Article Text

Abstract
Antithrombotic therapy is a key element of secondary prevention in patients who have had an ischaemic stroke or transient ischaemic attack. However, its use in clinical practice is not always straightforward. This review provides an update on certain difficult scenarios in antithrombotic management, with a focus on recent clinical trials and large observational studies. We discuss the approach to patients with an indication for antithrombotic treatment who also have clinical or radiological evidence of previous intracranial bleeding, patients with indications for both anticoagulant and antiplatelet treatment, and patients in whom antithrombotic treatment fails to prevent stroke. We also review the timing of anticoagulation initiation after cardioembolic stroke, and the use of antithrombotics in patients with asymptomatic cerebrovascular disease. Despite a wealth of new evidence, numerous uncertainties remain and we highlight ongoing trials addressing these.
- cerebrovascular disease
- stroke
- clinical neurology
Statistics from Altmetric.com
Introduction
Antithrombotic therapy remains the cornerstone of secondary prevention after ischaemic stroke or transient ischaemic attack (TIA). Antiplatelet or anticoagulant drugs are prescribed for most patients with ischaemic stroke and are indicated in a substantial proportion of those with intracerebral haemorrhage (ICH). These drugs are associated with a small yet unpredictable increase in bleeding risk (of which intracranial bleeding is the most lethal or disabling) but in many cases the benefits will outweigh the risks. However, stroke is not a homogeneous disease, and an important part of clinical practice is recognising when a deviation from routine antithrombotic therapy is necessary, perhaps due to safety concerns in patients at high risk of bleeding, or to balance competing indications for treatment in patients with vascular comorbidities. Despite a large body of evidence, practical dilemmas in how best to use antithrombotic treatment remain common, including when to start anticoagulants after stroke, and what to do when antithrombotics fail to prevent stroke. Whether antithrombotic treatment might benefit those with incidental cerebrovascular disease, an increasingly common scenario given the frequent use of brain CT and MRI, is also unknown. In this review, we discuss each of these areas in turn, summarising the available evidence, highlighting ongoing studies and priorities for further research, and giving recommendations for management where possible.
Antithrombotic medication in patients with ICH
At least one-third of patients presenting with ICH use antithrombotic medication: antiplatelets in 15%–40% and oral anticoagulants (OAC) in 15%–25% (mainly because of atrial fibrillation (AF)).1–5 Case fatality after ICH is approximately 40% at 1 month,6 and even higher in patients on antithrombotic treatment.2 7 8 In those who survive, clinicians face the dilemma if, in whom, and when antithrombotic medication should be reinitiated. As antithrombotic treatment is frequent in the elderly and the population continues to age, the absolute number of patients with ICH while on antithrombotic treatment is likely to increase with time. Although the adoption of non-vitamin K OACs (NOACs) for prevention of thromboembolism in patients with AF might reduce the incidence of OAC-associated ICH,9 the increased uptake of OAC in the elderly is likely to balance this effect.4 10 Current guidelines provide only weak recommendations on antithrombotic medication after ICH.11 12 Many clinicians have been reluctant to reinitiate antithrombotic treatment, in particular OACs, after ICH, especially in older patients, frail patients at risk of falling, and patients suspected to have cerebral amyloid angiopathy (CAA).13 14 In an observational cohort study describing patients from four different countries, the percentage of patients who restarted antithrombotic drugs after ICH varied between 11% and 45%.13 However, increasing awareness that in patients with ICH the long-term risk of ischaemic stroke and other thromboembolic events may be at least as high as the risk of ICH,15 and even higher in those with non-lobar ICH16 or AF,17 18 is starting to shift secondary prevention paradigms.
Current evidence
Acutely, patients with ICH are often immobile and at risk of deep venous thrombosis and pulmonary embolism. The optimal time to initiate prophylactic low-molecular-weight heparin (LMWH) is uncertain. A Cochrane review identified two small randomised controlled trials (RCTs) and found no differences between treatment groups in the occurrence of deep venous thrombosis (relative risk (RR) 0.99, 95% CI 0.49 to 1.96; n=121) or pulmonary embolism (RR 0.54, 95% CI 0.23 to 1.28; n=121) between those that started LMWH after 2 days or heparin from day four and controls (all patients also received graduated compression stockings).19 Observational data suggest that LMWH started within 48 hours after ICH is probably safe as it did not result in haematoma expansion compared with patients who did not receive this treatment or received it later.12 However, practice varies, with some clinicians choosing to defer LWMH initiation for several days, often with the use of intermittent pneumatic compression in the interim.20
The RESTART trial suggests that antiplatelet therapy after ICH is safe. In 536 participants with ICH while on antithrombotic medication, over a median follow-up duration of 3.0 years, the 268 patients allocated to antiplatelet therapy had a similar risk of recurrent ICH (22 participants, 8.2%) as the 268 allocated to avoid antiplatelet therapy (25 participants, 9.3%, adjusted HR (aHR) 0.87, 95% CI 0.49 to 1.55).21 The risks of major vascular events were also similar in both groups (HR 0.79, 95% CI 0.58 to 1.08). The median time between onset and randomisation was 76 days (IQR 29–146). The absolute risk of major occlusive events was about 1.5 to 2 times higher than the risk of major haemorrhagic events.
The Start or Stop Anticoagulants Randomised Trial (SoSTART) randomised 203 participants with previous spontaneous intracranial haemorrhage (92% intracerebral, 84% OAC-associated) to start or avoid OAC.22 The median time from onset to randomisation was 115 days (IQR 49–265), and nearly all participants starting anticoagulation received an NOAC. Participants were followed up for a median of 1.2 years (251 person-years of follow-up). Participants allocated to start OAC had more intracranial haemorrhage recurrences (8 of 100, 8.0%) than those allocated to avoid OAC (4 of 102, 3.9%), but the prespecified margin for declaring non-inferiority was not met. For the three prespecified composite secondary outcomes (any symptomatic major vascular event, any stroke, or any stroke or vascular death), the aHRs ranged between 0.51 and 0.55, suggesting that starting OAC might be superior to avoiding OAC, but none of the analyses reached statistical significance. The APACHE-AF (Apixaban After Anticoagulation-associated Intracerebral Haemorrhage in Patients with Atrial Fibrillation) trial randomised 101 participants with ICH in the previous 90 days to apixaban or no anticoagulation, a median of 46 days (IQR 21–74) after onset, and followed participants for a median of 1.9 years (222 person-years of follow-up).23 The primary outcome of stroke or vascular death occurred in 13 (26%) of 50 participants allocated to apixaban and in 12 (24%) of 51 allocated to avoid anticoagulation (aHR 1.05, 95% CI 0.48 to 2.31). More participants allocated to apixaban than allocated to avoid anticoagulation had a recurrent ICH (aHR 4.08, 95% CI 0.45 to 39.91), but there was no difference between the treatment groups in the rate of ischaemic stroke (aHR 0.96, 95% CI 0.31 to 2.97). Before the results of these trials, observational studies had suggested that survivors of intracranial haemorrhage recommencing OAC had a lower risk of ischaemic stroke (RR 0.46, 95% CI 0.29 to 0.72), whereas the risk of recurrent ICH was comparable (RR 1.23, 95% CI 0.80 to 1.87) to those who did not,24 and that OAC resumption was associated with a decreased risk of death and of ischaemic stroke and comparable risk of ICH recurrence, both in non-lobar and in lobar haemorrhage.25 OAC resumption was associated with decreased risk of death (aHR 0.27, 95% CI 0.08 to 0.86 for possible CAA (n=136); aHR 0.30, 95% CI 0.10 to 0.92 for probable CAA (n=54)).26 The results of these observational studies could have been confounded by indication, and most patients on anticoagulation were treated with vitamin K antagonists (VKAs). The neutral results of SoSTART and APACHE-AF underline the need for more evidence to identify subgroups of patients with AF and ICH or intracranial haemorrhage in whom the effect of restarting anticoagulation might be either beneficial or hazardous.
There are no randomised comparisons of the timing of recommencing antithrombotics after ICH, nor any ongoing RCTs. Observational data from 2619 ICH survivors included in the Swedish Stroke Register suggest that the optimal timing of initiation of OACs is 7–8 weeks after the ICH for prevention of stroke or vascular death and minimising the risk of severe haemorrhage.27 In patients with mechanical heart valves, earlier reinitiation of anticoagulation (with heparins or VKAs) should be considered due to the high risk of valve thrombosis. Based on a multicentre cohort study, a start time between 6 and 13 days after ICH, depending on anticipated thromboembolic risk, might be optimal.28
Research priorities
Two further studies of antiplatelet use are ongoing (RESTART-Fr, NCT02966119, n=280; STATICH, NCT03186729, n=250), as are six further studies addressing whether to restart OACs in patients with AF who have had an ICH (table 1), mostly testing the use of NOACs against other strategies, including no OAC.29 Of these, NASPAF-ICH has completed inclusion, and a pooled analysis of SoSTART, APACHE-AF and NASPAF-ICH is planned.30 A3ICH is a three-arm trial also including left atrial appendage occlusion (LAAO). The potential advantage of LAAO is that long term antithrombotic medication can be avoided. However, after implantation of the device antiplatelet therapy is needed, initially dual therapy, then monotherapy for about 6 months. In STROKECLOSE (NCT 02830152), LAAO (followed by aspirin for at least 6 months with or without clopidogrel in the first 45 days) is compared with OAC, antiplatelet therapy or no antithrombotic therapy at all, for prevention of a composite of stroke (ischaemic or haemorrhagic), systemic embolism, life-threatening or major bleeding and all-cause mortality in patients with ICH. In this context one should consider that ischaemic stroke may arise from other origins than the left atrial appendage (in AF) and non-AF sources (eg, arteriosclerosis, small vessel disease) and it is debatable whether antiplatelet therapy should be stopped entirely after LAAO in patients at high risk of ischaemic stroke.
Ongoing trials of anticoagulation in patients with AF and previous ICH
Recommendations
Based on the currently available evidence, restarting antiplatelets in patients who have had an intracranial haemorrhage appears safe, and there is currently no clear preference for starting or avoiding OAC in patients with AF and previous ICH or intracranial haemorrhage. If starting OAC is considered, an NOAC is generally preferred over VKAs, although data remain limited in patients with ICH. Information on the timing of initiation of OACs after ICH is scare, but 7–8 weeks appears a sensible optimum for avoiding early haemorrhagic events and prevention of ischaemic complications. The place of LAAO is yet to be determined. We encourage randomisation into ongoing clinical trial of OAC and LAAO in patients with ICH and AF.
Antithrombotic medication in patients with cerebral microbleeds
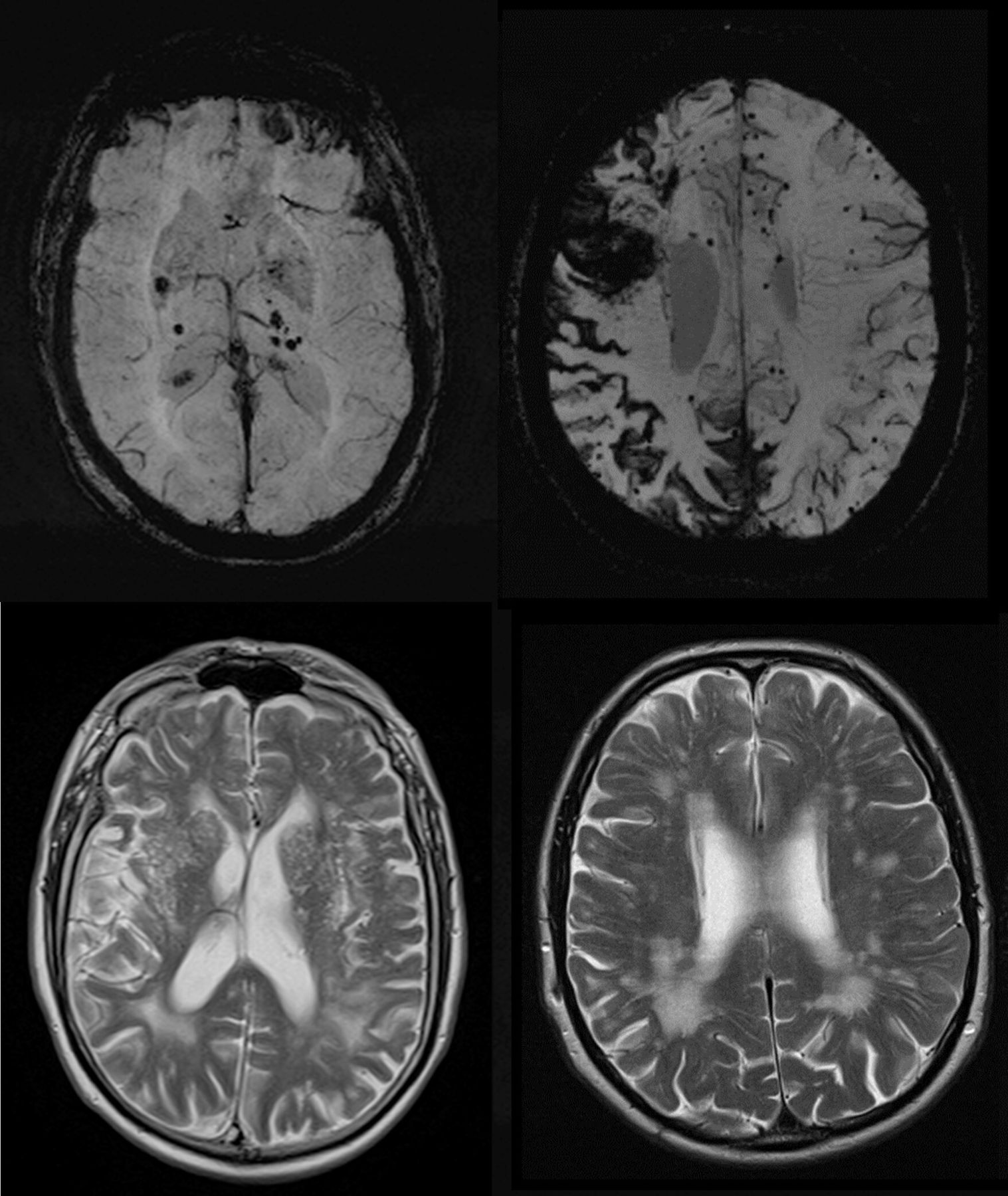
Cerebral microbleeds are small, black, rounded lesions seen on MRI scans sensitive to paramagnetic material; scans of this type include T2*-weighted gradient recalled echo and susceptibility-weighted imaging.31 Histological correlation studies indicate that most radiological microbleeds correspond, as hypothesised, to small areas of bleeding related to cerebral small vessels.32 Cerebral microbleeds have found clinical application as a biomarker of the presence and type of cerebral small vessel disease. In particular, a strictly lobar location has good diagnostic accuracy for CAA, at least in hospital-based cohorts of patients with symptomatic ICH (figure 1).33

Microbleeds in sporadic small vessel disease. Top, left, Susceptibility-weighted MRI sequences showing deep CMBs suggesting deep perforator arteriopathy, and right: strictly lobar CMBs with disseminated siderosis and evidence of previous lobar ICH, suggesting cerebral amyloid angiopathy respectively. Bottom: T2 sequences show compatible patterns of white matter hyperintensity and enlarged perivascular spaces. CMBs: cerebral microbleeds; ICH, intracerebral haemorrhage.
For the last two decades or so, microbleeds have generated substantial research interest as well as clinical anxiety regarding their potential role in predicting the future risk of intracranial haemorrhage. It is hypothesised that as a marker of fragile, bleeding-prone small vessels, microbleeds will be associated with increased intracranial bleeding risk, particularly in patients treated with antithrombotic drugs.
Current evidence
Multiple prospective cohort studies have now confirmed a clear association between increasing microbleed burden and intracranial haemorrhage risk.34 35 A recent large-scale international collaborative study has also demonstrated that cerebral microbleeds improve the prediction of intracranial haemorrhage in patients with previous ischaemic stroke or TIA, and that a cerebral microbleed-based risk score (the Microbleeds International Collaborative Network - Intracranial Haemorrhage score, MICON-ICH) has improved discrimination for intracranial haemorrhage compared with widely used clinical prediction instruments like the HAS-BLED (Hypertension, Abnormal renal/liver function, Stroke history, Bleeding, Labile international normalised ratio, Elderly, Drugs), ATRIA (Anticoagulation and Risk factors in Atrial Fibrilllation) or ORBIT (Outcomes Registry for Better Informed Treatment of Atrial Fibrillation) scores.36 However, the same data indicate that microbleeds are also associated with an increased risk of ischaemic stroke, although they do not appear to improve discrimination for ischaemic stroke risk over clinical variables alone.36 In a pooled analysis of individual patient data from 38 studies, the absolute risk of ischaemic stroke exceeded that of intracranial haemorrhage even in patients with 10 or more microbleeds (annual rates: intracranial haemorrhage: 2.7%; ischaemic stroke: 6.4%), or microbleeds in a strictly lobar distribution suggesting CAA (annual rates: intracranial haemorrhage: 1.3%; ischaemic stroke: 4.8%).35
Microbleeds have also been investigated in several RCTs of antithrombotic agents. Secondary analyses of the PERFORM and NAVIGATE-ESUS trials did not show any interaction of microbleeds at baseline with allocated treatment effects.37 38 This suggests that microbleeds do not modify the net benefit or harm of antithrombotic therapy. However, in the PICASSO (Prevention of Cardiovascular Events in Asian Patients with Ischaemic Stroke at High Risk of Cerebral Haemorrhage) trial, which enrolled participants with previous ischaemic stroke and high intracranial bleeding risk (evidenced by a history of symptomatic intracranial haemorrhage, radiological evidence of previous ICH, or the presence of two or more cerebral microbleeds), a substudy found that in those with microbleeds only at baseline, cilostazol was associated with a lower risk of intracranial bleeding than aspirin (HR 0.08, 95% CI 0.01 to 0.61).39
Research priorities
By using microbleeds to identify patients at highest risk, it may be possible to test new interventions that may have a lower intracranial bleeding risk. For example, in those with AF, the assessment of cerebral microbleeds could help prevent intracranial haemorrhage by identifying patients in whom LAAO should be considered.40 In those with non-cardioembolic ischaemic stroke or TIA, microbleeds could identify patients for trials of antithrombotic agents with lower expected bleeding risk, for example, cilostazol.
Cortical superficial siderosis (cSS) is associated with CAA, and a very high risk of future ICH in patients meeting modified Boston criteria, which might exceed that of ischaemic stroke (26.9% /year in patients with extensive bilateral cSS included in a single centre prospective cohort study).41 Whether antithrombotic treatment should be modified or withheld in patients with cSS not meeting modified Boston criteria or without previous ICH should be investigated, though very large studies would be needed due to its rarity in such patients.42
Recommendations
Based on the available data, the presence or burden of microbleeds should not preclude the use of antithrombotic therapy (antiplatelet drugs or OAC) for secondary prevention of ischaemic stroke or TIA. Accurate predictions regarding future intracranial haemorrhage risk (eg, using the MICON-ICH score) can nevertheless inform discussions about prognosis and highlight patients in whom measures to mitigate bleeding risk (such as intensive blood pressure control, avoiding alcohol and careful review of concomitant medication) should be prioritised and monitored particularly closely.
Antithrombotic strategies in patients with indications for both anticoagulant and antithrombotic treatment
Many patients with AF have vascular disease, whether coronary, carotid or peripheral artery disease. In such patients, there is both a need to prevent stroke due to AF, which requires OAC, and to prevent stroke due to vascular disease, which in the non-AF setting usually requires antiplatelet therapy. In AF patients with associated coronary artery disease, antithrombotic management varies between acute and stable clinical scenarios. In those presenting with an acute coronary syndrome, a balance must be found between AF-related stroke prevention which requires OAC; reducing cardiac ischaemia in an acute coronary syndrome presentation which requires antiplatelet therapy; minimising the risk of stent thrombosis after a percutaneous coronary intervention; and the risk of bleeding posed by combining OAC and antiplatelet therapy.43
Current evidence
Avoiding long-term combination therapy in AF patients with coronary artery disease without a recent acute coronary syndrome is supported by a systematic review and meta-analysis of observational data,44 which showed similar rates of thrombotic and ischaemic events in patients treated with single antiplatelet therapy and OAC compared with oral anticoagulation alone (HR 1.09, 95% CI 0.92 to 1.29), but higher rates of major bleeding with the former (HR 1.61, 95% CI 1.38 to 1.87). The AFIRE (Atrial Fibrillation and Ischemic Events with Rivaroxaban in Patients with Stable Coronary Artery Disease) trial compared single antiplatelet therapy and rivaroxaban to rivaroxaban alone in patients with AF and stable coronary artery disease. Although it was stopped early for increased mortality in the combined treatment group, the trial demonstrated non-inferiority of rivaroxaban alone for a composite primary outcome of stroke, systemic embolism, myocardial infarction, coronary revascularisation and death (HR 0.72, 95% CI 0.55 to 0.95), and superiority for major bleeding (HR 0.59, 95% CI, 0.39 to 0.89).45 This observation was evident irrespective of CHA2DS2VASc or HAS-BLED scores.46
In a systematic review and meta-analysis, the pooled prevalence of carotid stenosis in AF patients was 12.4% (95% CI 8.7% to 16.0%), with reported prevalence ranging from 4.4% to 24.3%.47 The pooled prevalence of carotid plaque was 48.4% and the prevalence of AF in patients with carotid stenosis was 9.3% (range 3.6–10.0). Thus, about 1 in 10 patients with AF have carotid stenosis, and vice versa. Also, non-stenotic carotid disease is present in about half of AF patients. Despite this, few data exist to guide the management of patients with AF and carotid or peripheral arterial disease, but the increased bleeding risk with combination therapy observed in patients with coronary artery disease might reasonably be expected in these patients.48 In the absence of evidence that concomitant antiplatelet therapy reduces the risk of stroke or major cardiovascular events, European guidelines recommend against its use in patients with peripheral arterial disease without vascular events in the last twelve months.49
In high-risk stable atherosclerotic vascular disease patients without AF, the COMPASS trial randomised 27 395 participants to receive rivaroxaban 2.5 mg two times per day plus aspirin 100 mg one time per day, rivaroxaban 5 mg two times per day or aspirin 100 mg one time per day.50 The incidence of the primary outcome, a composite of cardiovascular death, stroke or myocardial infarction, was lower in the rivaroxaban-plus-aspirin group compared with the aspirin-alone group (4.1% vs 5.4%; HR 0.76, 95% CI 0.66 to 0.86). Although more major bleeding events occurred in the combination group (3.1% vs 1.9%; HR 1.70, 95% CI 1.40 to 2.05), mortality was also lower (HR 0.82, 95% CI 0.71 to 0.96), without an increase in intracranial or fatal bleeds. Of the secondary outcomes, ischaemic stroke was significantly lower with combination therapy compared with aspirin (HR 0.51, 95% CI 0.38 to 0.68), and with rivaroxaban alone vs aspirin (HR 0.69, 95% CI 0.53 to 0.90). In the subgroup of patients with stable peripheral or carotid artery disease, combination therapy also significantly reduced major adverse cardiovascular and peripheral arterial events as well as stroke, when compared with aspirin monotherapy, but again with more major bleeding.51 Rivaroxaban alone did not significantly reduce major adverse cardiovascular events or stroke compared with aspirin alone, but did reduce major adverse limb events and increased major bleeding.
Research priorities
Whether a similar combination therapy strategy as in the COMPASS trial would be beneficial in patients with AF and vascular disease is uncertain. More clinical trials are needed to establish the best antithrombotic strategy for ischaemic stroke prevention in AF patients with evidence of large arterial disease, such as complex aortic plaque or symptomatic (and severe) carotid disease. In addition, emerging technologies have been proposed, such as use of the percutaneous permanent carotid filter which is investigated in the CAPTURE (Carotid Artery Implant for Trapping Upstream Emboli for Preventing Stroke in Atrial Fibrillatio Patients) trial.52
Recommendations
The current recommended management approach after an acute coronary syndrome in a patient with AF is to have an initial 1-month period of triple therapy with OAC, aspirin and a P2Y12 inhibitor (usually clopidogrel), after which the patient is managed with OAC plus a single antiplatelet (usually clopidogrel) (figure 2). In patients with a relatively low risk of thromboembolism and a particularly high risk of bleeding (eg, HASBLED score of 3 or higher; previous ICH with high recurrence risk, for example, lobar location or probable CAA), the initial triple therapy period may be omitted.43 Once ‘stable’ (arbitrarily defined as 12 months onwards) the patient is managed with OAC monotherapy, either an NOAC or well-managed VKA with a time in therapeutic range ≥70%, with a preference for an NOAC given their better safety profile in clinical trials.53

Suggested antithrombotic management for patients with atrial fibrillation undergoing PCI for an acute coronary syndrome (ACS). AF, atrial fibrillation; NOAC, non-vitamin K oral anticoagulants; PCI, percutaneous coronary intervention.
When combination therapy is used, efforts to mitigate bleeding risk are particularly important, and should aim to address modifiable bleeding risk factors (including hypertension, alcohol excess and pharmacokinetic and pharmacodynamic drug interactions), and identify the patients with the highest bleeding risk for early review and follow-up. Such a strategy has been tested in a prospective cluster RCT of AF patients (with or without comorbid vascular disease), resulting in a reduction in major bleeding at 1 year and an increase in OAC use.54 We should also not forget that stroke prevention is only one aspect of the integrated approach to AF care, as reflected in the Atrial fibrillation Better Care pathway recommended in the 2020 European Society of Cardiology guidelines.49 ‘A’ refers to Avoid stroke/Anticoagulation; ‘B’ Better symptom management with patient-centred decisions on rate or rhythm control’ and ‘C’ Cardiovascular risk factor and comorbidity optimisation.55 This pathway has been shown to reduce adverse outcomes in patients with AF, in various independent cohorts.56–60
Anticoagulant initiation after acute AF-associated ischaemic stroke
Around two-thirds of patients with cardioembolic ischaemic stroke are already known to have AF at presentation or will be diagnosed with AF during their initial hospitalisation.61 While the long-term benefit of OAC for stroke prevention in AF is well established,62 63 these patients pose the additional challenge of deciding when anticoagulation should be initiated or resumed.64 In the first 2 to 4 weeks after AF-associated ischaemic stroke, the daily risk of recurrence is around 0.5% if untreated.65–67 This must be balanced against the risk of clinically significant haemorrhagic transformation, roughly 0.4% per day in the first week after stroke,68 which might be increased by early anticoagulation. RCTs of anticoagulation with heparin or VKAs suggest that initiation within 48 hours of onset is not of net benefit compared with more delayed initiation, with weak evidence of a reduction in recurrent ischaemic stroke outweighed by clear evidence of an increased risk of symptomatic intracranial haemorrhage.69 Consistent with this, current guidelines suggest delaying anticoagulation by up to 2 weeks (table 2),11 48 49 70–73 a period based largely on expert opinion and small historical studies describing the time course of haemorrhagic transformation.74 75 The increasing use of NOACs suggests a need to review this practice, as NOACs pose half the risk of intracranial haemorrhage of VKAs, at least in the long term,63 and might therefore offer favourable risk-benefit balance in the acute phase.
Current guidelines on anticoagulation initiation timing after ischaemic stroke
Current evidence
The initial results of the TIMING study were presented at the European Stroke Organisation Conference in September 2021.76 To date, these are the only RCT data on when to initiate anticoagulation with an NOAC after AF-associated ischaemic stroke. In 888 participants randomised to anticoagulation initiation at 0–5 or 5–10 days from stroke and followed up for 90 days, early anticoagulation was statistically non-inferior (based on a prespecified margin of 3%) to delayed anticoagulation. The absolute risk of the composite primary outcome of ischaemic stroke, symptomatic ICH and mortality was lower in the early anticoagulation group, but superiority was not demonstrated. Most included patients had mild ischaemic stroke (defined clinically), and no ICH occurred in either study arm. These results provide some reassurance regarding the safety of early anticoagulation, but further RCTs are needed to establish the optimal timing of anticoagulation, both in patients with mild stroke, and those with moderate or severe stroke. Three RCTs are currently recruiting (OPTIMAS, ELAN and START) (table 3).
Completed and ongoing trials of anticoagulation timing after AF-associated ischaemic stroke
Several observational studies have also reported outcomes according to anticoagulation timing (online supplemental table 1). Collectively, these studies suggest that early anticoagulation with an NOAC is not associated with a high risk of intracranial haemorrhage, and that this risk is low compared with that of recurrent ischaemic stroke.77–83 Unexpectedly, several studies of these studies found numerically higher intracranial haemorrhage rates with more delayed anticoagulation, or similar or higher rates of recurrent ischaemia in early treatment groups.80–83 Given substantial imbalances in stroke severity, size and the presence of haemorrhagic transformation between groups, these results are likely to be confounded by treatment bias. For instance, while unadjusted event rates from the RAF-NOACs study suggested the optimal timing of anticoagulation might lie between 4 and 14 days after onset, a finding that has influenced current guidelines,73 a multivariable analysis correcting for confounding factors found no significant association between initiation period and the study composite outcome.78
Supplemental material
Research priorities
Once robust data from clinical trials are available, subgroup analyses might allow the development of a personalised approach to anticoagulation initiation, based on an individualised assessment of the risks of haemorrhagic transformation and recurrent ischaemic stroke. Currently, stroke severity and the presence of haemorrhagic transformation on initial imaging are major determinants of anticoagulation timing, influenced by the European Society of Cardiology’s 2016 ‘1-3-6-12’ rule.84 85 However, clinically assessed stroke severity is an imperfect proxy for the volume of infarcted tissue, which is likely to be a more direct determinant of the risk of haemorrhagic transformation.86 A considerable mismatch is not uncommon, for example in a thalamocapsular infarct causing a severe sensorimotor syndrome, or in a large posterior cerebral artery infarct causing hemianopia alone. Increasing infarct size is also associated with an increased risk of recurrent ischaemic stroke in patients with AF,86 suggesting it may not reliably discriminate between patients who should be anticoagulated soon after stroke, and those in whom anticoagulation should be delayed. Accordingly, this rule has been removed from the updated 2020 guideline.49
Haemorrhagic transformation on initial imaging also generally delays anticoagulation.87 However, minor haemorrhagic transformation (haemorrhagic infarction by ECASS classification) is common after cardioembolic stroke,88 is not clearly associated with worse clinical outcome,89 and has not been shown to affect the risk–benefit balance of early anticoagulation. Haemorrhagic infarction might indicate diffuse low-pressure bleeding from necrotic brain tissue, rather than the focal, higher-pressure bleeding, possibly triggered by reperfusion90 that forms a parenchymal haematoma associated with poor clinical outcomes (ECASS parenchymal haematoma type 2). Early anticoagulation initiation might therefore be insufficient to convert haemorrhagic infarction to a parenchymal haematoma. In 96 patients with baseline haemorrhagic transformation included in nine observational studies of early anticoagulation,91–99 none experienced symptomatic intracranial haemorrhage. However, it has also not been proven that delaying anticoagulation increases the risk of recurrent stroke: in a pooled analysis of the RAF and RAF-NOAC studies, delaying initiation by a mean of 12 days in patients with haemorrhagic transformation did not lead to additional recurrent ischaemic strokes compared with patients without haemorrhagic transformation.87 Secondary analyses including functional outcome measures, considering the higher morbidity and mortality of ICH than ischaemic stroke, would also be informative.
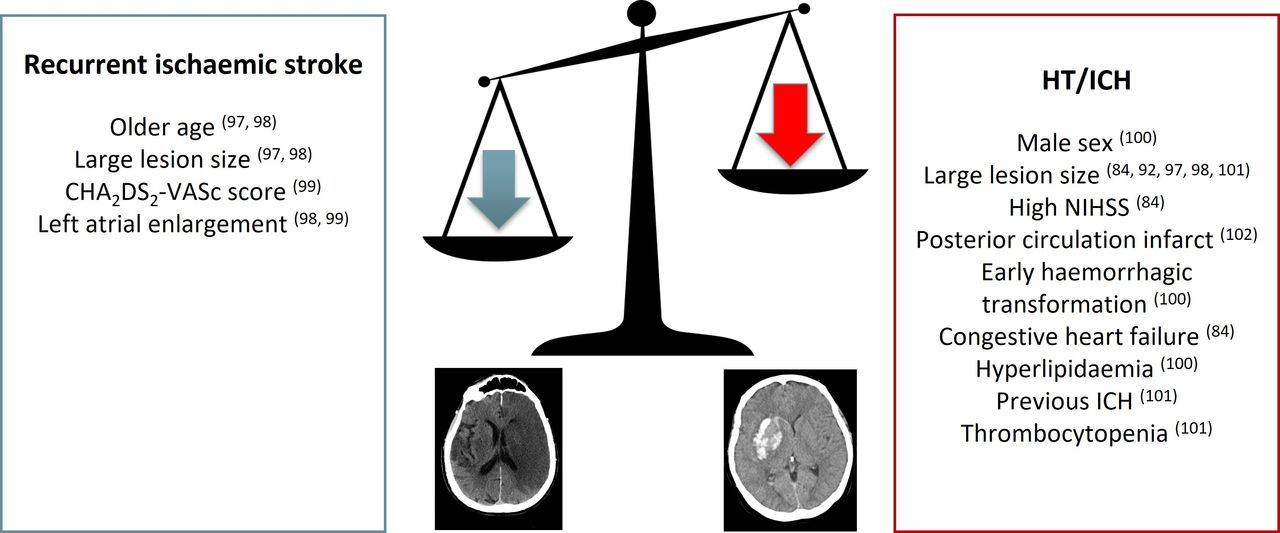
Observational studies in patients with AF and recent stroke have identified numerous other risk factors for early recurrent ischaemic and haemorrhagic events (figure 3).87 95 100–105 There is a need to synthesise these into risk models suitable for clinical application, as existing prediction models intended for use in AF, such as CHA2DS2-VASc and HAS-BLED, are validated for long-term use. Even more risk factors have been identified in patients with recent ischaemic stroke of any aetiology, including diabetes and hyperglycaemia, renal function, the hyperintense middle cerebral artery sign, leukocytosis, hypertension, obesity, smoking and alcohol habits, and elevated C reactive protein.106–109 These have been included in scoring systems which predict early recurrence110 111 or haemorrhagic transformation (mainly postthrombolysis)112–114 in all-cause ischaemic stroke with reasonable accuracy. In the absence of AF-specific models for early recurrence or bleeding, these scores might be investigated for use in risk stratification, although some components of these scores might be significant mainly as surrogate markers for AF.

Reported predictors of ICH and recurrent stroke in patients with recent AF-related ischaemic stroke. AF, atrial fibrillation; HT, haemorrhagic transformation; ICH, intracerebral haemorrhage; NIHSS, National Institutes of Health Stroke Scale
Recommendations
In light of the limitations of current evidence, offering enrolment in an RCT, if available, is likely to represent the best clinical care for most patients. In centres not participating in a relevant RCT, early anticoagulation within 5 days of onset might be appropriate in most patients with minor stroke, with later initiation in patients with moderate or severe stroke.64 In the absence of severe symptomatic intracranial haemorrhage, we recommend anticoagulation initiation within 14 days in all patients. We prefer NOAC use in the absence of a definite indication for VKA treatment.
Antithrombotic ‘failure’
As antithrombotic medication is the mainstay of stroke prevention in cardiovascular medicine, many patients with ischaemic stroke are on antithrombotic therapy prior to stroke onset. Management of these break-through strokes (‘treatment failure’ describes this scenario insufficiently) is a frequent and major challenge in cerebrovascular medicine.
Current evidence
Antiplatelet therapy using aspirin provides a modest risk-reduction for recurrent stroke not related to AF.115 However, ischaemic stroke despite antiplatelet therapy is frequent, with recent data suggesting 20%–35% of patients with stroke were on antiplatelet therapy at stroke onset.116 117 Prior antiplatelet therapy has been found to be associated with reduced stroke severity.116 117 Reasons for stroke despite antiplatelet therapy may include insufficient reduction of platelet aggregation by aspirin and other antiplatelet agents or underlying stroke aetiologies, where antiplatelet therapy is less effective (eg, AF, ipsilateral high-grade carotid stenosis).
Although in vivo platelet function testing118 and testing for genetic polymorphisms predisposing for reduced efficacy of different antiplatelet agents are available, their role to guide treatment decisions is currently debated not only in neurology but also in cardiology.119 120 A recent meta-analysis121 identified addition of or switch to a different antiplatelet agent to be associated with fewer vascular events but no RCT has yet investigated optimal treatment strategies.
Dual-antiplatelet therapy combining aspirin and clopidogrel has been shown to be an effective therapy in patients with minor stroke or high risk TIA used for a limited period after the event.122 Recurrent stroke despite dual antiplatelet therapy was found to be associated with CYP2C19 loss-of-function allele status in a subanalysis of patients enrolled in the CHANCE trial (from China)123 while there was no association between loss-of-function allele status and recurrent stroke among patients enrolled in the POINT trial (mostly from Europe and the USA). However, genetic testing to guide clinical decisions is not currently standard of care and there are limited data to recommend its use.
Anticoagulation using NOACs or VKAs is highly effective in preventing ischaemic stroke and systemic embolism in patients with AF.62 63 However, patients with AF may have stroke despite taking NOAC or VKA, with a rate of 1.0%–1.5% per year in RCTs.124–127 Recent data from the USA (2012–2015)128 and Switzerland (2015–2019)129 found that among patients with AF (known before or newly diagnosed after stroke onset) who had a stroke, 30% (USA) and 38% (Switzerland) were taking any OAC at the time of stroke onset. 8.8% of participants in the USA and 20% in Switzerland were taking an NOAC at onset. Thus, with more than one out of three patients with AF taking anticoagulants at the time of stroke onset, this represents a major challenge not only for acute recanalisation therapies130 131 but also for secondary prevention.
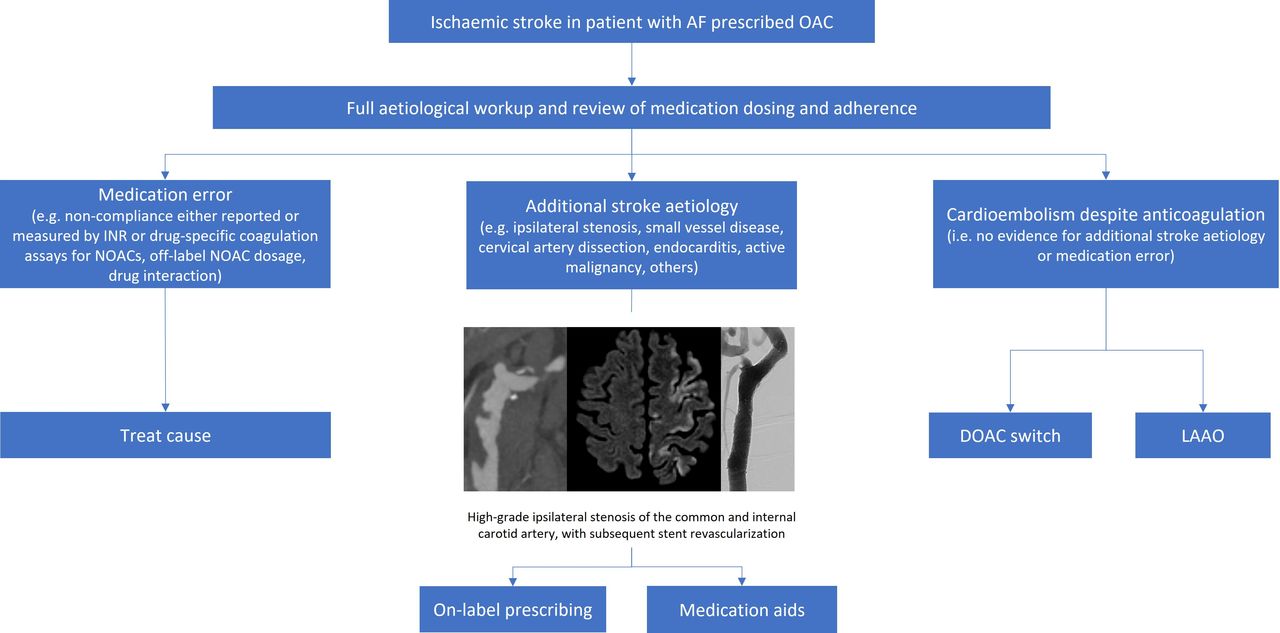
Reasons for having a stroke despite anticoagulant therapy are heterogeneous and poorly understood. Three different clusters should be distinguished (figure 4): (1) competing stroke aetiology (eg, stroke due to large artery arteriosclerosis, small vessel disease, cervical artery dissection, endocarditis, active malignancy or other determined origins); (2) medication error (eg, lack of compliance, use of non-label NOAC dosage, pharmacokinetic drug interactions reducing anticoagulant efficacy) and (3) cardioembolism despite anticoagulation (no evidence for competing stroke aetiology or medication error). Using the ASCOD132 classification (a multicause aetiological classification system of stroke causes), in 95% of patients at least one potential additional non-cardiac cause of stroke was identified.133 However, in the same study, medication error (eg, VKA therapy with INR <2.0 at stroke onset, non-label NOAC dosage or low NOAC plasma levels) was observed in 55% of patients. A multicentre study of patients with stroke despite NOAC therapy found comparable results with non-cardioembolic stroke aetiology and NOAC dosing error being frequent.134 A thorough aetiological work-up including investigation of additional stroke aetiologies (eg, vessel imaging, MRI) and anticoagulation dosing and adherence should be a standard of care for patients with AF who have a stroke despite anticoagulant therapy. Review of concomitant medication is particularly important in patients prescribed NOACs, as monitoring of anticoagulant effect is not routine. Drugs expected to reduce NOAC plasma levels include rifampicin, carbamazepine, phenytoin, phenobarbitone, primidone and St Johns’ wort (P-glycoprotein or CYP3A4 inducers). Whether NOAC monitoring leads to clinical benefit in patients who cannot stop interacting medication is uncertain.135

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Suggested approach to patients with ischaemic stroke despite oral anticoagulation. AF, atrial fibrillation; DOAC, direct OAC; LAAO, left atrial appendage occlusion; NOAC, non-vitamin K OAC; OAC, oral anticoagulant.
An international, multicentre study found that patients with AF who had a stroke despite anticoagulant therapy (88.8% VKA) are at increased risk of having another stroke (HR 1.6, 95% CI 1.2 to 2.3) with an annualised rate of 8.9% per year.136 In this study, anticoagulation was changed (eg, switching between VKA and NOAC therapy, or changing the type of NOAC) in 31% of patients, but most patients continued the same anticoagulant therapy as before the stroke. Neither treatment—change of anticoagulation or continuing the same anticoagulant as before stroke—was associated with decreased hazard of recurrent stroke.
Research priorities
The optimal secondary prevention therapy after stroke despite anticoagulant therapy in patients with AF remains unclear. Future studies should focus on potential mechanisms of stroke (eg, additional aetiology and medication error) and new treatment options for those with cardioembolism despite anticoagulation. Such treatments might include LAAO, as the recent LAAOS-III (Left Atrial Appendage Occlusion Study III) trial found that LAAO with anticoagulation reduced ischaemic stroke risk compared with anticoagulation alone (HR 0.67; 95% CI 0.53 to 0.85), although in patients undergoing cardiac surgery for a separate indication.137
Recommendations
In the absence of evidence from RCTs, figure 4 includes suggestions for work-up and secondary prevention therapy with respect to the most probable underlying cause of ischaemic stroke despite OAC. In patients with recurrence despite antiplatelet therapy, the possibility of a previously unrecognised and treatable cause should be considered. Short-term dual antiplatelet therapy is generally indicated. There is insufficient evidence to recommend platelet function or genetic testing as standard of care, but this approach might help to provide personalised treatment options in selected patients.
Silent stroke and asymptomatic small vessel disease
Whether aspirin or other antithrombotics should be used to prevent first-ever stroke or myocardial infarction in patients with incidentally discovered silent stroke, high white matter hyperintensity (WMH) burden or microbleeds is controversial, without evidence from high-quality RCTs. This clinical scenario arises frequently, as the prevalence of silent cerebrovascular disease is high in older patients undergoing neuroimaging for indications unrelated to stroke. Population-based studies show that more than 20% of persons older than 80 have either one or more brain infarcts, high WMH burden or one or more cerebral microbleeds.138 139
Current evidence
Observational evidence shows that the presence of brain infarcts, high WMH and microbleeds are associated with higher risk for future stroke, even after accounting for the higher risk factor burden in patients with these lesions. In a systematic review and meta-analysis,140 stroke risk was substantially elevated in persons with silent brain infarcts (HR 2.38, 95% CI 1.87 to 3.04), high WMH (HR 2.45, 95% CI 1.93 to 2.12) and microbleeds (HR 1.89, 95% CI 1.55 to 2.53), independent of hypertension and other vascular risk factors.
Thus, these signs of clinically unrecognised cerebrovascular disease mark patients at higher risk of stroke who might benefit from the application of vascular risk reduction strategies. Some guidelines recommend a risk-based approach for primary prevention; for example, by recommending statins based on the estimated 10-year probability of having a stroke or MI.141 From that perspective, the presence of silent cerebrovascular disease might favour applying additional management strategies for patients at high risk. However, the commonly used validated prediction models for stroke and MI risk are based on demographics, risk factors and simple physiological and laboratory measurements, without incorporating MRI information. MRI information probably improves the classification of risk,142 but prediction models using MRI have not yet been derived and externally validated for widespread use in patients without previous clinically diagnosed ischaemic stroke or TIA.
The potential downsides of aspirin therapy must also be considered. The pathophysiology of silent cerebrovascular disease is less certain than for symptomatic stroke. In the elderly, most silent brain infarcts are lacunes. Silent lacunes may have a different pathophysiology than symptomatic lacunar infarctions caused by occlusion of lenticulostriate and basilar arteries, and may not be related to thrombosis.143 One study failed to find evidence that genetic predisposition to thrombosis was associated with lacunes even though it was associated with cardioembolic and large artery stroke.144 The pathophysiology of WMH is even less certain, with increasing evidence that elevated blood-brain permeability is a key step.145 Two trials, of warfarin146 and aspirin,147 found that antithrombotic treatment increased the risk of ICH in patients with high WMH burden. Some patients with high WMH have underlying CAA, a vasculopathy that predisposes to ICH.148 Microbleeds are associated with higher risk of first ever ICH in the general population, but are also associated with higher risk of future ischaemic stroke such that in persons with microbleeds the overall absolute number of new ischaemic strokes exceeds the number of new ICHs.149
The applicability of aspirin for patients with silent cerebrovascular disease must also be considered in light of recent trials (without neuroimaging) that either failed to find a beneficial effect of aspirin or found a small effect similar in size to the increased harm from major bleeding.150 Contemporary guidelines either do not recommend aspirin use for primary prevention151 or only recommend that it be considered in higher risk patients (based on cardiovascular risk factor profile or predicted risk from validated models) but not in the elderly older than 70.152
Research priorities
To address current gaps in knowledge, studies are needed to develop and validate models to stratify the risks of stroke and cardiovascular disease in persons with and without silent cerebrovascular disease, and to test antithrombotic strategies. The relevance of different forms of cerebrovascular disease (eg, lacunes vs WMHs) requires further investigation.
Recommendations
Given current uncertainties, care should be individualised. A Scientific Statement from the American Heart Association recommends that patients with silent brain infarcts or high WMH should be considered at high risk for stroke, but without specific recommendations on aspirin.139 A Canadian dementia guideline recommends against prescribing aspirin to patients with high WMH without brain infarction, but weakly recommends that aspirin could be considered in patients with cognitive impairment and silent brain infarcts with low quality of supporting evidence.153 The European Stroke Organisation recommends against use of aspirin in patients with silent cerebral small vessel disease, based on inconclusive evidence from one small trial.154 We recommend that aspirin should generally not be used in patients with silent cerebrovascular disease, unless there is another indication such as a clinical history of TIA, ischaemic stroke or myocardial infarction. However, in patients with non-lacunar brain infarction, the use of aspirin can be considered, particularly if there is an embolic pattern of infarction or there is evidence that atherosclerosis or atheroembolism is the likely cause.
Conclusion
Table 4 summarises recommendations based on the available evidence for each antithrombotic dilemma. Although recent evidence from large-scale observational studies and a limited number of RCTs has provided reassurance about the use of antithrombotic therapy in high-risk populations—specifically antiplatelets in those with previous ICH, and antiplatelets and anticoagulants in those with high microbleed burdens (but not necessarily CAA)—many uncertainties remain. Ongoing RCTs should soon establish the optimal time to start anticoagulants after ischaemic stroke in patients with AF, and whether anticoagulants can be used safely in those with previous ICH (and the role of LAAO after ICH). Other clinical dilemmas are further from resolution, notably the role of combination antithrombotic therapy in patients with AF and peripheral or coronary artery disease, the best approach to stroke prevention when antithrombotic treatment appears to have failed, and the use of antithrombotics in patients with cerebrovascular disease without clinical stroke or TIA. New data have not only resolved some old challenges, but highlighted new ones: more well-designed RCTs are, as always, needed.
Summary of recommendations
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DJW had the idea for the article, and developed the outline with JB. All authors drafted sections of the manuscript, critically reviewed and revised the manuscript for intellectual content and approved the final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DJW reports personal fees from Bayer, Alnylam and Portola outside the submitted work. EES reports personal fees from Alnylam Pharmaceuticals, Bayer and Portola, outside the submitted work. GL reports consultancy and speaker fees from Bayer, Bayer/Janssen, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Microlife, Roche and Daiichi-Sankyo outside the submitted work. DJS reports funding from Bayer and Pfizer, outside the submitted work.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.