Article Text

Abstract
Background Middle-age risk scores predict cognitive impairment, but it is not known if these associations are evident when controlling for shared genetic and environmental factors. Using two risk scores, self-report educational-occupational score and Cardiovascular Risk Factors, Aging and Dementia (CAIDE), we investigated if twins with higher middle-age dementia risk have poorer old-age cognition compared with their co-twins with lower risk.
Methods We used a population-based older Finnish Twin Cohort study with middle-age questionnaire data (n=15 169, mean age=52.0 years, SD=11.8) and old-age cognition measured via telephone interview (mean age=74.1, SD=4.1, n=4302). Between-family and within-family linear regression analyses were performed.
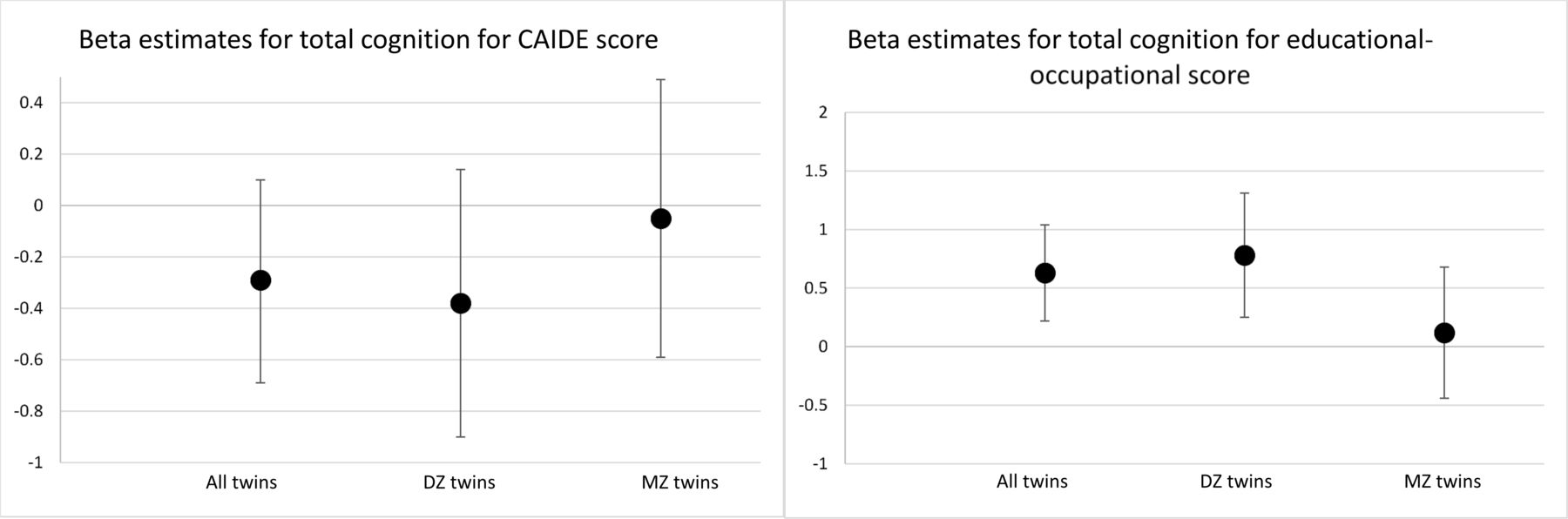
Results In between-family analyses (N=2359), higher educational-occupational score was related to better cognition (B=0.76, 95% CI 0.69 to 0.83) and higher CAIDE score was associated with poorer cognition (B=−0.73, 95% CI −0.82 to -0.65). Within twin-pair differences in educational-occupational score were significantly related to within twin-pair differences in cognition in dizygotic (DZ) pairs (B=0.78, 95% CI 0.25 to 1.31; N=338) but not in monozygotic (MZ) pairs (B=0.12, 95% CI −0.44 to 0.68; N=221). Within twin-pair differences in CAIDE score were not related to within twin-pair differences in cognition: DZ B=−0.38 (95% CI −0.90 to 0.14, N=343) and MZ B=−0.05 (95% CI −0.59 to 0.49; N=226).
Conclusion Middle-age dementia risk scores predicted old-age cognition, but within twin-pair analyses gave little support for associations independent of shared environmental and genetic factors. Understanding genetic underpinnings of risk score−cognition associations is important for early detection of dementia and designing intervention trials.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Dementia is a major challenge for healthcare and society. Currently, there is no treatment to stop or revert Alzheimer’s disease (AD) or similar disorders leading to old-age dementia. Multi-domain lifestyle interventions may, however, delay the onset of dementias.1 Early detection of high-risk individuals may be useful in targeting multi-domain lifestyle interventions and finding disease-modifying drugs for preclinical AD, and it is important because AD process starts 20–30 years prior to diagnosis.2 Risk scores can predict dementia in late life, but few midlife dementia risk scores exist. Only the Cardiovascular Risk Factors, Aging and Dementia (CAIDE) risk score3 of these has been externally validated.4–7
Between-family associations in samples of unrelated individuals can support the utility of the risk scores in detection of high-risk individuals, but they cannot tell if these associations are evident when controlling for shared genetic and environmental influences. Ideally, one would randomise people into high-risk versus low-risk groups, but this is not possible in practice. The closest to experimental design in humans is the use of within-family design comparing relatives, ideally siblings with different levels of risk factors.
Monozygotic (MZ) twins are genetically identical whereas dizygotic (DZ) twins, like non-twin siblings, share on average 50% of their segregating genes. Although MZ twins resemble each other more than DZ twins with regard to dementia, cognition and lifestyle factors such as educational attainment and cardiovascular risk factors,8 even MZ twins in a pair can differ in any of these factors. Quasi-experimental twin design tests if within twin-pair differences in risk factors are related to within twin-pair differences in cognition by controlling for shared environmental (both in DZs and MZs) and genetic influences (fully in MZs and partly in DZs). Compared with studies of unrelated individuals, this design provides more robust evidence regarding genetic and environmental underpinnings of risk factor−cognition associations. Evidence for an association independent of shared genetic and environmental factors is supported when the individual-level (between-family) associations are evident also in within-family comparisons of both DZ and MZ twin pairs.9 In these analyses, shared environmental effects refer to all environmental effects that make MZ or DZ twins within a pair similar. If the associations in DZ or MZ twin pairs are similar in magnitude but non-significant, then these associations are driven by shared environmental effects. If the associations are evident in DZs but not in MZs, then the relationship between risk factors and cognition is confounded by shared genetic effects. Partial genetic confounding occurs when the within-family associations are significant but smaller than between-family associations and MZ within twin-pair associations are about half of the DZ within twin-pair associations. In general, smaller within MZ than DZ pair associations are suggestive of genetic confounding (ie, controlling for greater genetic similarity yields weaker association between risk factors and cognition).
In this study, we used a population-based longitudinal older Finnish Twin Cohort (FTC) study to investigate both between-family and within-family associations of two middle-age dementia risk scores—educational-occupational score10 and CAIDE3—with old-age cognitive functioning. Educational-occupational score was created in the FTC (no within-family analyses).10 An earlier study from the FTC found that self-report measure−based CAIDE score had c-statistics of 0.747 which is comparable with original CAIDE score.3 Virta et al7 used also quasi-experimental twin design to study individual CAIDE factors (obesity, hypertension, hypercholesterolemia and physical inactivity) in relation to cognitive status (cognitively healthy vs impaired), but none of the associations were statistically significant in 54–67 twin pairs clearly discordant for cognitive function (TELE telephone cognition interview score either <16 or >17.5). The current study goes beyond Virta et al’s study7 in three important ways. First, we have a larger sample size allowing to study separately MZ and DZ pairs. Second, we studied the association of CAIDE score rather than individual factors with old-age cognition in within twin-pair analyses. Third, we used a continuous outcome measure.
The aim of the current study was to investigate if middle-age risk scores are associated with cognitive function in old age by conducting between-family and within-family analyses. The hypothesis was that co-twins with higher middle-age dementia risk have poorer old-age cognition compared with their co-twins with lower middle-age dementia risk.
Methods
Participants
We used a population-based longitudinal FTC study comprising all Finnish same-sex twins born before 1958 with both co-twins alive in 1967.8 Questionnaire data were collected in 1975 and 1981 (all cohorts) and in 1990 (those born 1930 or later). The participation rates were 89%, 84% and 77%, respectively.8 Those who were at least 65 years were invited to participate in a telephone interview for screening of cognition in two waves: in 1999–2007 (twins born in 1937 or earlier) and in 2013–2017 (cohorts 1938–1944) with a participation rate of 67%.8 DNA-based zygosity was available for 67% (483 full twin pairs) and 61% (1001 full twin pairs) of participants with CAIDE and educational-occupational score, respectively. For the rest of the participants, zygosity was determined in 1975 with a validated questionnaire with accuracy of over 90%.11
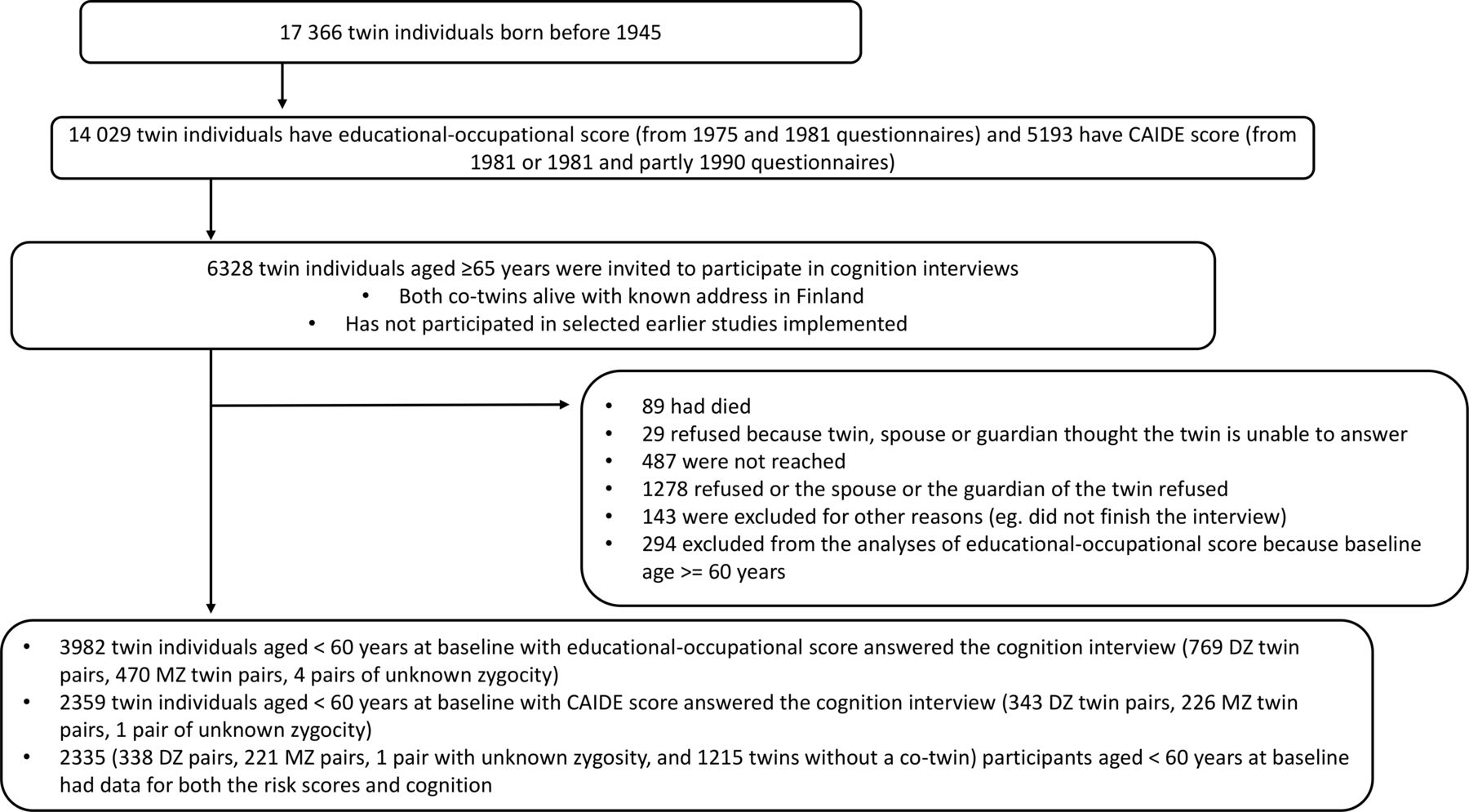
A total of 15 169 twins participated in 1975 and/or 1981. Of these, 14 029 had data to calculate educational-occupational score and a total of 5193 participants (37–59 years old at baseline) had middle-age data on factors included in the CAIDE score (figure 1). Of these, 3982 and 2359 had cognitive data for educational-occupational and CAIDE score analyses, respectively. Finally, 2335 participants had data for both risk scores and cognition (figure 1).

Flowchart of the study. DZ, dizygotic; MZ, monozygotic.
The FTC study has been conducted according to the Declaration of Helsinki. Returning questionnaire was considered as consent to participate. Questionnaire study was approved by the National Board of Health. The study participants have been repeatedly informed about the study and they have been able to withdraw from it. The participants of the telephone interview gave informed consent. Telephone interview protocol was approved by the Ethical Committee of Hospital District of Southwest Finland.
Middle-age dementia risk scores
CAIDE score
We calculated CAIDE score based on self-report measures. The highest self-reported education (“Which schools and classes you have attended?”) in 1975 or 1981 was used and transformed into years of education12 (table 1). Participants were categorised as having hypertension in 1981 (or in 1975 if missing information in 1981) if they reported elevated or slightly elevated blood pressure as measured by a healthcare professional during the last 5 years (5 years was the exact phrasing in these questions in 1981 and 1975). Body mass index (BMI, weight/height-squared) was calculated from self-reported weight and height in 1975 and 1981. Self-reported weight and height are highly correlated with measured height and weight,13 and we used a mean BMI of 1975 and 1981 or only single time point in case of missing data. Obesity was defined as BMI ≥30 kg/m2. Hypercholesterolemia in 1981 was based on elevated self-reported cholesterol levels. If the cholesterol data from 1981 was missing, the information from 1990 questionnaire (available for those born in 1930 or later) was used. Cholesterol values from 1990 were divided according to even numbers and we used value of at least 6.0 mmol/L as the threshold for elevated total cholesterol (6.5 mmol/L in the original CAIDE score). Physical activity information was based on 1981 data but if missing, we used the information from 1975 questionnaire. Participants exercising at least six times per month with a mean duration of at last 30 min with intensity corresponding at least vigorous walking were categorised as ‘active’ and others were classified as physically inactive.7
Additional covariates
The presence of doctor-diagnosed diabetes was queried both in 1975 and in 1981 and having diabetes was based on self-reported diabetes in either year. Smoking status in 1981 (or in 1975 if missing data in 1981) based on a detailed set of questions was classified as having never smoked or being an occasional smoker, former smoker or current smoker.14 Depressive symptoms were measured with Center for Epidemiologic Studies Depression Scale (CES‐D)15 at the time of the telephone interview in those born in 1938–1944 (total score ranges from 0 to 60 with higher scores indicating more depressive symptoms). Five persons who had four or more missing items in CES-D were excluded.
Educational-occupational score
The variables included in the educational-occupational score were self-reported age, years of education, work status, complexity of work, physical loading of work and work environment (table 1). As in the CAIDE score categorisation, education was the highest years of education either from the 1975 or 1981 questionnaire. Work status, complexity of work, physical loading of work and work environment were available both in 1975 and 1981 questionnaires and were categorised as presented in table 1. In order to match the answering age of these variable to CAIDE variables, we used data from 1981 but if missing, data from 1975 were used.
Telephone assessment of cognition at follow-up
Telephone interview consisted of two validated instruments: Telephone assessment of dementia (TELE)16 and Telephone Interview of Cognitive Status (TICS)17 (Finnish versions in18). In this study, we used a continuous score of all TELE and TICS item taking into account overlapping items, total score of cognition (referred in this article as ‘cognition’ with a possible range from 0 to 51).10 We also used a categorical dementia definition with scores of both <16 in TELE and <22.5 in TICS indicating dementia.10
Statistical analyses
We used linear regression analysis to evaluate the relationship between risk scores and cognition. A robust cluster variance estimator was used to adjust standard errors and p values for the dependence of observations in twin data.19 The results are reported in beta estimates and 95% CIs. The length of the follow-up was used as a covariate. In the analyses of CAIDE risk score, the follow-up started from the baseline year 1981 or from 1990 for those who had not answered the cholesterol question in 1981 (44.2% of the participants). In the analyses of educational-occupational score, the follow-up began primarily from 1981 but from 1975 for those who had not answered the questionnaire in 1981 (8.5% of the participants). Models were run with and without age. CES-D was used as a covariate. In CAIDE analyses, diabetes and smoking were used as additional covariates and we also used CAIDE score without education. For educational-occupational score, CAIDE score without education was used as additional covariate.
In within twin-pair analyses, we used a fixed-effect linear conditional regression analysis. Here, the model was ran by regressing the within twin-pair differences in the risk score on the within twin-pair differences in cognition.20
With regard to educational-occupational score, we ran models with all available data (N=3982) and then in those with available CAIDE score (N=2335). CAIDE score analyses were ran with all available data (N=2359) and also by restricting analyses to those with a follow-up time comparable with educational-occupational score, that is, at least 16.5 years of follow-up to minimise the possibility of reverse causation (N=1957). Post hoc analyses included only pairs with DNA-based zygosity.
Results
Demographics
The participants had a mean age of 49.1 (SD=5.9) years at the baseline (table 2). They had on average 8.0 (SD=2.9) years of education, 25.9% had elevated blood pressure and 31.1% had elevated cholesterol level; 3.9% were unemployed or on pension. The mean follow-up time was 23.8 years (SD=6.3, range 8.5–35.7) for CAIDE score and 28.0 years (SD=5.8, range 16.5–41.6) for educational-occupational score. The mean cognition score was 40.6 (SD=4.9) and there were 89 persons (3.8%) with dementia.
Baseline characteristics of the participants with available middle-age CAIDE score and educational-occupational score*
Drop-out analyses
Twins who had cholesterol information (N=2359) had better cognition compared with those who had no cholesterol information (N=1632) with mean cognition scores of 40.6 (SD=4.9) and 39.5 (SD=5.5), respectively (p<0.001). Compared with those who participated in the telephone interview, those who did not participate in the telephone interview were younger, less educated, less often working or studying and their work was more physical (table 2).
Between-family analyses
In individual-level analyses, higher middle-age educational-occupational score was associated with better old-age cognition and higher CAIDE score was associated with poorer old-age cognition (tables 3 and 4, figure 2). Adjusting for depressive symptoms reduced the beta estimates, but the risk score−cognition associations were still statistically significant. The results with both risk scores were similar when adjusting for age and sex ((online supplemental table 1). Educational-occupational score without age (age as a covariate) was statistically significant predictor of cognition (B=0.75, 95% CI 0.68 to 0.82). Similarly, CAIDE score without age (age as a covariate) was statistically significant predictor of cognition (B=−0.78, 95% CI −0.87 to -0.69).
Supplemental material

{kind=link}
{kind=link}
Results from within-pair linear regression analysis between midlife dementia risk scores (CAIDE score and educational-occupational score) and total cognition on average 26 years later for all twins, dizygotic (DZ) twins and monozygotic (MZ) twins. Error bars signify CIs. Higher CAIDE score is associated with poorer cognition and higher educational-occupational score is associated with better cognition.
Results from linear regression analysis between educational-occupational score and total cognition on average 28.0 years later*
Results from linear regression analysis between CAIDE score and total cognition on average 23.8 years later*
Association between educational-occupational score and cognition remained similar after adjustment for CAIDE score without education (table 3). Association between CAIDE score and cognition remained similar after adjustment for education (online supplemental table 1). Diabetes or smoking were not associated with cognition over and above CAIDE score (table 4). The results were similar if only twins with co-twins were included (online supplemental table 1).
Within-family analyses
In within-family analyses, co-twins with higher educational-occupational score had significantly better cognition compared with their co-twins with lower educational-occupational score (B=0.63 (95% CI 0.22 to 1.04), N=570 pairs). Significant within-family educational-occupational score–cognition associations were evident within DZ but not within MZ twin pairs (table 3, figure 2). Results were similar when adjusted for CAIDE score without education but not after adjusting for depressive symptoms (table 3).
Co-twins with higher CAIDE score did not have poorer cognition compared with their co-twins with lower CAIDE score (B=−0.29 (95% CI −0.69 to 0.10), N=570 pairs) and this result was similar when adjusting for depressive symptoms (table 4, figure 2).
Sensitivity analyses
Results were similar when including only pairs with DNA-based zygosity (data not shown). Restricting the CAIDE score analysis to those with at least 16.5 years of follow-up (ie, corresponding the minimum follow-up with educational-occupational score) yielded similar results as in the whole cohort (table 4).
Discussion
In this longitudinal population-based twin cohort study, both CAIDE and educational-occupational risk scores in middle age were significantly associated with old-age cognition over 20 years later. These results are consistent with our earlier reports and suggest that self-report middle-age scores are applicable in recognising middle-aged individuals at risk for cognitive impairment.7 10 One point in CAIDE score was associated with 0.73 points poorer cognition and one point in educational-occupational score was associated with 0.76 points higher cognition. These correspond approximately to the effect of 1.5 years on cognitive performance in this sample. We found no additional predictive ability of self-reported diabetes and smoking beyond the original CAIDE score, as found in another validation study of CAIDE score.6
We are not aware of earlier studies investigating if within twin-pair differences in dementia risk scores are related to within twin-pair differences in old-age cognition. This quasi-experimental twin design indicated that the associations between risk scores and old-age cognition are confounded by genetic and shared environmental influences.
Considering clinical utility, our results suggest that dementia risk scores should be used together with genetic risk. Recognising the importance of genetic influences on the risk score−cognition associations is also important when designing intervention trials. For example, in the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) study where participants were selected according to CAIDE score, intervention effects may be different between those with or without the Apolipoprotein E (APOE) ε4-allele.21 However, genetic risk of dementia goes beyond APOE. Although AD is highly polygenic, current polygenic risk scores of AD account for only a small part of its heritability.22 Within-family analyses in MZ pairs control for all genetic effects even without any measured variants.
The within twin-pair analyses showed that the effect of educational-occupational score on old-age cognition was still evident in DZ pairs. However, within twin-pair analyses were non-significant in MZ pairs indicating that the association between educational-occupational score and cognition is confounded by shared genetic factors. A recent Mendelian randomisation study indicated that the association between higher educational attainment and lower dementia risk is mostly due to genetic effects related to intelligence.23 Also, studies with measured young adult intelligence have suggested that the protective effect of higher education is explained mostly by premorbid cognitive ability.24 25
Regarding CAIDE score, neither analyses in DZ or MZ pairs yielded significant within-family associations suggesting that the relationship between CAIDE score and old-age cognition is confounded by shared environmental and possibly to a lesser degree also by genetic effects. Our study does not support the notion that this combination of cardiovascular risk factors would be causally associated with late-life cognition. Mendelian randomisation studies addressing cardiovascular risk factors and later dementia or AD incidence have found no consistent evidence for a causal association between BMI and dementia or cholesterol levels and dementia or AD.26 Further, early family factors such as poor socioeconomic status have found to largely explain associations between cardiovascular health and cognition.27 We also note that the effects of the three main drivers of vascular burden—blood pressure,28 BMI29 and cholesterol levels30—on cognition are age-dependent. In studies with short follow-up times, these cardiovascular risk factors may operate in opposite direction due to reverse causation making it important to measure risk factors before the onset of dementia process. Our results with CAIDE score were similar in a subgroup with at least 16.5 years of follow-up indicating that our results were likely not attributable to reverse causation.
Age has been suggested to be the main driving factor of dementia risk scores with other risk factors having little contribution to the risk estimate beyond age.5 We found that risk scores were associated with old-age cognition over and above age (in within-family analyses, twins were by design age-matched). Adjustments of educational-occupational score with cardiovascular risk factors did not change the results. Both middle-age risk scores were associated with old-age cognition after adjusting for old-age depressive symptoms in between-family analyses. However, in within-family analyses, the significant association between educational-occupational score was no longer significant after adjusting for depressive symptoms. This may be due to the smaller sample size (1101 vs 2335, depressive symptoms available only for those born in 1938–1944) but may also reflect depressive symptoms as prodromal feature of dementia or shared cause of cognitive impairment and depressive symptoms.31
Representativeness of our sample
The prevalence of dementia—based only on telephone interviews—in our study cohort (3.8%, mean age 72.9, range 66–87) is comparable with the prevalence of dementia in the Finnish general population (4.2% in a slightly younger sample of mean age 68.4 years (range 60–76)).32 There was no significant difference in CAIDE score between participants and non-participants of the cognitive assessment. However, participants in the cognitive assessment had higher education and occupational attainment than non-participants. Higher socioeconomic status and better health in study participants are commonly observed phenomena as seen in our study.
Limitations
Performance on telephone interview could be affected by hearing problems or by use of external aids such as calendars or calculators, although advised against. However, only a small percentage of our cohort reported hearing problems and the number of different tasks in our telephone cognition screening tool is an asset. Survival bias could affect the results, but the participants were mostly in their 70s at the time of cognition screening.
Self-reported risk factors may be vulnerable for recall bias and interpretation. However, self-reports of hypertension,33 BMI13 and smoking34 are shown to be reliable and valid in Finnish population. Also, our physical activity measure is a valid tool for identifying physically active and inactive people.35 On the other hand, the self-report of diabetes from the 1980s may represent only the tip of the iceberg as nearly half of persons with diabetes are unaware of it.36 Measuring cholesterol levels also was not routine in the healthcare system in 1970s and 1980s and the thresholds for normal cholesterol values have evolved during the course of the study.
Finally, dementia risk scores do not capture all within-pair variation. For example, co-twins with high school and university-level education have similar education score. Co-twins may also have differing levels of cholesterol and blood pressure even being in the same CAIDE score category. However, the aim of the study was to assess the predictive value of dementia risk scores that used these categories.
Strengths
Strengths of our study include the long follow-up time of over 20 years and enabled dementia risk prediction early enough for possibility of prevention. The baseline age of our cohort (middle-age) is good because we have information on risk factors before the probable onset of the neurodegenerative disease. The co-twin control design enabled to control for shared genetic and environmental effects which is the flagship of our study. The number of MZ (N=226) and DZ (N=343) pairs was relatively large in the co-twin analyses.
Conclusions
Both midlife dementia risk scores (CAIDE and educational-occupational score) predicted significantly old-age cognition. However, co-twin control study design did not support an association between risk scores and old-age cognition independent of shared genetic and environmental factors but rather highlighted the importance of genetic and environmental influences in early detection of high dementia risk individuals. Recognising the importance of genetic underpinnings of these associations is important for understanding the pathways to cognitive impairment and dementia and may also have implications for selecting individuals into intervention trials.
Acknowledgments
We thank Kauko Heikkilä and Teemu Palviainen for data management and Ulla Kulmala-Gråhn, Kristiina Saanakorpi, Maarit Mantere, Riitta Sipilä and Maarit Hanhiala for conducting the telephone interviews and Pia Ruokolinna for data entry. Special thanks goes to all the twins who have participated in the FTC study enabling this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Vuoksimaa
Contributors PI-M: study concept and design, statistical analysis, interpretation of data and drafting the manuscript. NL: acquisition of data, interpretation of data and revising the manuscript. JK: recruitment of the study cohort, supervision of data collection, interpretation of data, revising the manuscript and obtaining funding. JOR: supervision of data collection, interpretation of data, revising the manuscript and obtaining funding. EV: study concept and design, interpretation of data, statistical analysis, drafting/revising the manuscript, study supervision and obtaining funding. All authors have provided critical comments on the manuscript and approved the final version.
Funding This study was supported by the Juho Vainio Foundation and the Academy of Finland research grants (314639, 320109 to EV; 265240, 263278, 308248, 312073 to JK; 310962 to JOR). JOR was supported also by the Sigrid Juselius Foundation and Finnish State Research Funding. NL was supported by the Finnish Cultural Foundation, Päivikki and Sakari Sohlberg Foundation, Yrjö Jahnsson Foundation, Turku University Foundation, Finnish State Research Funding and Finnish Brain Foundation.
Competing interests JOR serves as a neurology consultant for Clinical Research Services Turku (CSRT Oy). PI-M, EV, JK and NL have nothing to disclose.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Because of the consent given by study participants and the high degree of identifiability, data cannot be made publicly available. Data are available through the Institute for Molecular Medicine Finland (FIMM) Data Access Committee (DAC) for authorised researchers who have IRB/ethics approval and an institutionally approved study plan. For more details, please contact the FIMM DAC (fimm‐dac@helsinki.fi).