Article Text

Abstract
Background Depression and anxiety frequently accompany the motor manifestations of isolated adult-onset focal dystonias. Whether the body region affected when this type of dystonia first presents is associated with the severity of these neuropsychiatric symptoms is unknown.
Objectives The aim of this study was to determine whether depression, anxiety and social anxiety vary by dystonia onset site and evaluate whether pain and dystonia severity account for any differences.
Methods Patients with isolated focal dystonia evaluated within 5 years from symptom onset, enrolled in the Natural History Project of the Dystonia Coalition, were included in the analysis. Individual onset sites were grouped into five body regions: cervical, laryngeal, limb, lower cranial and upper cranial. Neuropsychiatric symptoms were rated using the Beck Depression Inventory, Hospital Anxiety and Depression Scale and Liebowitz Social Anxiety Scale. Pain was estimated using the 36-Item Short Form Survey.
Results Four hundred and seventy-eight subjects met our inclusion criteria. High levels of depression, anxiety and social anxiety occurred in all groups; however, the severity of anxiety and social anxiety symptoms varied by onset site group. The most pronounced differences were higher anxiety in cervical and laryngeal, lower anxiety in upper cranial and higher social anxiety in laryngeal. Increases in pain were associated with worse neuropsychiatric symptom scores within all groups. Higher anxiety and social anxiety in laryngeal and lower anxiety in upper cranial persisted after correcting for pain and dystonia severity.
Conclusion Anxiety and social anxiety severity vary by onset site of focal dystonia, and this variation is not explained by differences in pain and dystonia severity.
- Isolated focal dystonia
- anxiety
- depression
- pain
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Isolated dystonia is a group of movement disorders characterised by sustained or intermittent involuntary muscle contractions that lead to abnormal and often repetitive movements, postures or both.1 These disorders are not accompanied by other neurological abnormalities except for tremor, and have no known cause except for relatively rare gene mutations.2 The most common form of isolated dystonia is adult-onset focal dystonia (AOFD), defined by dystonia that begins in adulthood and primarily affects one body region such as the face, neck or limbs.3
In addition to the characteristic motor symptoms, non-motor symptoms, such as depression, anxiety and social anxiety, are commonly seen in AOFD and can significantly contribute to disability,4–7 as well as diminish quality of life.8–11 Such neuropsychiatric manifestations may occur secondary to the development of dystonia, but their onset often precedes motor symptoms.12 13 Furthermore, in a number of studies, depression severity does not correlate with the dystonia severity nor does depression improve when dystonia is treated.5 14 Thus, depression and anxiety appear to be a feature of the clinical spectrum of AOFD and not just a reaction to motor symptoms. The pathophysiology underlying both motor and non-motor symptoms in AOFD, however, remains poorly understood.
Although different AOFD phenotypes share some aetiological and pathophysiological features,15 16 variations in a number of epidemiological and aetiological factors occur.17 Identifying differences in the neuropsychiatric manifestations for distinct AOFD phenotypes could enhance our understanding of the aetiology and pathophysiology underlying varying motor phenotypes, and also help clinicians more effectively recognise and treat these non-motor symptoms in their patients with AOFD. Presently, whether the type or severity of neuropsychiatric symptoms vary across different presentation of AOFD is not known, and small sample sizes, limited dystonia phenotypes, varying clinical assessment tools and lack of comorbid pain assessments impair generalisation from prior studies.7 In this study, we sought to address these prior limitations by investigating the severity of depression, anxiety and social anxiety in a large multi-centre cohort of recent-onset AOFD patients and determine whether symptom severity differs by initial site of onset. We further sought to assess whether differences in reported bodily pain and dystonia severity underlie any variance in the severity of these neuropsychiatric symptoms across different AOFD phenotypes.
Methods
Study participants
Participant data were acquired from the Natural History Project database of the Dystonia Coalition (https://www.rarediseasesnetwork.org/cms/dystonia), a multi-centre, cross-sectional study of subjects diagnosed with isolated, idiopathic dystonia. Subjects 18 years of age or older with isolated dystonia affecting any body region and presence of symptoms for no more than 5 years were enrolled across 28 clinical sites in the USA, Canada, Germany, France and Italy (see online supplementary appendix 1 for list of additional dystonia coalition investigators that contributed subjects included in our analysis). We excluded comorbidities that would confound diagnosis or evaluation other than dystonia or tremor, including medical or neurological disorders that would preclude completing the neurological examination protocol and questionnaires. Subjects receiving botulinum toxin injections were enrolled at least 2 months after their last injection. This study included all participants enrolled in the Natural History Project between 12 January 2011 and 6 April 2016.
Standard protocol approvals, registrations and patient consents
The study was approved by the Internal Review Boards of all participating clinical sites. All subjects gave written informed consent for participation in the study following the principles of the Declaration of Helsinki.
Dystonia phenotype
Subjects were categorised according to their initial site of dystonia, which included five regions: cervical (neck and shoulder), laryngeal (larynx), limb (upper arm, hand, upper leg and foot), lower cranial (lower face, tongue and jaw) and upper cranial (upper face). Subject data were excluded from analyses if onset site was the trunk or pelvis, not reported, or if more than one body region was reported as being initial sites of dystonia.
Rating scales
A movement disorders neurologist performed all subject motor evaluations using the Global Dystonia Rating Scale (GDRS)18 and the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS).19 The GDRS rates the presence and severity of dystonic signs in 10 different body parts—eyes and upper face, lower face, jaw and tongue, larynx, neck, shoulder and proximal arm (left and right), distal arm and elbow (left and right), proximal leg and pelvis (left and right), distal leg and foot (left and right) and trunk—and has been validated for internal consistency, inter-rater reliability and clinical applicability.18 The BFMDRS is a validated rating scale to assess the severity of dystonia and provoking factors affecting seven body regions and functions—eyes, mouth, speech/swallowing, neck, trunk, upper limb (left and right) and lower limb (left and right).
We captured depressive and anxiety symptoms with the Beck Depression Inventory, 2nd edition (BDI),20 the Hospital Anxiety and Depression Scale (HADS)21 and the Liebowitz Social Anxiety Scale (LSAS).22 The BDI is a 21-item self-reported instrument for depression rated on a 4-point scale (0–3) leading to a maximum score of 63 and has been shown to have high validity and reliability across a broad range of clinical and non-clinical populations.23 The HADS assesses self-reported severity of anxiety (HADS-A) and depression (HADS-D), with seven questions each yielding scores ranging from 0 to 21. The HADS has demonstrated good validity, sensitivity and specificity in the general population24 and has been used previously in studies of dystonia.11 Finally, the self-reported LSAS is a 24-item scale that assesses both fear/anxiety symptoms and avoidance behaviour using a 4-point scale (0–3) for each item yielding a maximum score of 144. The LSAS is a validated scale with high sensitivity and specificity for social anxiety25 and has been used in dystonia populations.26
The severity of pain in dystonia patients was assessed using the bodily pain domain of the 36-Item Short Form Survey (SF-36), a generic quality of life questionnaire to measure mental and physical well-being. We quantified pain by adding item 21 (severity of bodily pain over last 4 weeks on scale of 1–6) and item 22 (interference with physical functioning caused by bodily pain over last 4 weeks on scale of 1–5).
Statistical analysis
The severity of dystonia and neuropsychiatric symptoms was compared across AOFD phenotypes using a one-way analysis of variance. Group differences were first evaluated using an overall F test, and if significant at p<0.05 pairwise t-tests were performed. Tukey-Kramer adjustments for multiple comparisons were applied to all pairwise comparisons. In addition, the presence of depression, anxiety and social anxiety was dichotomised using standard scale cut-offs for clinically significant symptoms (BDI >13; HADS-D/HADS-A >7; and LSAS >30), and differences among dystonia onset sites were investigated using two-way χ2 tests or Fisher exact tests and logistic regression. Interactions between pain and dystonia severity versus region of dystonia onset were examined by testing for different slopes of the linear best fit models for pain and dystonia severity scores versus neuropsychiatric symptom scale scores across all onset site groups. The relationship of pain and dystonia severity to the severity of neuropsychiatric symptoms across AOFD phenotypes was further investigated using regression type methods and analysis of covariance, correcting for pain severity and dystonia severity (as measured by the GDRS), for continuous outcomes followed by pairwise comparisons among the dystonia onset site groups. SAS software V.9.4 was used for all data analyses. Significance level was defined as a p<0.05.
Results
Participants
Data from a total of 493 AOFD subjects enrolled in the Natural History Project met our initial search criteria, but 15 subjects were excluded due to having more than one region of initial dystonia onset reported, leaving 478 subjects for analyses (table 1). Subjects reporting onset of dystonia in a limb were predominantly affected in their upper limbs (52 of 60 subjects). Data for BDI, HADS-D, HADS-A, LSAS and SF-36 (Pain) rating scales were available for 93% of the subjects, in part, due to exclusion of data from one centre that used an older version of the BDI. There were more women than men in all onset site groups, but no significant difference across the groups (χ2=0.92, p=0.922). Age at onset differed across the groups (F4,123=5.74, p<0.001), with pairwise comparisons showing upper cranial had an older age of onset than cervical (p=0.002) and limb (p=0.005). Total dystonia severity as rated by the GDRS and BFMDRS at the time of enrolment in the Natural History Project (table 1) differed across dystonia onset sites (GDRS: F4,105=5.49, p<0.001; BFMDRS: F4,95=5.70, p<0.001). Pairwise comparisons revealed that upper cranial had higher dystonia severity scores compared with cervical (GDRS, BFMDRS: p=0.002, p=0.003), laryngeal (p=0.004, p=0.001) and limb (p=0.001, p=0.001).
Demographics and rating scale scores
Depression, anxiety and pain by dystonia group
HADS-D (F4,121=3.08, p=0.019), HADS-A (F4,129=3.14, p=0.017) and LSAS (F4,127=4.37, p=0.002) scores differed across AOFD groups, whereas BDI scores did not (F4,111=2.15, p=0.08) (figure 1). Pairwise comparisons revealed higher anxiety (HADS-A scores) in cervical compared with upper cranial (p=0.027) and higher social anxiety (LSAS scores) in laryngeal compared with limb (p=0.001) and to upper cranial (p=0.031). No significant pairwise comparisons were found for HADS-D. Pain varied across dystonia groups (F4,119=13.01, p <0.0001) (table 1). Pairwise comparisons revealed greater pain in cervical compared with laryngeal (p <0.0001), limb (p <0.0001) and upper cranial (p=0.003).
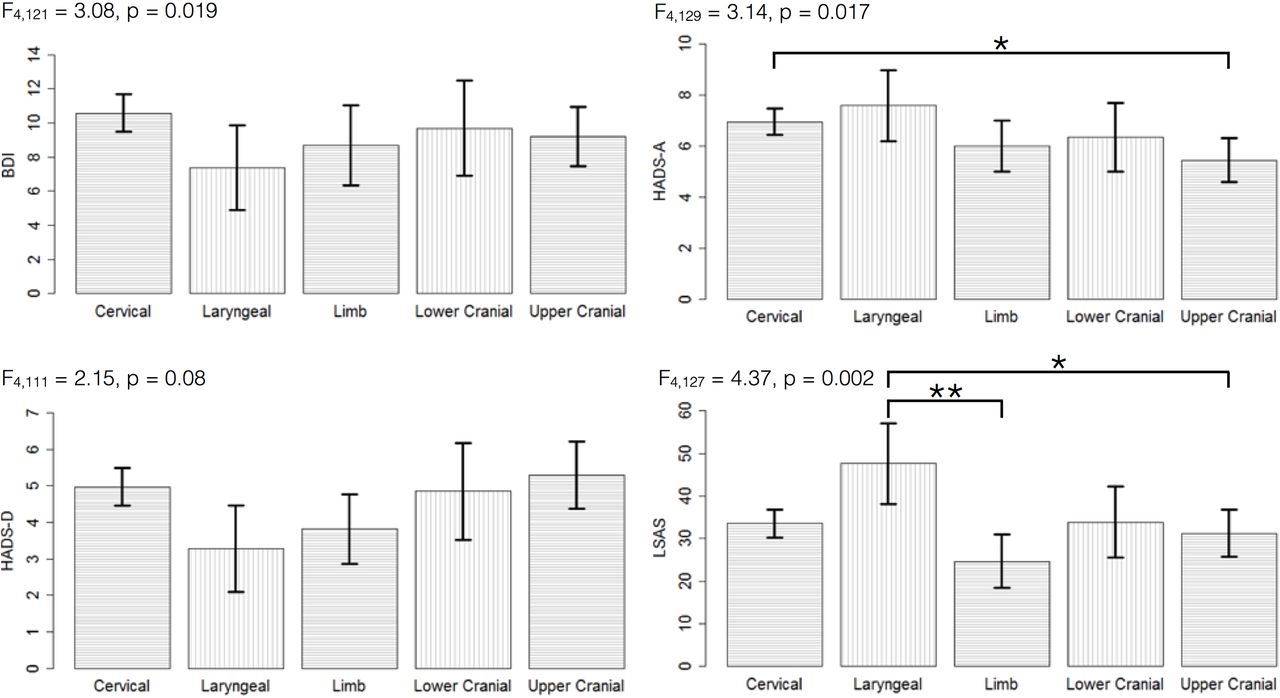
Depression, anxiety and social anxiety by dystonia onset region. Isolated focal dystonia patients were grouped into five regions of dystonia onset and excluded if they reported more than one body part affected at onset. Overall, F tests for group differences are shown for each scale. Significant difference of *p<0.05 or **p<0.005 in pairwise comparisons with Tukey-Kramer adjustments for multiple comparisons. Error bars represent 95% CIs. BDI, Beck Depression Inventory (2nd edition); HADS-D/A, Hospital Anxiety and Depression Scale–Depression/Anxiety; LSAS, Liebowitz Social Anxiety Scale.
Proportion with depression and anxiety by dystonia group
Using the standard neuropsychiatric scale cut-offs defined above, 29.7% of the patients with AOFD had depression by BDI, 22.6% depression by HADS-D, 37.7% anxiety by HADS-A and 45.0% social anxiety by LSAS (table 2). Significant differences across groups were found using the HADS-A (χ2=12.67; p=0.013) and LSAS (χ2=15.63; p=0.004) scales, but not the BDI (χ2=4.50; p=0.342) or HADS-D (χ2=8.86; p=0.065) scales (figure 2). Pairwise comparisons revealed a greater proportion with anxiety (HADS-A scores) in cervical (p=0.002) and laryngeal (p=0.038) compared with upper cranial, and a greater proportion with social anxiety (LSAS scores) in laryngeal compared with all other groups (cervical, p=0.004; limb, p <0.001; lower cranial, p=0.021; upper cranial, p=0.001).

Proportion of depression, anxiety and social anxiety by dystonia onset region. Isolated focal dystonia patients were grouped into five regions of dystonia onset and excluded if they reported more than one body part was affected at time of onset. Significant difference of *p <0.05 or **p <0.005 in pairwise comparisons using two-way χ2 tests or Fisher exact tests. Error bars represent 95% CIs. BDI, Beck Depression Inventory (2nd edition); HADS-D/A, Hospital Anxiety and Depression Scale–Depression/Anxiety; LSAS, Liebowitz Social Anxiety Scale.
Proportion of depression, anxiety and social anxiety by dystonia onset site region
Relationship of pain and dystonia severity to depression and anxiety by dystonia group
Regression analysis revealed significant positive associations for all onset site groups between bodily pain scores and neuropsychiatric symptom scale scores except for BDI (p=0.062) and LSAS (p=0.094) in the laryngeal group (figure 3). Regression analysis also revealed a limited number of significant associations between dystonia severity (GDRS scores) and neuropsychiatric symptom scale scores including positive associations with BDI (p=0.013), HADS-D (p=0.004) and LSAS (p=0.041) in the cervical group, with LSAS (p=0.0002) in the laryngeal group and with BDI (p=0.017), HADS-D (p=0.035) and HADS-A (p=0.016) in the lower cranial group (figure 4).

Relationship of pain with depression, anxiety and social anxiety by dystonia onset region. Isolated focal dystonia patients were grouped into five regions of dystonia onset and excluded if they reported more than one body part was affected at the time of onset. Significance of linear fit regression model is noted as *p<0.05 or **p<0.005. BDI, Beck Depression Inventory (2nd edition); HADS-D/A, Hospital Anxiety and Depression Scale–Depression/Anxiety; LSAS, Liebowitz Social Anxiety Scale; SF-36, 36-Item Short Form Survey.
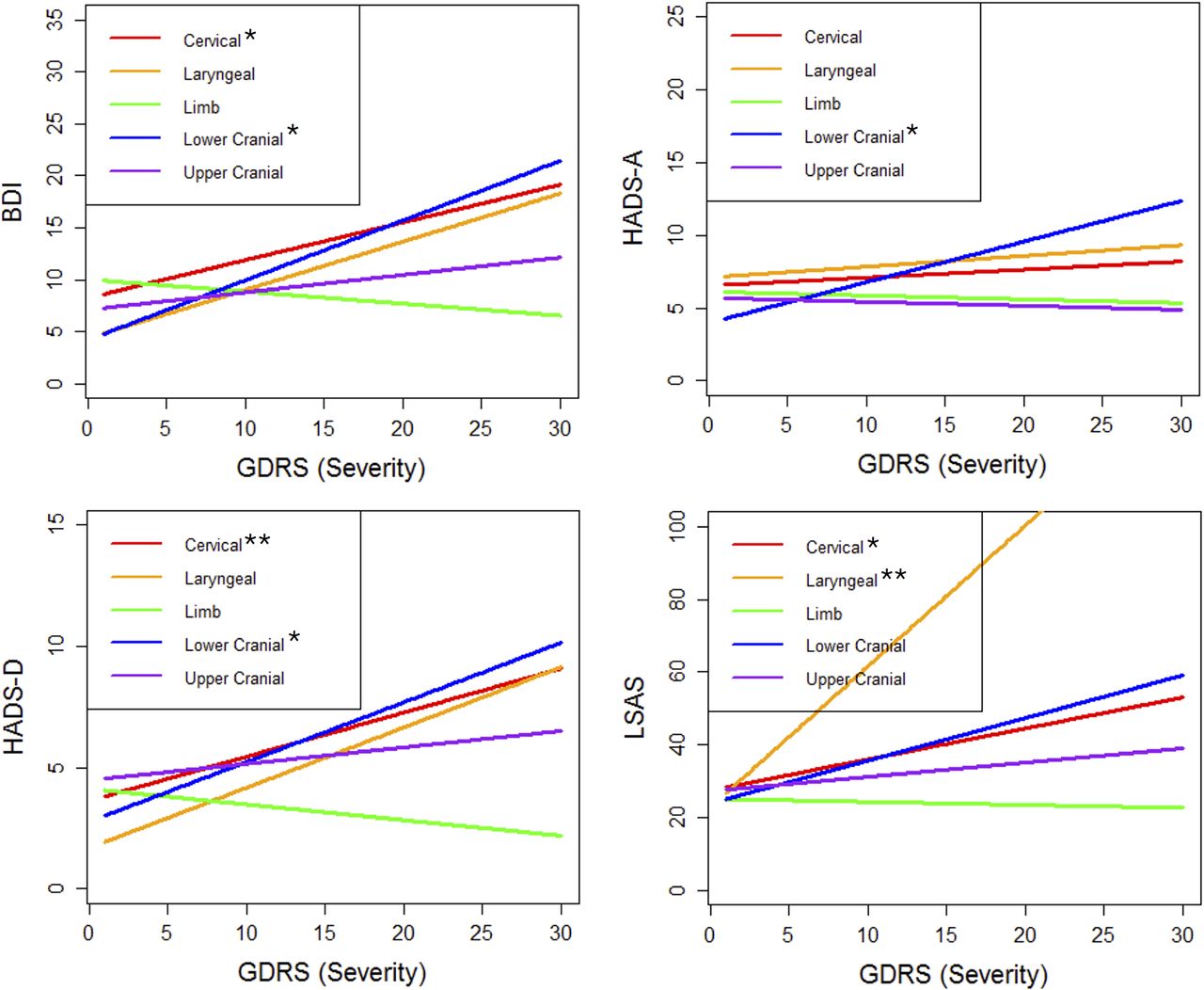
Relationship of dystonia severity with depression, anxiety and social anxiety by dystonia onset region. Isolated focal dystonia patients were grouped into five regions of dystonia onset and excluded if they reported more than one body part was affected at the time of onset. Significance of linear fit regression model is noted as *p<0.05 or **p<0.005. BDI, Beck Depression Inventory (2nd edition); GDRS, Global Dystonia Rating Scale; HADS-D/A, Hospital Anxiety and Depression Scale–Depression/Anxiety; LSAS, Liebowitz Social Anxiety Scale.
No interaction, as tested by comparing whether slopes of best linear fit lines differed between dystonia onset groups, was found between pain scores and neuropsychiatric symptom scale scores by dystonia group (BDI: F4,96.7=1.06, p>0.38; HADS-D: F4,110=0.30, p>0.87; HADS-A: F4,107=2.10, p>0.08; LSAS: F4,89.4=1.36, p>0.25). Similarly, no interaction was found between dystonia severity (GDRS scores) and neuropsychiatric symptom scale scores by dystonia group (BDI: F4,116=1.09, p>0.36; HADS-D: F4,118=1.36, p>0.25; HADS-A: F4,120=1.47, p>0.22). An interaction was found, however, between dystonia severity (GDRS scores) and social anxiety (LSAS) across dystonia groups (F4,125=3.52, p=0.009) with a larger slope observed for laryngeal onset group compared with cervical (p=0.005) and limb (p=0.001) onset groups.
Depression and anxiety by dystonia group after correcting for dystonia severity and pain
When dystonia severity and severity of bodily pain were included as covariates in our general linear model, BDI (F4,111=0.64, p=0.634) and HADS-D (F4,116=1.55, p=0.193) scores did not differ across AOFD groups, whereas HADS-A (F4,123=4.06, p=0.004) and LSAS (F4,130=5.88, p <0.001) scores continued to show significant differences across AOFD groups (figure 5). Pairwise comparisons revealed higher anxiety (HADS-A scores) in laryngeal compared with cervical (p=0.008) and upper cranial (p=0.002), and higher social anxiety (LSAS scores) in laryngeal compared with cervical (p <0.001), limb (p <0.001), lower cranial (p=0.015) and upper cranial (p=0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Depression, anxiety and social anxiety by dystonia onset region after correcting for pain and dystonia severity. Isolated focal dystonia patients were grouped into five regions of dystonia onset and excluded if they reported more than one body part affected at onset. Overall F tests for group differences are shown for each scale. Significant difference of *p <0.05 or **p<0.005 in pairwise comparisons with Tukey-Kramer adjustments for multiple comparisons. Error bars represent 95% CIs. BDI, Beck Depression Inventory (2nd edition); HADS-D/A, Hospital Anxiety and Depression Scale–Depression/Anxiety; LSAS, Liebowitz Social Anxiety Scale.
Discussion
In this large international, multicentre cohort of recently diagnosed patients with AOFD, we found that the severity and relative frequency of anxiety and social anxiety related to the site of dystonia onset. In particular, the cervical and laryngeal onset groups had greater anxiety than the limb and upper and lower cranial onset groups, and the laryngeal onset group had significantly higher social anxiety than those with dystonia that started in all the other body regions. After accounting for bodily pain and dystonia severity, however, the laryngeal onset group was found to have the highest levels of both anxiety and social anxiety. These findings provide new evidence that adult-onset patients affected by idiopathic focal dystonia may have distinct psychopathology depending on the initial body region affected by dystonia.
Our findings support a large and growing body of evidence of the coexistence of depression and anxiety with isolated, idiopathic dystonia.4–7 27 In our AOFD cohort, we found depression proportion rates of 29.1% and 22.6% by BDI and HADS-D, respectively, and an anxiety proportion rate of 37.7% by HADS-A. These relative rates lie within previously reported prevalence ranges of 25% to 50% in patients with dystonia4 5 7 and exceed the background prevalence of 7% for depression and 18% for anxiety of adults in the USA,28 supporting the notion that depression and anxiety frequently accompany AOFD.
High depression rates have been reported in non-focal (eg, segmental and generalised)29 and genetic forms of dystonia,30 as well as in asymptomatic carriers of dystonia-causing gene mutations31 and unaffected family members of those with dystonia.32 In our AOFD cohort, we did find a significant difference in the severity of depression across different onset sites by HADS-D, but after correcting for bodily pain and dystonia severity, this difference disappeared. Furthermore, stricter pairwise testing did not identify significant differences between pairs of onset site groups in either the corrected or uncorrected linear models. Finally, the proportion of patients with depression while high relative to background rates did not significantly differ across the dystonia groups. Taken together, our findings provide additional evidence to prior observations that depression is an inherent feature of isolated dystonia rather than secondary to the motor symptoms.
In our large, recently diagnosed AOFD cohort, we found an overall group difference in HADS-A scores across AOFD phenotypes, with pairwise testing revealing significantly greater anxiety in the cervical and laryngeal onset groups compared with the other onset site groups. One explanation for this finding is that the underlying pathophysiology of these phenotypes differs from the other onset site groups and leads to differences in associated psychopathology. Pathophysiological differences in trigeminal nerve signalling have been reported in patients with isolated focal dystonia,33 and abnormal signalling involving the vagal nerve (superior laryngeal branch) has been reported in laryngeal dystonia.34 As dysfunctional activity of the trigeminal and vagal nerves has been implicated in modulating affective disorders,35 36 differential effects on the signalling of these nerves in the cervical and laryngeal onset groups could contribute to the differences in anxiety observed. It is also possible differing demographic factors contributed to the differences in anxiety across onset site groups. In our cohort of patients with AOFD, however, gender did not differ across dystonia groups and only the upper cranial group was significantly older than the other groups limiting gender and age differences as potential contributors. Another possible explanation for the group differences is that anxiety in AOFD phenotypes is modulated by environmental or sociological factors not assessed or accounted for in our study. For example, the pervasive influence of laryngeal dystonia on basic interpersonal communication may lead to a greater propensity for anxiety. Additional studies are needed to help ascertain the contribution of these types of variables to the manifestation of neuropsychiatric symptoms in patients with AOFD.
Although bodily pain severity positively correlated with the severity of depression, anxiety and social anxiety across all onset site groups, there was no significant interaction found between pain and site of dystonia onset. This finding implies that increasing bodily pain severity has a similar effect on neuropsychiatric scale scores across all AOFD phenotypes. Moreover, although the cervical and laryngeal onset groups had the highest ratings of anxiety, they had divergent levels of reported pain severity with the cervical group having the highest reported pain of all dystonia onset sites and the laryngeal group having the lowest. Thus, after correcting for pain, a relative decrease in anxiety was seen in the cervical group compared with the laryngeal group. These findings suggest that pain, often a troublesome symptom in patients with dystonia, particularly for those with cervical dystonia, is an independent symptom with potentially several pathogenic mechanisms.37
Social phobia, an anxiety disorder characterised by an intense fear in one or more social situations that causes distress and impairs one’s social functioning, is another commonly associated neuropsychiatric symptom in AOFD.26 38 Indeed, the lifetime risk of social phobia is significantly increased in isolated focal dystonias (OR=21.6).12 We found the proportion of AOFD subjects with social anxiety ranged between 31.7% and 72.7% depending on the site of dystonia onset. In a large study of patients with cervical dystonia,39 a high prevalence of social phobia was associated with altered body image and attitudes towards illness but not disease severity. This finding supports that our observed high relative prevalence of social anxiety could stem from a reaction to the motor symptoms rather than a primary feature of dystonia. In our study, high social anxiety in the laryngeal onset group was the main driver of the significant difference found across onset site groups, both with and without correction for bodily pain and dystonia severity. We further found a rapidly increasing positive relationship between severity of dystonia and social anxiety in the laryngeal onset group. Thus, it may be that speech difficulties (eg, reduced intelligibility) in particular lead to secondary stigma and social anxiety. This is further supported by a study comparing patients with laryngeal dystonia to patients with vocal fold paralysis that found no significant difference in social phobia between the two groups.27
Although our study leveraged an international, multicentred database repository and is the largest of its kind, it is nevertheless limited by smaller sample sizes within some of the dystonia groups. Our study also may be weighted towards subjects who were evaluated at specialty tertiary centres and possibly have more severe forms of dystonia or more severe non-motor symptoms associated with their dystonia, potentially limiting the generalisability of our results. In our study, we also restricted our analysis to those with recent onset of dystonia to capture neuropsychiatric symptoms as it relates to the initial body region affected and at a relatively early stage of disease. Future longitudinal studies are needed to evaluate whether a tendency for dystonia to spread to additional body regions, such as recently reported in patients with cervical dystonia,40 influences the presence and severity of neuropsychiatric symptoms. Our study is also limited in that assessments of sleep disturbances along with collection of demographic information such as education level and employment status, factors that can influence the occurrence of neuropsychiatric symptoms,41 42 were not collected and may have confounded our results. Another limitation of our study is the lack of controls. Including healthy controls along with patients with similarly disabling symptoms from non-dystonia diagnoses would have strengthened the ability to determine whether differences in neuropsychiatric symptoms across AOFD phenotypes are secondary to the varying motor manifestations or constitute primary features of particular AOFD phenotypes.
In summary, we found high rates of neuropsychiatric symptoms in recently diagnosed patients with AOFD, and that the severity of depression, anxiety and social anxiety vary by site of dystonia onset. In particular, anxiety was most prominent in those with cervical and laryngeal onset groups, and social anxiety was greatest in those with laryngeal onset. Increasing bodily pain and dystonia severity for the most part correlated with worsening severity of neuropsychiatric symptoms independent of onset region, but pain levels differed by site of dystonia onset in patients with AOFD. After accounting for bodily pain and dystonia severity, no differences in depression severity were found across dystonia onset sites providing further support that depression may be inherent to isolated dystonia regardless of the body region. In contrast, accounting for bodily pain and dystonia severity resulted in an increase in anxiety and social anxiety within the laryngeal onset group, suggesting a potential unique psychopathology in this form of AOFD.
Acknowledgments
This study was supported by a grant from the National Institutes of Health (Dystonia Coalition U54 NS065701). We would like to thank Laura J Wright, MA, for her assistance with accessing the Dystonia Coalition database and Ami R Rosen, MS, for providing organisational support for the Dystonia Coalition.
References
Footnotes
Contributors BDB: Project conception, design, organisation and execution; recruitment and clinical assessment of subjects; statistical analysis design and oversight; manuscript drafting and revision. JJ: Project conception, design and organisation; manuscript review and critique. ES: Recruitment and clinical assessment of subjects. SHS: Statistical analysis design and execution. HAJ, JSP, AJE, JJ, MV, CB, WO, IAM, RR, TB: Recruitment and clinical assessment of subjects; manuscript review and critique. WMM, LM, MZ: Neuropsychiatric scale selection; manuscript review and critique. NB: Project conception, design and organisation; recruitment and clinical assessment of subjects; manuscript review and critique.
Funding This work was supported in part by grants to the Dystonia Coalition (U54NS065701/TR001456), a consortium of the Rare Diseases Clinical Research Network (RDCRN) that is supported by the Office of Rare Diseases Research (ORDR) at the National Center for Advancing Clinical and Translational Studies (NCATS) in collaboration with the National Institute for Neurological Diseases and Stroke (NINDS).
Competing interests None declared.
Patient consent All patients consent with local IRB-approved consent forms.
Ethics approval Internal Review Boards for all participating clinical sites.
Provenance and peer review Not commissioned; externally peer reviewed.