Article Text

Abstract
Background Common memory aids for people with dementia at home are recommended. However, rigorous evaluation is lacking, particularly what guidance or support is valued.
Objective To investigate effects of memory aids and guidance by dementia support practitioners (DSPs) for people in early-stage dementia through a pragmatic, randomised controlled trial.
Methods Of 469 people with mild-to-moderate dementia and their informal carers, 468 were randomised to a DSP with memory aids or to usual care plus existing dementia guide. Allocation was stratified by Trust/Health Board; time since first attendance at memory service; gender; age; and living with primary carer or not. Primary outcome was Bristol Activities of Daily Living Scale (BADLS) Score at 3 and 6 months (primary end-point). Secondary outcomes for people with dementia: quality of life (CASP-19; DEMQOL); cognition and functioning (Clinical Dementia Rating Scale; S-MMSE); capability (ICECAP-O); social networks (LSNS-R); and instrumental daily living activities (R-IDDD). Secondary outcomes for carers: psychological health (GHQ-12); sense of competence (SSCQ).
Results DSPs were successfully trained, compliance was good and welcomed by participants. Mean 6 months BADLS Score increased to 14.6 (SD: 10.4) in intervention and 12.6 (SD: 8.1) in comparator, indicative of greater dependence in the activities of daily living. Adjusted between-group difference was 0.38 (95% CI: −0.89 to 1.65, p=0.56). Though this suggests greater dependency in the intervention group the difference was not significant. No differences were found in secondary outcomes.
Conclusions This intervention did not maintain independence in the activities of daily living with no improvement in other outcomes for people with dementia or carers.
Trial registration number Current Controlled Trials ISRCTN12591717.
- dementia
- memory
- AIDS
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request from the corresponding author
Statistics from Altmetric.com
Introduction
Dementia affects over 47 million people worldwide,1 with 850 000 people with dementia in the UK at any one time.2 Numbers are predicted to increase, creating a challenge for health and care services to meet the needs of individuals living with the condition and their families.3 Many people with dementia find it difficult to manage their day to day problems. Interventions to help them and their families manage these problems and difficulties can help to maintain functioning, and so independence from carer help, thus improving quality of life. To address this, the Lancet Commission on Dementia4 recommended that interventions should be multicomponent, individualised to need, support carers in their coping skills and modify the environment around the person with dementia. Provision of memory aids, for those diagnosed with early-stage dementia, aiming to assist with daily living activities by sustaining cognitive and functional abilities5 6 and reducing carer burden7 have been explored. The use of these common, low-technology, aids, like calendars, clocks, whiteboards with electric timers and ‘post-it’ note dispensers, is widely recommended in clinical practice and by support organisations8; many are used by people with dementia at home, often with support from their family carers. However, rigorous effectiveness evaluation is lacking, particularly of what guidance for using aids is valued, although people with dementia report a preference for such advice to be provided at home by a trained worker.9 A Cochrane review10 identified several studies reporting the usefulness of such memory aids or associated training, but they were small or low quality, with only two trials identified. One trial11 evaluated improvement in medication adherence from using an electronic pill dispenser, but although participants had memory impairment they had no validated dementia diagnosis. The ATTILA RCT12 evaluated whether assistive technology and telecare assessments and interventions extend the time people with dementia may continue to live independently at home. However, the interventions were not directed towards assistance with memory problems but rather safety concerns (eg, provision of pendant alarms). This review therefore highlighted the need for a larger and more dedicated study, building on evidence from small-scale trials and other studies.13–17
The rationale for these aids is that they can help people with dementia overcome some of the effects of their memory problems so promoting achievement of daily living activities for longer. In a context where memory is progressively deteriorating, the effectiveness of such memory aids would not be judged by improvements in cognition per se, but by the extent to which people with dementia may act more independently to attain their daily goals, for example keeping appointments and performing activities independently. This is the domain in which the effects of such aids may be judged as successful or not—the proximal, or targeted outcome that such interventions are designed to impact on following completion. There may be further distal outcomes from use of such aids; the person may be less agitated or confused, and may experience a better quality of life; and their informal carers may experience less burden.18 19
The Dementia Early-Stage Cognitive Aids New Trial (DESCANT), a multisite, pragmatic randomised trial, tested the effectiveness of this approach on relevant outcomes for people with dementia and their carers. We implemented and evaluated the effectiveness of guidance by dementia support practitioners (DSPs) to support people with early-stage dementia and their carers in using memory aids at home, relative to treatment as usual. We designed the intervention to be relatively inexpensive, realistic and scalable20 for use within the UK NHS or by third-sector organisations.
Methods
Study design
This trial was preceded by a feasibility study and internal pilot. Randomisation allocation was in equal proportions between intervention and comparator groups. We recruited people with mild-to-moderate dementia with an identified primary carer—from memory services within 10 Health Trusts/Boards across England and Wales. Trained DSPs delivered the interventions in participants’ homes.
Trained interviewers assessed the capacity to consent of potential participants according to the principles of the Mental Capacity Act (2005). We asked those judged to have capacity for their written informed consent. For those judged to lack capacity, we asked their primary carer or a personal consultee about whether the person would have consented and asked that person to provide written consent on their behalf.
Carers gave written informed consent to provide data about the person with dementia. We checked their agreement to continue participation at each visit. We also undertook interviews with carers to investigate their own outcomes, for which they provided separate written informed consent.
Participants
Eligibility criteria for people with dementia were diagnosed dementia of mild-to-moderate severity; aged 50 years or more; under the care of a trial memory clinic; within 1 year of their first attendance for dementia; physically (judged from medical records) and clinically (judged by a responsible clinician) able to engage with the intervention, for instance able to hold, view and use the memory aids and be sufficiently able to interact with the DSP; living in their own home or sharing with a relative; and having an identified carer, defined as the primary person who feels responsible and supports them.
Study treatments
Our trial protocol describes the intervention and rationale.21 The 4-week intervention aimed to improve the abilities, functioning and independence of people with early-stage dementia and their carers, by providing a range of memory aids, and training and support in their use. DSPs delivered the intervention using a manual (https://sites.manchester.ac.uk/home-support-dementia/) to guide each of the four sessions, with worksheets to facilitate and record delivery (‘Intervention record’). The aim was to deliver the first session face-to-face at home to participant pairs within 2 weeks of randomisation. During this session DSPs collected information about memory problems, current use of memory aids, and what goals participants would like to achieve by participating, using standardised and study specific worksheets.22 DSPs provided an appropriate pack of memory aids and support at the first session. They used core memory aids: whiteboard; clock showing day and date; post-it notes; pen and notepad; and calendar. These were selected as they are readily available, were simple to install, and are relatively inexpensive. DSPs also had the flexibility to purchase more items within a budget of £150 per participant to tailor their intervention to individual goals. Additionally, they could also provide support with memory aids already in use within the home. Two telephone follow-up support sessions and a final session face-to-face at home with participants and their carers were undertaken by DSPs. While the first and fourth sessions were a core part of the intervention, intermediate support sessions—telephone or face-to-face to deliver or adjust a memory aid—were optional. A reflection of the fact that this was a personalised intervention, throughout there was flexibility for participants, people with dementia or carers, to meet the DSP jointly or separately if they wished, and it was recognised that the extent of participation in each session could vary depending on the preferences of the person with dementia and their carer.22
All participants received usual care from memory clinics, in accordance with clinical guidance. This comprised help from clinic staff, post-diagnostic counselling and advice, and specialist follow-up as appropriate.
Data collection
We trained clinical staff in participating sites. They completed a screening tool to check participant eligibility, gave a participant information sheet to eligible participants, and sought oral consent to refer them to the DESCANT team. We collected baseline data from outcome questionnaires before randomisation and followed all participants up 3 and 6 months after randomisation. The research team checked the quality of these data.
Outcomes for people with dementia
The primary outcome at 6 months was the carer-rated Bristol Activities of Daily Living Scale (BADLS),23 representing independence in the activities of daily living; scored 0–60 with higher scores showing worse impairment. Secondary outcomes at 3 and 6 months after randomisation were Control, Autonomy, Self-realisation and Pleasure 19-item (CASP19),24 scored 0–57 with higher scores showing better quality of life; Clinical Dementia Rating scale (CDR),25 scored 0–3 with higher scores showing worse cognitive and behavioural functioning; Dementia Quality of Life (DEMQOL,26 scored 28 to 112 with higher scores showing better quality of life; Investigating Choice Experiments for the Capability of Older people (ICECAP-O),27 scores between 0 (no capability) and 1 (full capability); Lubben Social Network Scale-Revised (LSNS-R),28 scored 0–60, with higher scores showing more social engagement; Revised Interview for Deterioration in Daily Living Activities in Dementia (RIDDD),29 with Initiative scoring between 0 and 60, Performance scoring between 0 and 76 and higher scores showing greater impairment; and the Standardised Mini-Mental State Examination (S-MMSE),30 scored between 0 and 30 with lower scores showing worse cognitive impairment. To estimate use of health and social care resources we completed the Client Services Receipt Inventory31 and Resource Utilisation in Dementia questionnaire.32 The interviews took about one and a half hours.33
Outcomes for carers
Secondary outcomes for carers were the General Health Questionnaire (GHQ-12),34 scoring between 0 and 36 with higher scores showing worse health and the Short Sense of Competence Questionnaire (SSCQ),35 scoring from 7 to 35 with higher scores showing greater competence.
Randomisation and masking
Trial managers coordinated recruitment and forwarded participants’ details to the trials unit’s email-based randomisation service. After baseline interviews, the unmasked trial data manager oversaw randomisation, which allocated participants in equal proportions between intervention and comparator groups, stratified by Trust or Health Board (1 of 10); time since first attendance at memory clinic (more or less than 90 days); gender (male or female); age (more or less than 75 years); and living with primary carer or not. Allocation between groups used dynamic software to randomise participants in real time, thus preventing subversion while ensuring (stochastic) balance between groups.36 Participants then received a letter specifying their allocated group and reminding them what this entailed. Participants in the comparator group received a general guide to dementia.8 Participants in the intervention group received invitations to arrange initial visits by the DSP within 2 weeks of randomisation.
Masking participants, carers or DSPs was not possible. Researchers conducting baseline and follow-up interviews were masked to treatment condition and participants were asked not to disclose the group they were allocated to. In this way, interviewers were kept masked as much as possible, although we also asked them to indicate what group they believed the participant had been allocated to at the end of each follow-up interview.
Sample size
We calculated that an analysable sample of 360 (180 in each group) across participating sites would yield 80% power to detect an effect size (standardised mean difference) of 0.30 on BADLS, using a two-sided significance level of 5%. To allow for 25% attrition (estimated from previous studies37) between baseline and final interviews, we aimed to randomise 480 pairs of people with mild-to-moderate dementia and their carers.
Statistical analysis
Analysis followed a statistical analysis plan approved by our Data Monitoring and Ethics Committee (DMEC) before data were accessed. We analysed data on all participants by treatment allocated. Analyses were done in Stata V.16. We present descriptive statistics, by group, for baseline characteristics of participants randomised and in the primary analysis. To characterise the effect of the intervention over time, we fitted multilevel mixed-effect models, as these take better account of missing data, especially if missing at random, and explicitly account for correlations between repeated measurements within each participant.38 Analyses by treatment allocated estimated the effect of the intervention on participants by adjusting for baseline differences in the measure under analysis, participant characteristics (viz Trust/Health Board, age, gender and ethnicity), time since first attendance at memory clinic or equivalent, whether living with primary carer or not and the time to follow-up. We followed this plan both in primary analysis of BADLS and secondary analyses of all other outcomes.
We excluded participants without any follow-up data from the main analyses. We followed published rules for imputing missing data for individual outcome measures. To investigate the potential effects of missing data on the primary outcome, we performed a multiple imputation with Markov Chain Monte Carlo procedures. This, the most common parametric approach for multiple imputation, assumes that all the variables in the imputation model have a joint multivariate normal distribution. We undertook sensitivity analysis comparing estimates with and without imputation.
Study monitoring
A Trial Management Group (TMG) monitored compliance with the study protocol, operating procedures and liaised with Trusts/Boards to recruit participants. The TMG oversaw and resolved operational issues, and reported to the DMEC, the Programme Steering Committee and the funder.
To ensure the intervention and research methods that worked in practice, we completed an internal feasibility study and pilot with 40 participants recruited from the two initial host Trusts in equal numbers, in August 2017. We adapted the Acceptance Checklist for Clinical Effectiveness Pilot Trials criteria39 to assess whether the intervention and trial protocol worked in practice, and the DMEC accepted these criteria. The decision from the pilot was that the design and methods were feasible and appropriate and that the intervention training and procedures were acceptable, to DSPs and participants. DSPs considered the available budget to be feasible to fund necessary items. Despite their low cost they found the aids to potentially permit individualised responses to identified needs. Participants valued the strategies and advice from DSPs in tandem with the provision of aids. Participants provided positive feedback to DSPs about the memory aids, particularly the orientation clock, whiteboards and calendars. People with dementia reported reduced reliance on their carer and carers the opportunity to discuss dementia and its impact.22 The only adjustment suggested by the pilot was to reduce the length of follow-up from the initially planned 12 months–6 months for the main study. This enabled us to meet recruitment targets and tackle the more realistic goal of improving BADLS Scores over 6 months. Thus, we included the pilot data, adjusted to reflect this change, in the main analyses. The University of Manchester as Sponsor approved this modification and we communicated this to the National Research Ethics Service which approved the original protocol, sites and participants.
The DMEC could halt the trial for safety or ethical concerns. Only the DMEC had access, through the trial data manager, to un-blinded data before the trial ended in November 2019 and they approved the blinded primary analysis.
Patient and carer involvement
We involved people with dementia and their carers through a Public, Patient and Carer Reference Group (PPCRG), in North West England and a Lay Advisory Panel across the country, established through Together in Dementia Everyday, a national charity advocating on behalf of carers of people with dementia. The PPCRG helped specify research questions, select outcome domains and design the intervention, including guidance given to the comparator group. The PPCRG also advised on data collection procedures, patient facing materials and on strategies to boost recruitment. Carers of people with dementia were formal members of the trial DMEC and Programme Steering Committee.
Results
Trial progression and recruitment
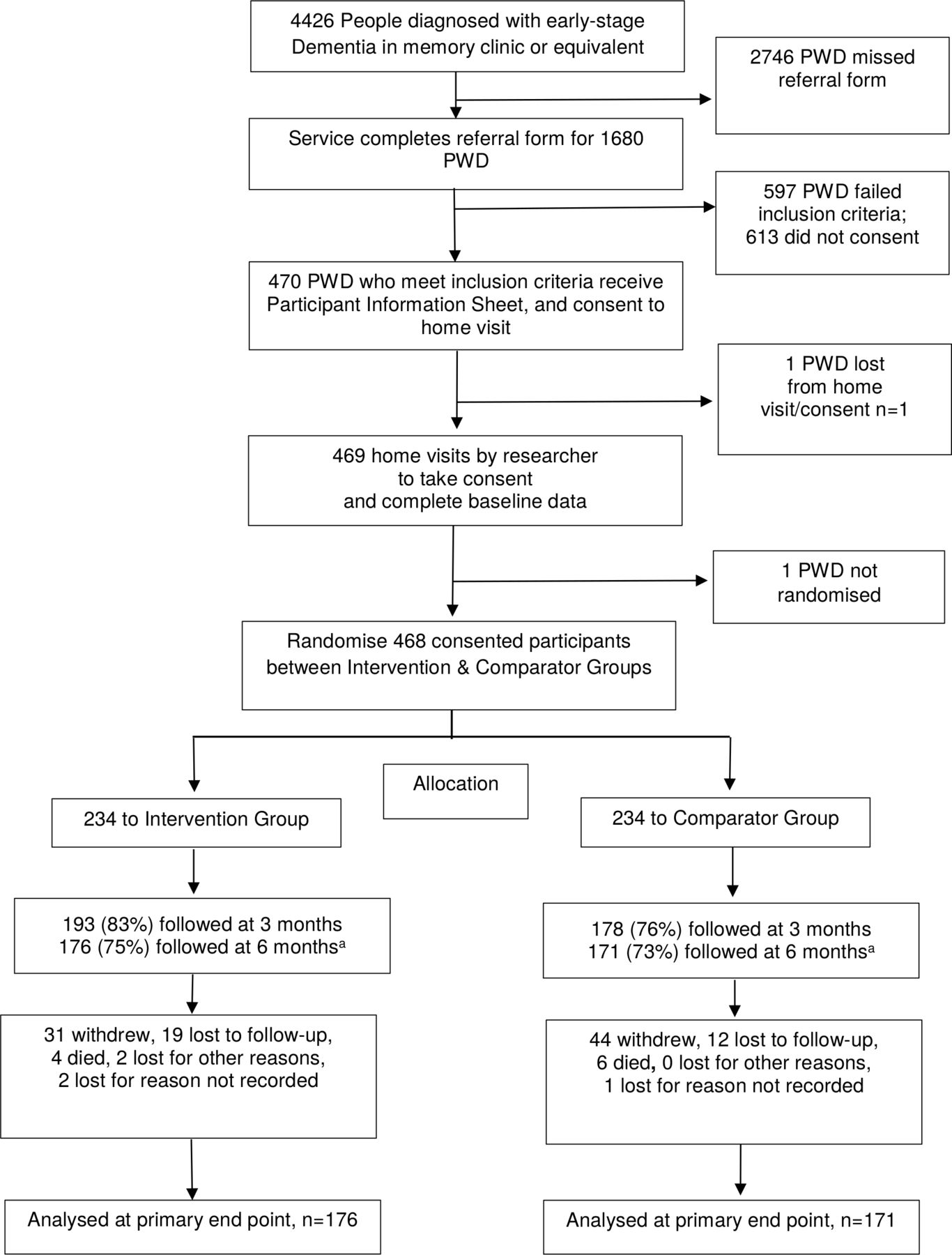
We recruited participants incrementally over 3 years, with sites added from the support to recruitment provided by the infrastructure of the funder, the National Institute for Health Research in England. Figure 1 shows that between 25 November 2016 (first participant enrolled on 6 December 16) and 25 November 2019 (when data were locked for analysis), we screened 4426 people, found 1680 potentially eligible and recruited 470; as one participant missed the home visit and thus informed consent and another withdrew before randomisation, we randomised 468–234 to the intervention and 234 to usual care. Four (2%) participants died in the intervention group and 6 (3%) in the comparator. The mean (SD) duration of intervention visits was 94 min (29) for the first visit, 17 (11) for first follow-up, 17 (16) for second follow-up and 55 (25) for the final review.22 The intervention followed at a mean (SD) of 15 (11) days after randomisation. The mean (SD) number of days between first and last sessions was 26 (9). In total 121 participants (58 intervention and 63 comparator) withdrew: 75 actively withdrew (31 intervention and 44 comparators); 31 were lost to follow-up (19 intervention and 12 comparators); one participant withdrew following a serious adverse event unrelated to the intervention; and one for another reason (both intervention). Ten participants died (four intervention and six comparators), and reasons were missing for three participants (two in the intervention arm).

Flowchart for participants through the Dementia Early-Stage Cognitive Aids New Trial. aThough final follow-up was originally at 12 months, the Data Monitoring and Ethics Committee agreed to reduce this to 6 months after the pilot. PWD, person with dementia.
Sample
The 468 randomised participants were slightly fewer than the 480 estimated as needed to achieve our analysis target of 360, to allow for attrition characteristic of recruitment in this vulnerable population. Attrition at 6 months was slightly higher than expected (26% rather than 25%), so the number of participants for primary analysis, with data at baseline and 6 months, was 347, also slightly lower than target. Baseline characteristics of the randomised and analysed samples were well-balanced (table 1). The average age of those with dementia was around 80 years, with slightly more females. At referral, 376 (80%) people with dementia were able to provide informed consent; the remaining 92 (20%) needed a consultee. Table 1 shows baseline characteristics of randomised and analysed participants.
Baseline characteristics of randomised participants (people with dementia) and those providing data for analysis of the primary end point (BADLS Score at 6 months) by arm
Intervention
DSPs in each of the 10 Trusts/Health Boards delivered the intervention to people with dementia and their carers. A sample of 126 intervention records22 showed good engagement with almost all participants (98%) fully completing the sessions, delivered as planned with packages individually tailored to participants’ preferences. The mean interval between randomisation and the first home visit, the duration of visits and the total duration of the intervention were consistent with study protocol. Variations in delivery typically reflected participants’ goals and preferences (eg, time of day, availability of a carer) and DSP availability. Misplacement of items and orientation to date and time were common areas of need. Memory aids frequently supplied or supported included orientation clocks, whiteboards, calendars and notebooks as well as bespoke items. The intervention was acceptable, with little negative feedback. Unforeseen benefits included the recognition of undiagnosed memory issues in a family member and the use of memory aids by other family members to coordinate care.22
Resource use
At baseline health and social care resource use differed between arms: more people with dementia in the intervention group had been inpatients on general medical wards (online supplemental table A1). Some participants already had memory aids at home, notably clocks or medication reminders, but without guidance from a DSP; this existing use of aids did not differ between groups. At 6 months, more intervention participants had received visits from a social worker, dementia support worker or health visitor; or been admitted to general medical wards. More participants in the usual care group had received aids, adaptations or equipment at follow-up. We report cost-effectiveness of the intervention elsewhere.40
Supplemental material
Serious adverse Eevents
There were 43 SAEs in 42 participants (24 intervention and 18 comparators). One comparator experienced two SAEs, both falls. People with dementia experienced 36 of these SAEs. No SAE was definitely, probably or possibly related to the intervention. Eight SAEs resulted in death (four in intervention arm, four in comparator); three were life threatening (one intervention, two comparator); two caused persistent or significant disability or incapacity (both intervention); one comparator suffered another medically important condition; and 29 were hospitalised (17 intervention, 12 comparator).
Outcomes
Table 2 shows the main treatment effect estimates for the primary outcome. The intervention group began with higher unadjusted BADLS Scores (showing more dependency), which stayed constant at 3 months, but showed a marked increase to significantly higher dependency than the comparator group at 6 months. This significance was due in part to higher BADLS Scores in comparators who were lost to follow-up or died between baseline and 6 months.
Unadjusted findings for BADLS (primary outcome) by arm
The multi-level mixed-effects models showed no significant differences between arms over time (table 3 and figure 2) in BADLS, the primary outcome. Outcomes in both groups reflected increasing dependency over time in activities of daily living. BADLS Scores showed a mean difference of only 0.38 at 6 months, slightly but not significantly favouring the comparator group (95% CI: −0.89 to 1.65, p=0.56). There were no significant differences between groups for all other patient-reported and carer-reported outcomes (table 4 presents summary data; online supplemental tables A2−A11 present full data for each).

{kind=link}
{kind=link}
Mean (95% CI) BADLS Scores (adjusted) over time by group allocated. Here n values are: 468, 371 and 347 for the three time points, respectively. BADLS, Bristol Activities of Daily Living Scale; TAU, treatment as usual.
Adjusted (multilevel mixed model) estimates for primary outcome, BADLS: coefficients
Adjusted (multilevel mixed model) estimates for secondary outcomes: coefficients
Sensitivity analyses for the primary outcome, BADLS, accounting for missing data showed no differences in outcome estimates with and without imputation (online supplemental table A12 and figure A1).
At 6 months, interviewers indicated they knew treatment assignment in 33 (14%)/234 cases in the usual care arm and 82 (35%)/234 in the intervention arm (overall 25 %). Including masking status in covariate adjustment did not alter the treatment effect.
Discussion
Our 4-week programme, in which DSPs added to usual care by offering guidance in the use of memory aids at home, did not improve independence in the activities of daily living for people with mild-to-moderate dementia. We implemented the intervention as planned, and people with dementia and their carers welcomed it. But that did not translate into improvements in independence in activities of daily living, quality of life, or in carers’ outcomes.
Comparison with previous studies
These results are less positive than some other studies,41 42 but those studies are smaller and in single centres. Furthermore, those interventions were not as well designed and included little dedicated training. Some previous studies investigated provision of memory aids and training and concluded that these helped with everyday memory. One trial of a memory aids service43 compared a three-session 6-week clinic programme with waiting list controls for people with neurological conditions. This benefited participants’ everyday memory goals if they had a non-progressive condition; but did not measure activities of daily living. There were no benefits for those with progressive conditions, like dementia. That study concluded that more than three training sessions were needed for those with progressive memory problems. Another trial41 reported training in using a notebook/calendar system for participants with mild cognitive impairment and found beneficial effects on activities of daily living. However, this recruited only 40 participants and excluded participants with dementia. A trial of cognitive rehabilitation for people with early-stage Alzheimer disease,42 including practical aids and strategies to assist memory, found improved goal performance and satisfaction, but randomised only 69 participants.
Strengths and limitations
We improved on previous studies by including systematic training and record-keeping, and an extended number of sessions in participants’ homes—a familiar environment most likely to yield benefit. We delivered the intervention as planned, with good compliance by participants and carers. Compared with other trials we recruited a much larger sample and covered a greater geographical spread. Our analysis of both observed and fully imputed data, taking account of missing data, yielded similar estimates of treatment effects on activities of daily living.
Though we could not mask participants and carers to treatment allocation, masking was neither feasible nor desirable. Recruiting enough people with dementia living at home is challenging for all such trials. Though our sample was slightly smaller than target, and our analysis slightly underpowered, we found no hint of benefit.
Interpretation
Our intervention was implemented successfully,22 with high compliance and delivery as planned. Following several small studies, we aimed to improve independence in activities of daily living by using DSPs to deliver memory aids to participants’ homes, and guide their use. Our prespecified effect size, used in our sample size calculation, corresponded to a 3.5 minimum clinically important difference on BADLS, with a SD of 8.7.44 However, we found an adjusted average effect of only 0.38, with dependency in the activities of daily living increasing over time, consistent with published evidence.45 Any slowing of that dependency is a valuable consequence of care with tertiary prevention a legitimate aim.4 But the intervention did not achieve that aim. It may be that this kind of practical intervention may be useful much earlier in the course of dementia in promoting independence, even before diagnosis when abilities have not deteriorated to the same extent. However, assistance like this cannot be accessed earlier in existing service systems (at least in the UK) as diagnosis is the gateway to receiving such formal, tailored support. However, it could also be that the 4-week duration of this intervention was insufficient to realise its potential effects.
Recommendations
A dedicated practitioner to guide and advise on the use of memory aids cannot be recommended as a care option to maintain independence in activities of daily living in people with dementia. In future, similar trials should investigate other outcomes valued by people with dementia, for example engagement and other, more subtle effects, such as increased confidence, enhanced relationships, feeling valued and respected, not yet measured in trials.46 The effectiveness of offering other types of guidance needs investigation with such outcome measures. However, this intervention was not an effective way to manage daily living activities, or our other outcomes, for people with mild-to-moderate dementia or their carers.
Conclusion
A 4-week programme of advice, guidance and support in using memory aids, did not increase independence in activities of daily living in people with mild-to-moderate dementia. Although well received and providing reassurance in other areas, such as enhanced information for carers and advice as to unmet needs, it did not improve the outcomes studied.
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request from the corresponding author
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by national ethics review committee (REC No 16/NW/0389; 13/05/16), Health Research Authority (HRA) and research governance in each organisation. All participants or consultees gave informed consent before taking part.
Acknowledgments
We thank all participants and their carers for agreeing to take part in the study. We would like to thank the following people for their important contributions: Programme steering committee (independent members): Ken Wilson, Gail Mountain, Sue Watts, Eileen Symonds, Sabine Landau, and David Britt. Data monitoring and ethics committee: Peter Crome (Chair), Gill Manthorpe, Linda Clare, Zoe Hoare, Anthony Hodgson. Patient and Public Involvement Reference Group: Brenda Roe, Jean Tottie, Anthony Hodgson, Julie Dickinson, Phil Dickinson, Jennifer Lord, David Britt, Cathy Clarke, Graham Gavin, Eileen Gilbert, Dave Gilbert, Dawn Williams, Susan Healey, Joyce Dunne, Jacqui Walker, Cecilia Toole. We thank other members of the DESCANT Trial Team at the University of Manchester, Linda Davies and Sue Davies and interviewers, research nurses and managers in each of the NHS sites undertaking the trial: Carol Harper, Carol Ainsworth, Simon Kaye, Linda Booth, Kim Bennett, Brenda Pimlott, Reagan Blyth, Mrudula Davé, Kim Bennett, Jessica Whiston, Ritchard Ledgerd, Jane Burgess, Krisha Hirani, Jemima Hassan, Sheetal Dandgey, Pat Mottram, Theresa Whittingham, Caroline Mogan, Helen Leyland, Dianne Jones, Willemijn Spoor, Annette.Haddon-Silver, Cathryn Hart, Gavin Dawson, Saba Alam, Kathryn Gilgallon, Emma Anderson, Daniel Kelleher, Pretha Koshy, Lauren Sugden, Sarah Trufhitt, Jo Waring, Antony Bayer, Charlotte Colbeck, Alex Carey, Alison Stubbs, Gina Nelson, Rebecca Davies, Dan Pulford, Polly Bidwell, Shani McCoy, Leena Reddy, Penny Lane, Janine Smith, Viraj Rahul, Liz Dalton.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @PaulClarkn, @RSCOP1
Contributors PC (chief investigator, 8 April 2019 to 31 March 2020) conceived and designed the study and had overall responsibility for study delivery and is the joint guarantor. RP was responsible for trial logistics and management, and led on writing and reviewing of the manuscript. SI did the statistical analysis. JP had lead responsibility for trial logistics and management, and was responsible for writing and reviewing of the manuscript. IR was a grant holder and was responsible for trial design and statistical analysis and for writing and reviewing of the manuscript. GF had lead responsibility for trial management and was responsible for writing and reviewing of the manuscript. RB was responsible for trial logistics and management and writing and reviewing of the manuscript. CE was responsible for trial logistics and management. VG was responsible for trial logistics and management. MO was a grant holder, conceived and designed the study and developed the intervention. JH was a grant holder, helped design the study, led on the development of the training manual and was involved in trial management. HC was responsible for trial management and recruitment lead (until 30 May 2019), responsible for training and quality assurance and developed and helped implement the intervention. DC (chief investigator, 1 July 2015 to 7 April 2019) conceived and designed the study and had responsibility for study delivery. NK was a grant holder, and developed the intervention and trained DSPs in its use. BR was a grant holder and led on PPCRG activities with PC. BM was responsible for trial management (from 30 May 2019 to 31 March 2020). CR (co-chief investigator, 8 April 2019 to 31 March 2020): had responsibility for study delivery and for reviewing of the manuscript. She is the joint guarantor. All authors have contributed to drafting the manuscript and approving the final version. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This trial was funded by the National Institute for Health Research (NIHR Programme Grants for Applied Research, Grant Number DTC-RP-PG-0311-12003) and received additional support from the NIHR Local Clinical Research Networks in England and Wales. NIHR funded the study. It developed a commissioning brief but had no role in the study design, data acquisition, analysis or manuscript preparation. The sponsor (University of Manchester) had no role in the funding, study design, in the collection, analysis and interpretation of data, in the writing of the report and in the decision to submit the article for publication. The views expressed are those of the authors and are not an official view of the institutions or funders. All authors had full access to the data (including statistical reports and tables) in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.