Article Text

Abstract
Objective Neuropsychiatric (NP) symptoms are prominent features of cognitive decline, but they have been understudied in patients with spontaneous intracerebral haemorrhage (ICH). In ICH survivors, we aimed at assessing NP symptoms prevalence and profiles, and their influence on long-term outcomes.
Methods We analysed data from consecutive 6-month ICH survivors enrolled in the Prognosis of Intracerebral Haemorrhage study. We performed NP evaluation using the Neuropsychiatric Inventory Questionnaire. Patients underwent long-term clinical follow-up after ICH (median follow-up time 7.2 years, IQR 4.8–8.2).
Results Out of 560 patients with ICH, 265 survived at 6 months. NP evaluation 6 months after ICH was feasible in 202 patients. NP symptoms were present in 112 patients (55%), and in 36 out of 48 patients (75%) with post-ICH dementia. Affective symptoms were present in 77 patients (38%), followed by vegetative symptoms (52 patients, 26%) and hyperactivity (47 patients, 23%). Apathy and hyperactivity were associated with post-ICH dementia and cerebral amyloid angiopathy MRI profile (all p<0.05). Apathy and hyperactivity prevailing over affective symptoms at 6-month follow-up were associated with higher risks of developing new-onset dementia (HR 5.40; 95% CI 2.27 to 12.84), while presence or severity of NP symptoms were not.
Conclusion NP symptoms were present in more than half of 6-month ICH survivors, with higher prevalence and severity in patients with post-ICH dementia. Distinctive NP profile might be associated to cognitive status and inform on long-term dementia risk.
- dementia
- amyloid
- cerebrovascular
- MRI
- stroke
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Introduction
Neuropsychiatric (NP) symptoms are prominent features of neurodegenerative diseases and cognitive decline, and are highly prevalent at all stages of dementia irrespective of presumed causes.1–3 NP symptoms seem also to predict the development of cognitive impairment in cognitively normal elderly, as well as the transition from mild cognitive impairment to dementia.4 5
Intracerebral haemorrhage (ICH) is associated with poor long-term outcomes, especially mortality, disability and cognitive decline.6–8 ICH survivors are potentially at high risk of developing NP symptoms, but NP screening has rarely been investigated in this population. A recent study on patients with all types of stroke found higher rates of behavioural disturbances in a small ICH subgroup.9 The over-representation of NP disturbances in patients with ICH might be related to the higher prevalence of dementia and cerebral amyloid angiopathy (CAA) in this population.6 10
In patients with dementia, the presence of NP symptoms is associated with worse functional status and quality of life in both patients and caregivers.11 The identification of NP symptoms could influence planning of care and preventive strategies to reduce the burden of cognitive and functional status in ICH survivors. Finally, NP screening might improve the early identification of patients at higher risk for long-term cognitive decline after ICH. However, to date determinants and clinical implications related to NP symptoms have been poorly evaluated in ICH.
In a large cohort of consecutive ICH survivors, we aimed to determine the prevalence and the predictors of NP symptoms 6 months after ICH. We hypothesised that NP symptoms profiles would differ according to the cognitive status, the location of ICH, and the underlying small-vessel disease (SVD) type (CAA vs non-CAA). We also evaluated the influence of NP symptoms on the long-term mortality and dementia risks.
Methods
Patient selection
We analysed data from consecutive patients with spontaneous ICH enrolled in the ‘Prognosis of Intra-Cerebral Haemorrhage’ (PITCH) cohort12 from November 2004 to March 2009, alive at 6 months, who could undergo NP assessment. Inclusion and exclusion criteria for the enrolment in the prospective PITCH cohort have been extensively described in previous studies.6 13
Baseline clinical evaluations
Baseline demographic characteristics, vascular risk factors, history of stroke (ischaemic or haemorrhagic) were collected, as previously detailed.6 13 History of pre-existing dementia was defined as a score ≥64 using the short version of Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE)—French adaptation.6 14 We used the modified Rankin Scale to assess functional status before ICH, and the National Institute of Health Stroke Scale (NIHSS) score to assess ICH severity.
Follow-up evaluation
As part of our standard in-house protocol for post-stroke care, patients were invited to be followed up at 6 months and 1, 2, 3, 4.5, 6, 8 and 10 years after the index ICH, as previously detailed.6 8 During the follow-up visits, we recorded the occurrence of dementia, and use of antidepressant, hypnotic and anxiolytic drugs. The diagnosis of dementia was made according to the National Institute on Aging-Alzheimer’s Association criteria for all-cause dementia.15 The term post-ICH dementia refers to the presence of dementia at the moment of NP evaluation 6 months after ICH. When patients were not able to come to the hospital for the follow-up visit, we contacted them, their relatives or family physician to ascertain whether the patient was alive or not.
NP evaluation
The NP evaluation was conducted by a neurologist 6 months after ICH using the Neuropsychiatric Inventory Questionnaire (NPI-Q), a tool that allows a quick evaluation of NP symptoms through an informant-based, self-administered battery.16 NPI-Q is a brief version of the Neuropsychiatric Inventory (NPI) originally designed by Cummings et al.17 NPI-Q encompasses 12 items: hallucinations, delusions, agitation/aggression, depression, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, aberrant motor behaviour, night-time behaviour, appetite/eating change. For each item, the informant was asked if the principal symptoms were absent or present; if present, severity (range 1–3) was recorded for each item. A global NPI-Q severity score (maximum score 36) was calculated. For the purpose of the study, we categorised NP symptoms into five domains: hyperactivity (agitation/aggression, disinhibition, irritability/lability), affect (depression, anxiety), psychosis (hallucinations, delusions), apathy and vegetative (night-time behaviour, appetite/eating change).18 A severity sum score was calculated for each domain.
Imaging
CT scan was performed at admission for all patients in the study. ICH location was dichotomised into lobar and non-lobar, the latter encompassing also brainstem and cerebellar haemorrhages.7 ICH volume was calculated according to ABC/2 method.19 A 1.5 Tesla brain MRI was performed in all patients without contraindications a few days after the index ICH. The MRI protocol included at least fluid attenuated inversion recovery and T2*-weighted gradient-echo sequences (echo time: 228 ms, repetition time: 700 ms, flip angle: 25°, field of view: 250 mm, matrix: 352 224, slice thickness: 5 mm and interslice gap: 1.5 mm).6–8 Presence of lacunes and cortical superficial siderosis (cSS), presence and location (strictly lobar, strictly deep, mixed) of cerebral microbleeds (CMB), white matter hyperintensities (WMH) severity (Fazekas scale)20 and degree of cerebral atrophy were assessed as previously reported.6 7 21
Based on the location of ICH and CMB, we categorised patients into two groups: (1) CAA MRI profile, when the ICH was limited to lobar locations and was associated or not with (a) strictly lobar CMB (deep ICH and CMB not allowed), (b) cSS10 22; (2) non-CAA MRI profile in all the remaining cases.
Statistical analyses
We assessed normality of distribution for all quantitative measures using Shapiro-Wilk W test. To determine whether patients with NP evaluation were representative of the whole ICH survivors’ cohort, we compared their main baseline characteristics using the χ2 test for categorical variables and the Mann-Whitney U test for continuous variables. We performed the same analyses for patients who were not fit enough to undergo brain MRI.
We used the χ2 and Mann-Whitney U tests to evaluate univariate associations between NP symptoms presence and demographic, clinical and imaging variables. We performed multivariable analysis for the presence of NP symptoms (ie, the presence of at least one NP symptom) using a binary logistic regression model. In patients with NP symptoms, we used an ordinal logistic regression model to evaluate associations between NP symptoms severity and demographic, clinical and imaging variables. To perform ordinal logistical regression analysis, we divided the global NP symptoms severity score distribution in tertiles (1st: score 1–2; 2nd: score 3–6; 3rd: score ≥7). In multivariable models, we adjusted for age, sex and baseline factors with a p value <0.1 in univariate analysis.
Among patients with NP symptoms, we evaluated differences in NP profiles in pre-specified subgroups: (1) demented versus non-demented; (2) lobar versus non-lobar ICH; (3) CAA versus non-CAA MRI profile. We calculated the ORs for prevalence of each NP symptom domain in the prespecified subgroups.
We performed survival analysis to evaluate the influence of NP symptoms, their severity, and profiles on mortality and long-term new-onset dementia risks. We performed multivariable analyses using Cox proportional hazard regression model for age-adjusted long-term mortality and age-adjusted long-term new-onset dementia risk. We further adjusted for presence of post-ICH dementia in survival analyses on long-term mortality. In survival analyses, we censored those lost to follow-up at the last available follow-up.
Before developing multivariable model, the collinearity was appreciated using a variance inflation risk with an alert threshold value of 2.5. We used a p value threshold of 0.05 to ascertain statistical significance for all analyses. We performed all statistical analyses using the SPSS software (V.22; IBM).
Results
Subjects
Out of the 560 patients with spontaneous ICH included in the PITCH cohort, 265 (47.3%) were alive 6 months later (figure 1). We could not perform the NPI-Q evaluation in 63 patients (23.8%), mainly for the absence of a reliable informant and in case of severely impaired/aphasic patients in which the identification of NP symptoms is difficult. ICH survivors without NPI-Q evaluation were overall similar compared with those included in the study except for higher cerebral atrophy scores (p=0.041).

Flow diagram of patient selection. ICH, intracerebral haemorrhage; NP, neuropsychiatric. This is an original image and has not been reused or adapted from another source.
The study population consisted of 202 patients (mean age 65 years, SD 14.3; 115 males, 57%; 72 lobar ICH, 36%). The median delay between ICH onset and NP evaluation was 189 days (IQR 174–209). The median long-term follow-up time was 7.2 years (IQR 4.8–8.2). Forty-eight patients (24%) had post-ICH dementia (table 1). One hundred and sixty-seven patients (83%) were fit enough to undergo brain MRI during the hospital stay. Compared with patients with MRI, patients without were more likely to be demented and to be excessive alcohol consumers (both p<0.05). Thirty-four out of 167 patients (20%) had a CAA MRI profile.
Patient characteristics
Prevalence of NP symptoms after ICH
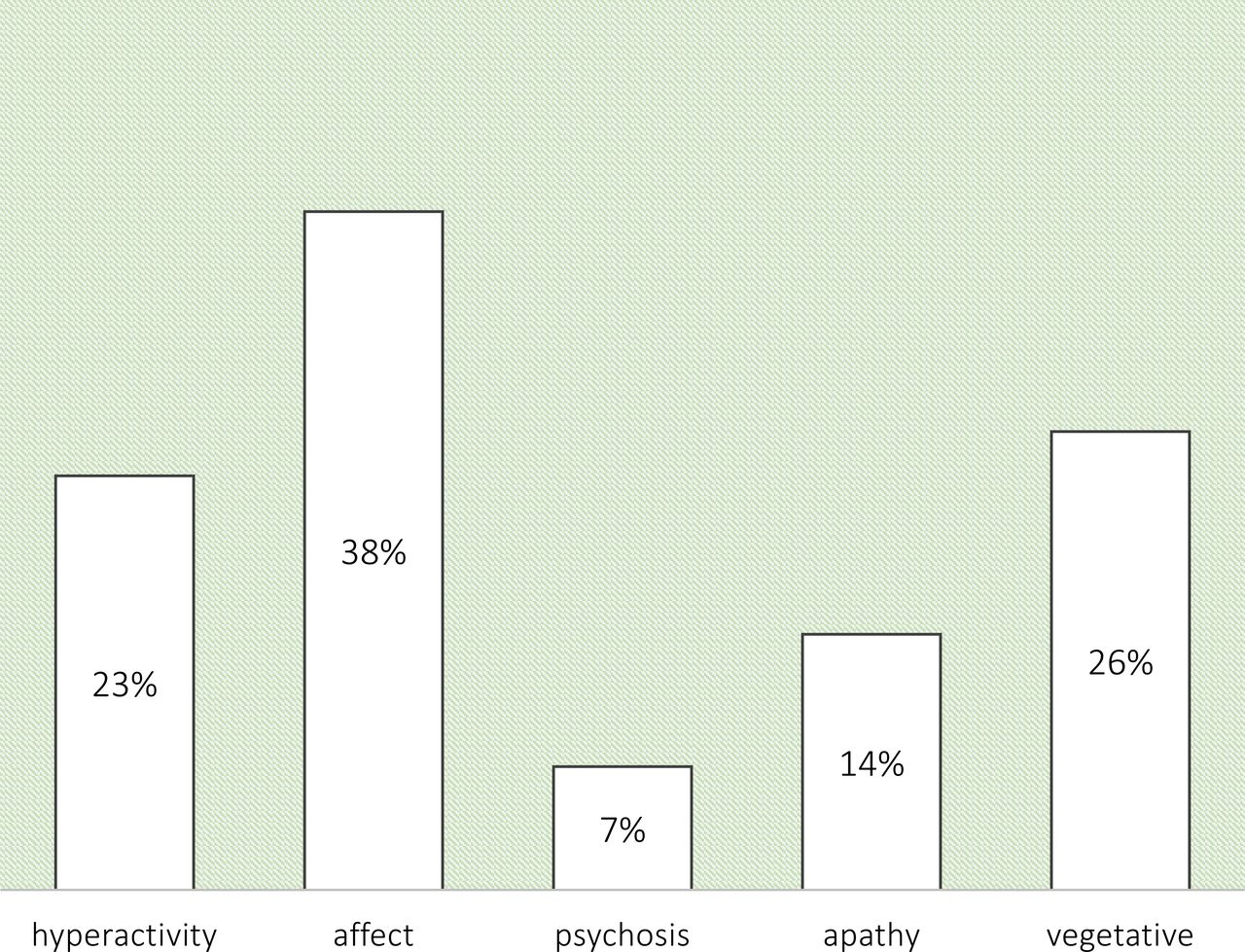
One hundred and twelve patients (55%) had at least one NP symptom 6 months after ICH. The NP symptoms prevalence was higher in patients with post-ICH dementia than in those without (75% and 49%, respectively; p=0.002). Affective symptoms were the most frequent feature, followed by vegetative symptoms, hyperactivity, apathy and psychosis (see figure 2). In univariate and multivariable analyses, among baseline characteristics, NIHSS score at admission was the only variable associated with NP symptoms presence (OR 1.06 for each point increase, 95% CI 1.01 to 1.11, adjusted for age, sex, pre-existing dementia, strictly deep CMB). ICH location and CAA MRI profile were not significantly associated with presence of NP symptoms.

Neuropsychiatric (NP) symptoms 6 months after intracerebral haemorrhage. NP symptoms were clustered into five groups: ‘hyperactivity’ (agitation/aggression, disinhibition, irritability/lability), ‘affect’ (depression, anxiety), ‘psychosis’ (hallucinations, delusions), ‘apathy’ and ‘vegetative’ (night-time behaviour, appetite/eating change). This is an original image and has not been reused or adapted from another source.
NPI-Q severity score in patients with NP symptoms
Among subjects with at least one NP symptom, the median global NPI-Q severity score was 4 (IQR 2–7). The symptoms were more severe among patients with post-ICH dementia (median global NPI-Q severity score 6.5 vs 3; p<0.001), and in patients using anxiolytic/hypnotic drugs during follow-up (p<0.001). In univariate analysis, among baseline clinical and imaging characteristics, previous stroke, pre-ICH functional disability and CAA MRI profile were associated with higher global NP symptoms severity scores (all p<0.05). In multivariable model, CAA MRI profile and pre-ICH functional disability were independently associated with higher global NP symptoms severity scores (table 2).
Multivariable ordinal regression model for neuropsychiatric symptoms severity
NP profile
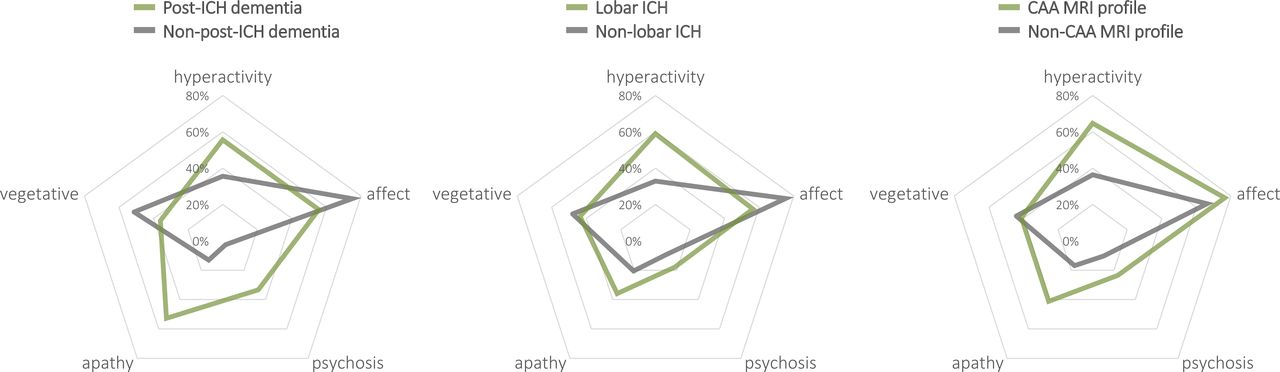
In figure 3, we described NP profile of patients with NP symptoms in different prespecified subgroups. In the subgroup of patients with post-ICH dementia compared with those without, we found a significant higher rate of hyperactivity symptoms (OR 2.27, 95% CI 1.01 to 5.09), apathy (OR 7.38, 95% CI 2.90 to 18.75) and psychosis (OR 18.50, 95% CI 3.86 to 88.58), with a lower rate of affective symptoms (OR 0.42, 95% CI 0.18 to 0.96). Compared with patients with non-lobar ICH, those with lobar ICH were more likely to have hyperactivity symptoms (OR 2.94, 95% CI 1.31 to 6.55) and less likely to have affective symptoms (OR 0.42, 95% CI 0.18 to 0.97). Patients with a CAA MRI profile were more likely to have hyperactivity symptoms (OR 3.21, 95% CI 1.07 to 9.62) and apathy (OR 3.45, 95% CI 1.11 to 10.72) compared with those without.
{kind=link}
{kind=link}
{kind=link}
Neuropsychiatric (NP) profiles according to intracerebral haemorrhage (ICH) subtype and cognitive status. Values in radar charts represent the observed prevalence of each Neuropsychiatric Inventory Questionnaire domain among patients with at least one NP symptom. CAA, cerebral amyloid angiopathy. This is an original image and has not been re-used or adapted from another source.
NP symptoms and long-term outcome
During a median follow-up time of 7.2 years (IQR 3.8–10.6), 88 patients (44%) died. The case-fatality rate was higher in patients with NP symptoms vs without (51% vs 34%; p=0.019). Presence and severity of NP symptoms were significantly associated with long-term mortality in Cox proportional hazard regression analyses adjusted for age: HR for presence of NP symptoms was 1.57 (95% CI 1.00 to 2.45); HR for each level increase in NPI-Q severity score was 1.05 (95% CI 1.00 to 1.11). However, these significant associations were not confirmed after further adjustment for post-ICH dementia.
During the long-term follow-up, in patients without dementia at the time of NP evaluation 6 months after ICH (n=154), 26 developed long-term new-onset dementia over a median delay of 3.1 years (IQR 2.0–6.0). There was no association between presence and severity of NP symptoms and the risk of long-term new-onset dementia. Based on the higher frequency of apathy and hyperactivity symptoms in patients with post-ICH dementia compared with those without, we categorised included patients with ICH into two groups: (1) patients with NPI-Q severity score higher in hyperactivity plus apathy subscores compared with affect subscore; (2) all the remaining patients. Prevailing apathy and hyperactivity symptoms were associated with long-term new-onset dementia in Cox proportional hazard regression analyses adjusted for age (HR 5.40; 95% CI 2.27 to 12.84; p<0.001). This NP profile was not associated with mortality in survival analyses.
Discussion
We found that NP symptoms are observed in more than half of 6-month ICH survivors. Patients with post-ICH dementia had a three-times higher risk to present concomitant NP symptoms. Affective symptoms were the most prevalent disturbances, followed by vegetative and hyperactivity symptoms. Greater ICH severity at onset was associated with presence of NP symptoms after ICH. Severity of NP symptoms was independently associated with CAA MRI profile and pre-ICH disability. Hyperactivity and apathy were more frequent among patients with post-ICH dementia, while affective symptoms were more frequent in patients without post-ICH dementia. In survival analyses, presence and severity of NP symptoms were not independently associated with an increased long-term mortality and dementia. Differently, a specific NP profile (prevailing apathy and hyperactivity over affective symptoms) was associated with an increased risk of developing long-term new-onset dementia. Overall, this study is the first attempt to investigate NP symptoms specifically in patients with ICH. In this context, a timely recognition of NP symptoms could improve care planning and have a clinically meaningful effect for long-term ICH management.
The most frequently observed NP symptoms were affective disturbances. This result is in line with studies focusing on anxiety and depression that have been consistently reported as frequent manifestations after stroke.23 24 However, we found that other NP disturbances (ie, vegetative symptoms, hyperactivity) are also relatively frequent in the ICH population.
NP symptoms were more severe in patients with post-ICH dementia and in those showing a CAA MRI profile. In Alzheimer-type and vascular cognitive impairment NP symptoms are highly prevalent suggesting a contribution of cortical beta-amyloid load.1 25 26 Our results suggest that vascular amyloid deposition may influence NP manifestations in patients with ICH. Unfortunately, to date, no study using amyloid positron emission tomography, nor neuropathology, can confirm this hypothesis. In our cohort, individual SVD markers such as WMH, lacunes, cerebral atrophy and cSS were neither associated with NP symptoms presence nor severity. This might be related to a lack of power, or to a lower specificity of markers such as WMH, lacunes, cerebral atrophy for underlying CAA. As highlighted in a recent systematic review focusing on patients with SVD,27 further studies are needed and cohorts should also include large numbers of patients with ICH.
Our results suggest that NP profiles vary according to cognitive status, ICH location and predominant SVD subtype (CAA vs non-CAA). In fact, patients with post-ICH dementia, lobar ICH location, and CAA MRI profile share an overall similar NP profile. Apathy and hyperactivity were more frequent in patients with post-ICH dementia, while affective symptoms were more frequent in patients without post-ICH dementia. The lower rate of affective symptoms observed in patients with post-ICH dementia might partially be related to a relative lack of insight of depressive and anxious symptoms in severely cognitively impaired individuals and their informant.28 29 However, we cannot exclude a potential inaccuracy of brief screening tools in assessing affective symptoms in demented patients.30 Furthermore, several studies have reported high rate of depression and anxiety in the whole stroke population, also in the absence of cognitive impairment.23 24 Finally, we can speculate that the overall similarity between NP profiles of patients with post-ICH dementia, lobar ICH and CAA-MRI profile is related to the parenchymal damage due to the cumulative burden of lesions attributable to CAA.26 31
We also evaluated the association between NP symptoms and long-term outcomes, in terms of mortality and new-onset dementia risk. Presence and severity of NP symptoms were associated with long-term mortality in age-adjusted survival analyses, although this finding could be driven by the presence of coexisting dementia, since these associations were not confirmed after adjustment for post-ICH dementia. Differently, presence and severity of NP symptoms were not associated with long-term new-onset dementia. However, we identified a distinctive NP profile (apathy and hyperactivity prevailing over affective symptoms) associated with the development of new-onset dementia in long-term follow-up. Similarly, a recent study on patients with cerebral SVD showed that apathy, but not depression, predicted development of new-onset dementia.32 Therefore, it appears that, more than the presence/severity of NP symptoms, is the NP profile to be associated with cognitive decline. The lack of association between NP symptoms presence and new-onset dementia is in part related to the design of NPI-Q. This validated screening tool provide a comprehensive overview of NP symptoms. In fact, NPI-Q evaluates different and heterogeneous NP manifestations in terms of clinical significance and risk prediction.33 Of note, the median time of the diagnosis of new-onset dementia was 3 years, and a non-negligeable 25% of them were made 6 years after ICH: this finding underlines the importance of long-term follow-up of ICH survivors.
Our study has several limitations. This is a retrospective analysis of prospectively collected data from a single-centre cohort potentially hampering the generalisability of our results; but the characteristics of the PITCH cohort are similar to those of a population-based ICH study of the same country suggesting that recruitment bias was minimised.13 Notably, our results confirm the high mortality rates associated with spontaneous ICH and the study population consists only of the group of patients that survived the acute phase of ICH. Nevertheless, this group of patients is at high risk of significant clinical event after the index ICH.6 7 In this perspective, our study showed that NP symptoms are also common in long-term ICH survivors. Furthermore, the presence of a specific pattern of NP symptoms may increase the risk of developing dementia during follow-up. We recognise that the exclusion of the minority of 6-month survivors who did not underwent NP evaluation may have constituted a bias in the interpretation of results. However, patients without NP evaluation were similar to those included in the study, except for higher global atrophy score; thus, we think that the risk of bias should be minimal. NPI-Q is a screening tool rather than a comprehensive NP battery preventing to formulate precise clinical diagnosis. However, NPI-Q is an informative tool to identify those patients that could benefit from a more accurate NP evaluation.16 We acknowledge that the exclusion of the minority of patients without brain MRI from some analyses might have constituted a possible bias in interpreting data on cerebral small vessel disease pathology; however, we think this risk is minimised since (1) only a minority of analyses in the study required MRI data, and (2) we were able to demonstrate an effect of CAA MRI profile on NP symptoms despite the risk of underestimation related to the higher prevalence of dementia among patients without brain MRI. Finally, due to the relatively small number of events, our NP symptoms-based prognostic model should be interpreted with caution. Nevertheless, our study prospectively collected long-term outcome data (median follow-up time of 7 years) on many 6-month ICH survivors, but further studies are needed to validate our findings.
NP symptoms are frequently observed in ICH survivors, often in association with post-ICH dementia. Affective symptoms were the most prevalent disturbances. Among patients with NP symptoms, severity was higher in patients with post-ICH dementia and CAA MRI-profile. NP profile varies according to cognitive status, ICH location and predominant SVD subtype (CAA vs non-CAA). Finally, presence and severity of NP symptoms are associated with an increased risk of mortality after ICH (though this association is likely mediated by coexisting dementia), but only a distinctive NP profile seems to inform on long-term dementia risk.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was considered observational by the Internal Review Board of the Lille University Hospital that gave ethics approval for this study. Patients (or their relatives, or primary caregiver) gave informed consent for the study.
Acknowledgments
CC is a member of the Institut Universitaire de France.
References
Footnotes
Twitter @skopelliti, @gboulouis, @leysdidier1, @prccordonnier, @marco_pasi85
Contributors GS designed and conceptualised the study, analysed, and interpreted all data, and drafted the manuscript. MP designed and conceptualised the study, analysed, and interpreted all data, drafted and reviewed the manuscript. HH, DL and CC designed and conceptualised the study, interpreted data and reviewed the manuscript. BC and SM contributed to data collection and revised the manuscript. GB and GK contributed to data collection, analysed imaging data and revised the manuscript. MP was the guarantor for this study.
Funding Inserm U1172 and Adrinord. No award/grant number.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.