Article Text

Abstract
Objective A reperfusion quality of thrombolysis in cerebral infarction (TICI)≥2b has been set as the therapeutic angiography target for interventions in patients with acute ischaemic stroke. This study addresses whether the distinction between TICI2b and TICI3 reperfusions shows a clinically relevant difference on functional outcome.
Methods A systematic literature review and meta-analysis was carried out and presented in conformity with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria to test the primary hypothesis that TICI2b and TICI3 reperfusions are associated with different rates of modified Rankin Scale (mRS) ≤2 at day 90. Secondary endpoints included rates of haemorrhagic transformations, mortality and excellent functional outcome (mRS ≤1). Summary estimates of ORs (sOR) with 95% CI were calculated using the inverse variance heterogeneity model accounting for multiple true effect sizes.
Results Fourteen studies on 2379 successfully reperfused patients were included (1131 TICI3, 1248 TICI2b). TICI3 reperfusions were associated with higher rates of functional independence (1.74, 95% CI 1.44 to 2.10) and excellent functional outcomes (2.01, 95% CI 1.60 to 2.53), also after including adjusted estimates. The safety profile of patients with TICI3 was superior, as demonstrated by lower rates of mortality (sOR 0.59, 95% CI 0.37 to 0.92) and symptomatic intracranial haemorrhages (sOR 0.42, 95% CI 0.25 to 0.71).
Conclusion TICI3 reperfusions are associated with superior outcome and better safety profiles than TICI2b reperfusions. This effect seems to be independent of time and collaterals. As reperfusion quality is the most important modifiable predictor of patients’ outcome, a more conservative definition of successful therapy and further evaluation of treatment approaches geared towards achieving TICI3 reperfusions are desirable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Quality of reperfusion is one of the most important and potentially modifiable determinants of clinical outcome in patients treated with thrombectomy following acute ischaemic stroke.1 It is commonly evaluated by applying the five-step thrombolysis in cerebral infarction (TICI) grading scale.2 Grades 2b and 3 are routinely termed ‘successful reperfusion’ as this was shown to be the most favourable cut-off for predicting good outcome at 90 days with non-significant differences between grades 2b and 3.3 4 Consequently, the target angiographic endpoint has been set to TICI ≥2b.5 However, differences in outcome between patients with TICI2b and TICI3 reperfusions have mostly been neglected, as they are often subtle or may have simply been overlooked, because both grades have been routinely subsumed under the term ‘successful’. Recently, some studies have suggested superior outcomes for TICI3 versus TICI2b reperfusions, thus putting into question whether the definition of success should be revised.6–8 Due to the relatively small number of patients included, it currently remains unclear whether the distinction between TICI2b and TICI3 is clinically relevant. The primary objective of this analysis was therefore to identify and quantify all available observational data on clinical outcomes between TICI2b and TICI3 reperfusions. Furthermore, we aimed to review and discuss recent refinements and modification of the TICI score.
Methods
The meta-analysis conducted adheres to the reporting guidelines laid down by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses report (PRISMA statement)9 and Meta-analysis of Observational Studies in Epidemiology checklist.10 Several versions of the TICI scale exist and are referred to as original, modified or extended TICI scale (abbreviated as oTICI, mTICI and eTICI, respectively, see online supplementary table I). To avoid confusion, oTICI grade 2b is defined as antegrade reperfusion of at least two-thirds of the target territory.2 mTICI grade 2b refers to antegrade reperfusion of at least half of the target territory.5 Grade 2b in mTICI and eTICI is the same, but an additional TICI2c grade has been employed in eTICI referring to ‘near complete perfusion except for slow flow in a few distal cortical vessels, or presence of small distal cortical emboli’.11 12 Lastly, Liebeskind et al recently suggested the oTICI2c scale which subdivides the grade 2b into 2b with 50%–66% reperfusion and 2b with 67%–90% reperfusion. Here, reperfusion of 90%–99% is referred to as grade 2c13 (see online supplementary table I).
Supplementary file 1
Literature search and data extraction
PubMed and Web of Science databases (from inception to 18 October 2017) were accessed using a predefined search strategy formulated according to the Population, Intervention, Comparison and Outcome (PICO) format (see online supplementary tables II and III).14 Full-text articles and conference abstracts were reviewed. No language restriction was applied. Eligibility of the studies for the quantitative analysis was rated by two independent readers (JK and TD). Studies were included into the quantitative synopsis if the study reported on (1) the primary outcome stratified according to TICI2b versus TICI3 reperfusions or (2) the primary outcome stratified according to TICI2b versus TICI2c/3 reperfusions. Manual searching of reference lists of the included studies was coupled with a search of all articles citing the included articles using Google Scholar metadata (https://scholar.google.ch/). If available, TICI2c was pooled together with TICI3, as preliminary evidence has suggested that both are associated with a comparable clinical course.15–17 In a sensitivity analysis, comparisons of TICI2c/3 and TICI2b were excluded leading to a comparison confined to mTICI2b versus mTICI3 in order to rule out the possibility that potential differences are only discernible when applying the more detailed eTICI scale. Studies that did not meet the eligibility criteria but appraised the topic of outcome differences between TICI2b and TICI3 reperfusions were included into further semiquantitative or qualitative analyses.
Primary outcome was the rate of patients achieving functional independence at day 90, defined as modified Rankin Scale (mRS) ≤2. Predefined secondary outcomes were excellent functional outcome (mRS ≤1), mRS shift, all-cause mortality (during hospitalisation or day 90, depending on the reporting standards), final infarct volume, rates of symptomatic intracranial haemorrhage (sICH) and rates of any intracranial haemorrhage (any ICH). If a study did not report on a clinical definition of sICH, rates of parenchymal haematomas (PH1/2 or PH2 only, depending on the way of reporting) were evaluated as radiological surrogate, according to the European Acute Stroke Study definiton.18
If available, the following parameters were extracted and calculated: type of study, unadjusted odds for the primary and secondary outcomes, results from adjusted analyses with a description of parameters adjusted for, type of TICI scale applied and presence of differences in baseline characteristics. Two independent raters extracted the data (JK and MRH). All extracted raw frequency counts can be found in the online supplementary dataset 1.
Supplementary file 2
Statistical analysis
The inverse variance heterogeneity model was used to calculate summary estimates of effect sizes (summarised ORs, sOR),19 since included studies used different inclusion and exclusion criteria and require to account for multiple true effect sizes. To calculate unadjusted ORs, the prevalence of different endpoints was extracted from the published data for each arm. Summarised point estimates are displayed together with 95% CIs to express the odds for a comparison between TICI3 and TICI2b. Adjusted ORs were summarised separately, if available. Heterogeneity was explored using Cochrane’s Q and I².20 Visual inspection of funnel plots and Doi plots and calculation of the Luis Furuya-Kanamori (LFK) index were used for the evaluation of publication bias regarding the primary endpoint.21 Data analysis was performed using the software package MetaXL (EpiGear International, Sunrise Beach, Queensland, Australia) for Microsoft Excel.
Risk of bias and quality assessment
The risk of bias was evaluated as per Cochrane Collaboration tool.22 Additionally, the following quality criteria were specifically evaluated: (1) specification of inclusion criteria; (2) comprehensive reporting of baseline characteristics; (3) availability of adjusted analyses; and (4) core lab adjudicated reperfusion grading. Both ratings were performed independently by two readers. In cases of discrepancies a consensus was reached (n=6/126 items).
Results
Quantitative analyses
Fourteen studies with a total of 2379 successfully reperfused patients (1131 TICI3, 1248 TICI2b) with available follow-up were included in the quantitative analysis (see figure 1 for PRISMA flow chart).3 7 13 16 17 23–31 During the eligibility rating process, five discrepancies arose, which could be resolved by a third rater (see online supplementary table IV). Three conference abstracts13 27 31 and 11 research articles met the inclusion criteria. Eleven of the 14 studies were retrospective observational studies. One study examined different degrees of successful reperfusion in the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials collaboration of recent endovascular trials.13 Eleven studies provided comparisons of mTICI2b and mTICI3, one study reported a comparison of mTICI2b and mTICI3 together with mTICI2b and mTICI2c/3,17 one compared mTICI2b with mTICI2c/3,16 and one study provided comparison of TICI2b and TICI2c/3 using the TICI scale revised by Liebeskind et al.13 The reporting frequencies and respective patient numbers for the primary and secondary endpoints can be found in online supplementary table V. An overview of characteristics of the included studies can be found in table 1 and online supplementary table VI). The most frequently observed differences between patients with TICI2c/3 and TICI2b reperfusions were shorter onset to reperfusion metrics and better collaterals in the TICI2c/3 group (see table 1). No differences regarding the rates of preinterventional intravenous tissue plasminogen activator (tPA) administration between both groups were reported (see online supplementary table VI).

Flow chart according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. mRS, modified Rankin Scale; TICI, thrombolysis in cerebral infarction.
Characteristics of studies included into quantitative analysis
TICI2c/3 reperfusion was more frequently associated with functional independence at day 90 than TICI2b (sOR 1.74, 95% CI 1.44 to 2.10, figure 2), without substantial heterogeneity (I² 13%, Q=15.00, P=0.31). This association remained statistically tangible if analysis was confined to studies that used the mTICI scale (mTICI3 vs mTICI2b, sOR 1.82, 95% CI 1.41 to 2.34, online supplementary figure I). Importantly, this association also reached statistical significance after summarising the adjusted ORs of the respective studies (adjusted sOR 2.36, 95% CI 1.69 to 3.30, online supplementary figure II). The overall event rate of mRS ≤2 calculated from the studies reviewed was ~55%. Assuming this as a reference level, achieving TICI3 instead of TICI2b in five cases, would result in one additional patient reaching functional independence according to the adjusted estimates. Furthermore, excellent functional outcomes were more commonly observed in patients with TICI2c/3 reperfusions (unadjusted sOR 2.01, 95% CI 1.60 to 2.53, adjusted sOR 2.70, 95% CI 1.71 to 4.25, figure 3 and online supplementary figure III, respectively). This was also the case when analysis was limited to studies using the mTICI scale (mTICI3 vs mTICI2b, sOR 2.27, 95% CI 1.67 to 3.08, online supplementary figure IV).

Summary OR TICI2c/3 versus TICI2b for d90 modified Rankin Scale (mRS) ≤2. *Used extended TICI (eTICI) scale with TICI2c; TICI2c and TICI3 were subsumed under TICI3; for grading used in Liebeskind et al see online supplementary table I. TICI, thrombolysis in cerebral infarction.

Summary OR TICI2c/3 versus TICI2b for d90 modified Rankin Scale (mRS) ≤1. *Used extended TICI (eTICI) scale with TICI2c; TICI2c and TICI3 were subsumed under TICI3; for grading used in Liebeskind et al see online supplementary table I. TICI, thrombolysis in cerebral infarction.
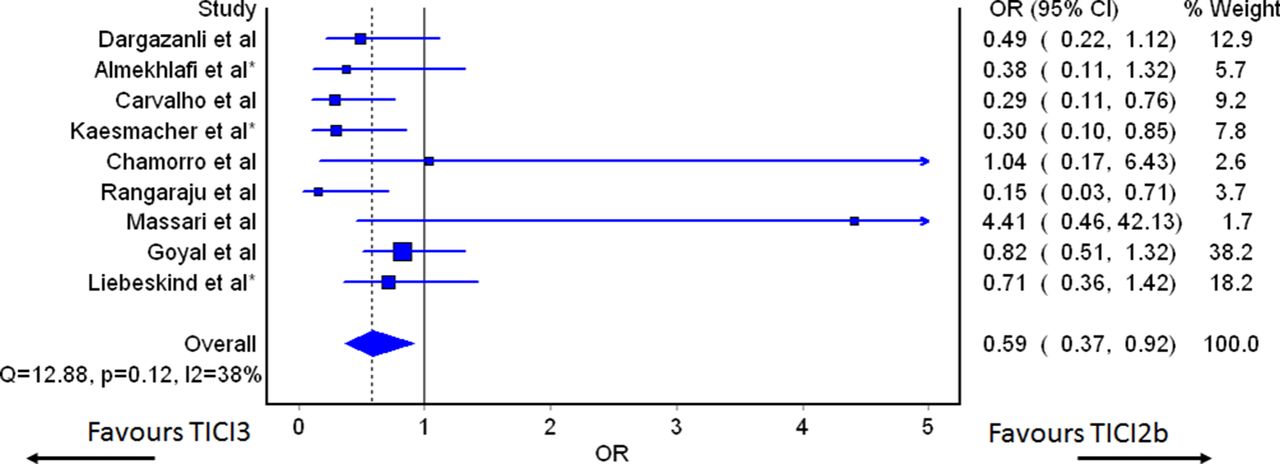
TICI2c/3 reperfusion was associated with reduced haemorrhagic transformations (sOR 0.48, 95% CI 0.26 to 0.90 for any ICH, figure 4A), including symptomatic ICH (sOR 0.42, 95% CI 0.25 to 0.71, figure 4B, adjusted sOR 0.23, 95% CI 0.11 to 0.48, available in two studies). Correspondingly, there was reduced outcome fatality in patients in whom TICI2c/3 reperfusion was achieved (sOR 0.59, 95% CI 0.37 to 0.92, see figure 5). All of the above-mentioned associations were also present in an analysis confined to studies applying mTICI (mTICI3 vs mTICI2b, data not shown).

Summary OR TICI2c/3 versus TICI2b for any intracranial haemorrhage (ICH) and symptomatic intracranial haemorrhage (sICH). (A) Any type of ICH. (B) Symptomatic ICH. §Parenchymal haematomas (PH1/2) defined as sICH. *Used extended TICI (eTICI) scale with TICI2c; TICI2c and TICI3 were subsumed under TICI3. TICI, thrombolysis in cerebral infarction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary OR TICI2c/3 versus TICI2b for mortality. *Used extended TICI (eTICI) scale with TICI2c; TICI2c and TICI3 were subsumed under TICI3; for grading used in Liebeskind et al see online supplementary table I. TICI, thrombolysis in cerebral infarction.
No asymmetry was noted for the analyses concerning the rates of functional independence at day 90, as revealed by funnel and Doi plot inspection (online supplementary figure V). The LFK index was indicative of no asymmetry (0.98).
Due to the nature of the topic under review, no study with random sequence allocation was available. A substantial risk of bias was observed in most studies, however, the most common being incomplete outcome data, selective reporting and blinding of participants and personnel (online supplementary table VII). The most common features reducing the quality of the respective studies were lack of core lab adjudicated reperfusion grading and lack of reporting on adjusted analyses (online supplementary table VII).
Further semiquantitative and qualitative synopsis
One study provided a comparison of oTICI2b and oTICI3 patients but was not included because of a significant overlap of the study cohort with another analysis.6 16 This article remains of interest, however, as it uses the more conservative oTICI scale in its definition of grade 2b. Nonetheless, a significant outcome difference was present, suggesting that the outcome discrepancies recognised in the above outlined meta-analysis are also present when applying the strictest scale.
A recent observational study failed to prove the existence of significant outcome differences among TICI3 and TICI2b patients when applying the oTICI or mTICI scale, although a clear trend was recognisable.15 However, significant differences between TICI2c/3 and TICI2b were noted if the eTICI scale was applied. The study was excluded from quantitative analyses because no dichotomised mRS values were provided.15
One study included in the quantitative analysis group did not disclose an adjusted analysis for dichotomised analysis, although an ordinal regression analysis was performed. After correction for age, sex, pretreatment National Institutes of Health Stroke Scale score, target occlusion, infarct core and pretreatment alteplase, TICI3 was independently associated with a favourable mRS shift at day 90.23
Two of the included studies also provided analyses of tissue outcomes. Rangaraju et al 27 reported a significant reduction in final infarct volume in patients achieving TICI3 as compared with TICI2b reperfusion (6.2cc vs 22.5cc, P=0.007). Corroborating this finding, Chamorro et al reported smaller final infarct volumes and reduced infarct growth in patients with TICI3 reperfusions. Importantly, this association remained statistically tangible after the correction for covariates, including infarct core on CT perfusion.23
Discussion
The study-level meta-analysis incorporating data from 2379 patients provides further evidence that the outcome of patients with TICI3 reperfusion is superior to that of patients in whom TICI2b reperfusion is achieved. This discrepancy was evident from multiple endpoints and even more pronounced when analyses were restricted to adjusted estimates. The observed effect remains significant irrespective which TICI score is applied. Logically, the better the TICI score, the more tissue is reperfused, and the smaller the chance for the penumbra to evolve into infarct.32 33 However, the present analysis has substantiated that this specifically holds true also for different degrees of successful reperfusion (ie, TICI2b vs TICI3). This implies that TICI3 should be reported separately from TICI2b reperfusion in all future studies and calls into question whether the definition of successful reperfusion should be refined.6 25
Various versions of TICI scales already exist.34 35 So far, the three most commonly used are the oTICI,2 the mTICI5 and the eTICI with the implementation of grade TICI2c.11 12 All of these scales have an acceptable inter-rater reliability.15 36 37 The TICI2c score was first mentioned by Noser et al 11 and later revisited by Goyal et al.12 Its primary intention was to better characterise and subcategorise successful reperfusion. So far, substantial evidence suggests that patients with a TICI2c reperfusion follow the same clinical course as TICI3 patients.15–17 Some TICI2c reperfusions would be classified as TICI2b according to the mTICI and oTICI systems.15 17 The eTICI systems therefore appear to be the best biomarker scale to predict patient outcome more accurately.15 17 Furthermore, the clinical impact of TICI2b might be influenced by the eloquence of the non-reperfused area, a factor currently neglected. Distinguishing eloquent (TICI2bE) from non-eloquent (TICI2bNE) reperfusion might have added value but may also add unnecessary complexity to the scale.
Numerous reasons for successful but incomplete reperfusion are conceivable. The most common reason is probably iatrogenic distal embolisation during the thrombectomy manoeuver, since preinterventional thrombus fragmentation with multiple emboli prior to thrombectomy is only rarely observed.38 Another explanation could be microcirculatory failure due to vascular dysregulation or progressive oedema.39 Another aspect to consider is that full parenchymal reperfusion may occur retrogradely via well-developed pial collaterals, despite some very distal emboli impeding antegrade flow, corresponding to the definition of eTICI2c, a functional equivalent of TICI3. Numerous studies reported that good collaterals favour excellent angiographic results.7 40–42 However, the impact of TICI3 reperfusion on outcome seems to be independent of good collaterals and independent of time until reperfusion is achieved (cf adjusted estimates). Recent evidence from a large registry supports the notion that the advancement in technical equipment and operators’ experience results in increasing rates of TICI3 reperfusions.43 Increasing rates of TICI3 result from protection devices and techniques preventing distal embolisation, or due to the operators’ dedication to treat remaining distal emboli.6 A recent meta-analysis has shown that balloon guiding catheters (BGC) increase good angiographic outcomes.44 Moreover, there are emerging techniques combining BGC and distal aspiration with stent retrievers or stent retriever-assisted vacuum-locked extraction of clots aimed at achieving maximum protection.45 46 Given these results, it seems reasonable that technical efforts should be maximised to reduce the risks of periprocedural thrombus fragmentation. However, a well-balanced consideration of risks associated with these techniques should be made.
We have not found evidence that pretreatment with intravenous tPA favours achieving TICI3 instead of TICI2b reperfusion, as no differences in the rates of intravenous tPA administration between TICI2b and TICI2c/3 patients were observed. Results from an animal study have suggested a benefit of intravenous tPA in reducing downstream microvascular thrombosis during large vessel recanalisation.47 However, equal rates of TICI3 reperfusions between patients treated with direct mechanical thrombectomy and bridging have been reported in recent observational studies.48–50 Results from currently enrolling randomised controlled trials evaluating direct mechanical thrombectomy versus bridging (SWIFT-DIRECT, NCT03192332 and MR CLEAN-NO IV, ISRCTN80619088) will provide further high-quality evidence regarding the potential value of intravenous tPA regarding this issue.
Additionally, we cannot give a general recommendation to treat vascular occlusions causing TICI2b rather than TICI3 reperfusions only because TICI3 reperfusions are associated with better outcomes. Although a recent publication has addressed the technical feasibility and safety of manoeuvres aiming to improve TICI2b reperfusions to TICI3 reperfusions,16 this topic deserves further evaluation in a prospective design. In summary, the future direction of research should aim at evaluating strategies to increase the rate of TICI3 reperfusion, the ultimate angiographic benchmark of best clinical success and outcome.
Strengths and limitations
So far, this is the largest pooled patient sample comparing the clinical outcome of patients with TICI2b and TICI3 reperfusions. However, this analysis has several limitations, mostly reflecting the limitations of the included studies. Most of these studies were retrospective observational analyses, giving them scope for selection, publication and detection bias. Furthermore, most reperfusion statuses were not core lab adjudicated, nor was the clinical endpoint assessment blinded. Additionally, outcome differences between TICI2b and TICI3 depend on the inclusion and exclusion criteria applied at each site. Although we tried to account for this heterogeneity using a more conservative statistical approach, we cannot exclude that this affected our analyses. Further evaluation derived from large registries may ultimately clarify whether core lab evaluated TICI3 vs TICI2b reperfusion is as clinically relevant as it appears on outcome and independent of potential covariates.
Conclusion
Without considerable heterogeneity and across a wide range of clinical and biomarker endpoints analysed, TICI3 reperfusion is associated with superior outcome and safety compared with TICI2b. This effect seems to be independent of potential confounders (eg, time to reperfusion, collaterals). Data regarding the interaction and interdependence of these factors, however, are sparse. As reperfusion quality is the most important modifiable predictor of patient outcome, a more conservative definition of therapy success and further evaluation of treatment approaches geared towards achieving TICI3 reperfusions by preventing or treating distal emboli more efficiently are warranted.
Acknowledgments
We thank Susan Kaplan for the writing assistance and language editing.
References
Footnotes
JG and UF contributed equally.
Contributors Study design: JK, JG, UF. Study supervision: UF, JG. Statistical analysis: JK. Initial draft: JK. Revision of the draft for important intellectual content: all authors. Intrepretation of results: all authors. Eligibility rating and quality assessment: JK, TD, MRH. Extraction of raw frequency counts: JK, MRH.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Unrelated: JG is a global PI of STAR, CEC member of the PROMISE study (Penumbra), Consultancy; is the global PI for the SWIFT DIRECT study (Medtronic), Consultancy; and receives SNSF grants for magnetic resonance imaging in stroke. UF is the global PI for the SWIFT DIRECT study (Medtronic), Consultancy, and receives research grants from the Swiss National Science Foundation (SNSF). All other authors have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available within the respective analyses included into this meta-analysis. Extracted raw frequencies are available in the online supplementary dataset 1.