensive care unit; MINI, Mini International Neuropsychiatric Interview.
Baseline characteristics
Sociodemographic information and medical conditions present prior to COVID-19 and potentially associated with long COVID complaints and psychiatric disorders were extracted: age, sex, body mass index (BMI), ICU stay.
Long COVID complaints
To be considered as related to long COVID,5 complaints had to have appeared or worsened since acute COVID-19 infection, and to persist since hospital discharge. We studied first the total number of long COVID complaints, then each complaint separately. Assessed complaints were: fatigue, as declared by the patient; respiratory complaints, that is, subjective feelings of dyspnoea appearing after acute COVID-19; cognitive complaints, comprising memory and self-reported attention difficulties, as well as slowed cognitive processing speed, as reported through the European AIDS Clinical Society screening questionnaire for cognitive complaints25; muscle weakness, that is, difficulty moving, pain (ie, a diffuse pain or myalgia), headache, paraesthesia and anosmia.
Objective criteria associated with long COVID
Since pulmonary sequelae and cognitive impairment are associated with long COVID,6 they were assessed in the study. To detect pulmonary abnormalities, a high-resolution lung CT scan was performed in all patients.12 Cognitive functions were evaluated with the Montreal Cognitive Assessment (MoCA) scale26 to detect objective cognitive impairment (MoCA <26: yes/no).
Psychiatric symptoms and psychiatric disorders
Patients first filled out self-assessment questionnaires focusing on psychiatric symptoms as a screening procedure: the Insomnia Severity Index (ISI)27 for insomnia (cut-off score: 14), the Hospital Anxiety and Depression scale-Anxiety subscale (HAD-A)28 for anxiety symptoms (cut-off score: 7), the Beck Depression Inventory-13 items (BDI)29 for depressive symptoms (cut-off score: 7) and the PTSD Check-List for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 (PCL-5)30 for post-traumatic symptoms (cut-off score: 30). BDI is commonly used to diagnose depression in medically ill patients.31 The cut-off scores were chosen to maximise sensitivity in order to screen psychiatric symptoms.27–30 One hundred seventy of the 177 patients completed the self-assessment questionnaires. Seven patients did not because of difficulties in understanding the questionnaire due to cognitive impairment.
Patients with scores higher than cut-off scores for the ISI, HAD-A, BDI and PCL-5, as well as those identified by psychologists or medical doctors as having significant psychological distress at the time of interview (n=77, 43.5%), were eligible for a systematic interview with a psychiatrist. Patients who were not eligible (ie, who had scores below cut-off scores and who had no psychological distress) were considered as without a current psychiatric disorder (n=100, 56.5%). This diagnostic strategy has been previously validated to detect psychiatric disorders in patients of unknown psychiatric status,32 and structured clinical interview is recommended to diagnose depression in medically ill patients.31 It should be emphasised that the detection thresholds of psychological symptoms were sensitive, since more than half of patients with significant psychological symptoms systematically assessed by psychiatrists were free of psychiatric disorders.
Current psychiatric disorders 4 months after COVID-19 were diagnosed by qualified psychiatrists according to the DSM-5 criteria33 using the Mini International Neuropsychiatric Interview (MINI 5.0).34 The MINI covers the following diagnoses: major depressive episode (lifetime and past 2 weeks), suicidality (past month), manic and hypomanic episodes, bipolar I and II disorders (lifetime and current), panic disorder (lifetime and past month), agoraphobia (lifetime and past month), social anxiety disorder (lifetime and past month), obsessive-compulsive disorder (lifetime and past month), generalised anxiety disorder (lifetime and current), PTSD (lifetime and past month), alcohol and other substance use disorders (lifetime and current), current psychotic disorder, anorexia nervosa (past 3 months), bulimia nervosa (past 3 months) and binge-eating disorder (past 3 months).33 Panic disorder, generalised anxiety disorder, agoraphobia and social anxiety disorder were pooled into a single category: anxiety disorders. The current presence or absence of each psychiatric disorder was reported.
New-onset psychiatric disorders were defined as any psychiatric disorder that appeared during the 4 months following acute COVID-19 in patients with no previous history of psychiatric disorders. History of psychiatric disorders before the COVID-19 acute infection was assessed through psychiatric interviews and extracted from previous medical and psychiatric records.
Because of its clinical relevance, significant suicide risk (yes/no) was also assessed specifically according to item C of the MINI, using the ‘low’ threshold (score <8).34 35 This risk is based on current suicidal thoughts and/or a suicide attempt in the month prior to evaluation.
Statistical analysis
Baseline characteristics, long COVID complaints (total number of complaints and presence/absence of each complaint: fatigue, respiratory complaints, cognitive complaints, muscle weakness, pain, headache, paraesthesia and anosmia), psychometric questionnaire scores (ISI, HAD-A, BDI, PCL-5), diagnoses of psychiatric disorders, new-onset psychiatric disorders and a significant suicide risk 4 months after acute COVID-19 were first described.
First, the association between the number of long COVID complaints and psychiatric symptoms and psychiatric disorders was studied. Correlations between the number of long COVID complaints and the psychiatric symptoms were analysed with Spearman’s correlation tests. The mean number of long COVID complaints was compared between patients with a psychiatric disorder, a new-onset psychiatric disorder or a significant suicide risk, and those without any current or past psychiatric psychiatric disorders using Student’s t-test or Wilcoxon test. Poisson regressions were used to compare the numbers of long COVID complaints between patients with a psychiatric disorder, a new-onset psychiatric disorder or a significant suicide risk, and those without any current or past psychiatric disorders.
Second, the association between individual COVID-19 complaints and psychiatric complaints and psychiatric disorders was studied. Patients with or without each long COVID complaint were compared for baseline characteristics and psychometric questionnaire scores with Student’s t-test or Wilcoxon test for quantitative variables and χ² test or Fisher’s exact test for qualitative variables.
The total number of long COVID complaints, each long COVID complaint and objective long COVID criteria was compared between patients with psychiatric disorders, new-onset psychiatric disorders, significant suicide risk and those without any psychiatric disorders lifetime with Student’s t-test or Wilcoxon test for quantitative variables and χ² test or Fisher’s exact test for qualitative variables. To identify the specific long COVID complaints independently associated with psychiatric disorders, new-onset psychiatric disorders, suicide risk, anxiety disorders and major depressive episodes, five logistic regressions were performed (one for each type of psychiatric disorder as a variable to be explained). For each regression, the explicative variables were the long COVID complaints and variables that were significantly different in bivariate analyses between the control group and each type of psychiatric disorder, with adjustment for age, sex, ICU stay during the acute COVID-19 period (chosen a priori). Statistical analyses were performed using R V.4.0.3.
Results
Patients
The characteristics of the 177 patients are shown in table 1. Among them, 115 (65.0%) patients presented at least one long COVID complaint. Mean number of long COVID complaints was 1.55 (SD 1.54). Fatigue (44.1%), respiratory complaints (43.5%), cognitive complaints (23.7%) and paraesthesia (20.9%) were the most common long COVID complaints. Moreover, 108 patients (61.0%) had lung CT scan abnormalities and 115 (65.0%) had objective cognitive impairment (MoCA score <26). Ninety-seven (54.8%) patients were admitted to the ICU during their hospitalisation.
Long COVID complaints and scores of insomnia, anxiety, depressive and post-traumatic stress
Patients with fatigue were more frequently women (39 (50.0%)) as compared with patients without fatigue (22 (25.3%)). No other baseline or COVID-19 characteristic was associated with long COVID-19 complaint.
Anxiety (in 31.4% of patients), depressive (in 20.6% of patients), post-traumatic (in 14.2% of patients) and insomnia (in 53.6% of patients) symptoms have been described in a previous study.12
One hundred thirty-one (74.0%) patients were free of any psychiatric disorder (past or current). Thirty-six (20.3%) patients had at least one current psychiatric disorder, of which 29 (16.4%) were new-onset psychiatric psychiatric disorders, including 24 (13.6%) major depressive episodes, 20 (11.3%) anxiety disorders and 7 (3.9%) PTSD. Nine (5.1%) patients had a significant suicide risk.
Seven (19.4%) of the 36 patients had a history of psychiatric disorder (major depressive disorder) before the onset of the acute COVID-19 infection. After COVID-19, six of them were diagnosed with a current major depressive episode, and one of them with a PTSD.
Number of long COVID complaints
The number of long COVID complaints was significantly associated with insomnia, anxiety, depressive and post-traumatic stress symptoms (table 1).
The number of long COVID complaints was greater in patients with a psychiatric disorder, in those with a new-onset psychiatric disorder and in those with a significant suicide risk compared with patients without any past or current psychiatric disorder (table 2).
Baseline characteristics and long COVID in patients without any psychiatric disorder lifetime, with at least one current psychiatric disorder, with a new-onset psychiatric disorder and with a significant suicide risk
Poisson regressions adjusted for age, sex, ICU stay showed that the number of long COVID complaints was higher in patients with a psychiatric disorder (estimate=0.45; 95% CI (0.18 to 0.72); p=0.001), a new-onset psychiatric disorder (estimate=0.37; 95% CI (0.07 to 0.66); p=0.01) or a significant suicide risk (estimate=0.51; 95% CI (0.06 to 0.91); p=0.02).
Specific long COVID complaints
The occurrence of fatigue, respiratory and cognitive complaints, headache, paraesthesia and anosmia were all associated with higher scores for at least one psychometric self-measure, whereas muscle weakness and persistent pain were not (table 1).
Respiratory and cognitive complaints and persistent fatigue were more frequent in patients with psychiatric disorders, new-onset psychiatric disorders and significant suicide risk than in patients without any psychiatric disorders lifetime (table 2). No association was observed for the other long COVID complaints.
Multivariable logistic regressions including respiratory and cognitive complaints and persistent fatigue and adjusted for age, sex, ICU stay showed that respiratory complaints were associated with a higher risk of psychiatric disorder (OR=4.30; 95% CI (1.71 to 10.70); p=0.003) and new-onset psychiatric disorder (OR=2.45; 95% CI (1.16 to 7.80); p=0.03). Cognitive complaints were associated with a higher risk of psychiatric disorder (OR=2.63; 95% CI (1.03 to 6.73); p=0.04).
A multivariable logistic regression including respiratory and cognitive complaints, and adjusted for age, sex, ICU stay, showed that cognitive complaints were associated with a significant suicide risk (OR=7.33; 95% CI (1.52 to 44.3); p=0.02) (table 3).
Adjusted OR calculated from logistic regression model with adjustment on age, sex and ICU stay, assessing the association between long COVID complaints and psychiatric disorders
Respiratory complaints (OR=7.8; 95% CI (2.1 to 39.4); p=0.005) and fatigue (OR=6.7; 95% CI (1.8 to 34.9); p=0.01) were more frequent in patients with anxiety disorders independently from other long COVID complaints, whereas cognitive (OR=4.8; 95% CI (1.7 to 14.6); p=0.004) and respiratory complaints (OR=3.5; 95% CI (1.2 to 11.4); p=0.03) were more frequent in patients with a major depressive episode (table 3).
Discussion
This is the first study to examine the association between long COVID and psychiatric disorders diagnosed by qualified psychiatrists. It evidences the psychiatric burden associated with long COVID. We find that long COVID is associated with higher levels of psychiatric symptoms and current psychiatric disorders, new-onset psychiatric disorders and a current significant suicide risk. This is the first study showing this association between disorders diagnosed by psychiatrist.
Our results are in line with previous results showing an association between long COVID symptoms and psychiatric symptoms.15 18 36 Recent findings on electronic health records23 showed a co-occurrence of psychiatric disorders and long COVID symptom but without systematic assessment by psychiatrists.
Suicidal ideation have been reported in patients with COVID-19 during the acute phase.37 Our results show that suicide risk is also observed 4 months after COVID-19.
Specifically, cognitive and respiratory complaints are particularly associated with psychiatric disorders and suicide risk. Patients with respiratory complaints have a fourfold higher risk to have a disorder and a twofold higher risk to have a new-onset psychiatric disorder. Patients with cognitive complaints have a twofold higher risk to experience a psychiatric disorder and a sevenfold higher significant suicide risk. This later result is coherent with those reported in patients without COVID-19.38 Of note, subjective complaints more than objective cognitive deficits assessed with the MoCA therefore appear to be the main issue in long COVID conditions.
The association between long COVID respiratory complaints and psychiatric disorders is in agreement with the scientific literature showing that respiratory complaints present in COVID-19 survivors39 are associated with more psychiatric symptoms.15 18 Interestingly, this association was independent of lung CT scan abnormalities. In line with this finding, a discrepancy between long COVID respiratory complaints and lung CT scan abnormalities has been reported.10 More specifically, we show that respiratory complaints are associated with anxiety disorders, whereas both respiratory and cognitive complaints are associated with major depressive episodes, which could provide a diagnosis cue to clinicians.
We did not find any association between psychiatric disorders and other long COVID complaints, including muscle weakness, headache, paraesthesia, persistent pain or anosmia. It has been suggested that long COVID may comprise different syndromes, each with a specific mechanism.1 Our results suggest that a specific subtype of long COVID comprising respiratory and cognitive complaints may be particularly associated with anxiety and major depressive disorders. Further studies should confirm the identification of this specific subtype of long COVID.
This study has several limitations. First, its sample size is relatively small. Second, these patients were hospitalised for acute COVID-19. It is unclear whether our results can be extended to milder non-hospitalised forms of COVID-19. Further studies should include non-hospitalised patients, who may have different mechanisms underlying the persistence of symptoms. Moreover, the assessment was conducted 4 months postinfection, and the frequency of a persisting psychiatric disorders and the incidence of later ones is unknown. Indeed, recent studies suggest that some long COVID symptoms (but not anxiety and depressive symptoms) may disappear over time.11 Third, since this was an inclusion criterion, a majority of patients has been hospitalised in ICU, and this group may not be representative of all patients hospitalised for an acute COVID-19 infection. Fourth, only some of the long COVID complaints known at the time of the study were investigated (eg, symptoms such as dizziness were not assessed). Fifth, the screening procedure might miss some psychiatric disorders.
The main strength of this study is the clinical characterisation of patients with COVID-19, with relevant somatic and psychiatric assessments following COVID-19. In particular, psychiatric disorders and significant suicide risk have been systematically checked with validated tools and evaluated by psychiatrists. The relevance of a systematic psychiatric assessment in COVID-19 survivors has been highlighted.40 The comorbidity of long COVID with psychiatric disorders has to be taken into account first because they increase suicide risk and imply significant impairment, second because an adequate treatment of psychiatric disorders could improve long COVID outcome.
Conclusion
Long COVID complaints are associated with psychiatric disorders, new-onset psychiatric disorders, significant suicide risk and psychiatric symptoms. In patients with long COVID, especially those with respiratory or cognitive complaints, psychiatric disorders and suicide risk should be systematically assessed.
Data availability statement
Data may be obtained from a third party and are not publicly available. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
The Ethics Committee of the French Intensive Care Society (CE20-56) approved the study. All patients provided written informed consent to this study.
Acknowledgments
We thank the patients who participated in this cohort, as well as the physicians, psychologists, nurses, caregivers, biologists, pharmacists, other allied health professionals and administrators of Bicêtre Hospital and the Assistance Publique-Hôpitaux de Paris.
References
Footnotes
Twitter @m_gasnier, @Montanidavid, @MOODS_Inserm
Collaborators The COMEBAC study group: Luc Morin, MD, MSc; Laurent Savale, MD, PhD; Tài Pham, MD, PhD; Romain Colle, MD, PhD; Samy Figueiredo, MD, PhD; Anatole Harrois, MD, PhD; Matthieu Gasnier, MD; Anne-Lise Lecoq, MD, PhD; Olivier Meyrignac, MD, PhD; Nicolas Noel, MD, PhD; Elodie Baudry, MD; Marie-France Bellin, MD; Antoine Beurnier, MD; Walid Choucha, MD; Emmanuelle Corruble, MD, PhD; Laurent Dortet, PharmD, PhD; Isabelle Hardy-Leger, MA; François Radiguer, MA; Sabine Sportouch, MA; Christiane Verny, MD; Benjamin Wyplosz, MD, PhD; Mohamad Zaidan, MD, PhD; Laurent Becquemont, MD, PhD; David Montani, MD, PhD; Xavier Monnet, MD, PhD.
Contributors MG, EC, RC: conception of the study; the design of the study, collection of the data, statistical analysis, interpretation of the results, drafting of the manuscript and editing. FJ: interpretation of the results, editing and approval of the final version of the manuscript. KC: interpretation of the results, language editing and approval of the final version of the manuscript. WC, FR, AB, TF, CK, PT, MD, AEKTB, HH, IH-L, OM, LM, A-LL, TP, NN, DM, XM, LB participated in the collection of the data, and editing. All authors: approval of the final version of the manuscript. EC and RC are the guarantors of this work. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This study was funded by the Assistance Publique—Hôpitaux de Paris.
Disclaimer The funder was not involved in the design and conduct of the study, collection, management, analysis and interpretation of the data, preparation, review or approval of the manuscript, nor the decision to submit the manuscript for publication.
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work. NN reported personal fees from MSD and Biogen outside the submitted work. DM reported personal fees from Actelion, GSK, Pfizer, MSD, Chiesi, Boehringer and Incyte Biosciences France, grants from Bayer and MSD and non-financial support from Acceleron outside the submitted work. XM reported personal fees from Getinge Pulsion Medical and Baxter outside the submitted work. No other disclosures were reported. LB reported grants from Sanofi Genzyme for a presentation concerning Gaucher disease, and pharmacogenetics and drug interactions with Eliglustat outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.