Article Text

Abstract
Objective To optimise dementia prevention strategies, we must understand the complex relationships between lifestyle behaviours, frailty and genetics.
Methods We explored relationships between frailty index, healthy lifestyle and polygenic risk scores (all assessed at study entry) and incident all-cause dementia as recorded on hospital admission records and death register data.
Results The analytical sample had a mean age of 64.1 years at baseline (SD=2.9) and 53% were women. Incident dementia was detected in 1762 participants (median follow-up time=8.0 years). High frailty was associated with increased dementia risk independently of genetic risk (HR 3.68, 95% CI 3.11 to 4.35). Frailty mediated 44% of the relationship between healthy lifestyle behaviours and dementia risk (indirect effect HR 0.95, 95% CI 0.95 to 0.96). Participants at high genetic risk and with high frailty had 5.8 times greater risk of incident dementia compared with those at low genetic risk and with low frailty (HR 5.81, 95% CI 4.01 to 8.42). Higher genetic risk was most influential in those with low frailty (HR 1.31, 95% CI 1.22 to 1.40) but not influential in those with high frailty (HR 1.09, 95% CI 0.92 to 1.28).
Conclusion Frailty is strongly associated with dementia risk and affects the risk attributable to genetic factors. Frailty should be considered an important modifiable risk factor for dementia and a target for dementia prevention strategies, even among people at high genetic risk.
- dementia
- genetics
- clinical neurology
- geriatrics
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. These data are available for approved researchers from the UK Biobank (https://www.ukbiobank.ac.uk/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The number of people with dementia is rising as populations age, leading to personal and socioeconomic challenges. Even so, the age-adjusted incidence of dementia has notably fallen in some high-income countries,1 2 providing hope that dementia risk may be reduced by protective lifestyle and environmental changes. A considerable body of recent work indicates this to be possible,1 but it is unclear in observational data whether adherence to a healthy lifestyle lowers risk for dementia in those at high genetic risk.3 4 Trials of lifestyle interventions aimed at preventing cognitive decline and dementia have shown similarly mixed results.5 6 To propel the promising trend of decline in age-related dementia incidence, we must better understand the modifiable risk and protective factors, and the mechanisms through which dementia trajectories are altered.
Adherence to a healthy lifestyle has been related to lower dementia risk in multiple large cohort studies,3 4 7 but the mechanisms are poorly understood. Cardiovascular risk factors are firmly associated with increased incident dementia,8 but there is limited evidence to suggest that healthy lifestyles reduced risk due to better vascular health.3 4 7 Another possibility is that healthy lifestyles confer protection from dementia by slowing the rate of age-related health-deficit accumulation, otherwise known as the degree of frailty. Frailty is a detrimental health state that exerts a broadly based increase in risk for adverse health outcomes, including mortality.9 For example, frailty has been shown to be independently related to cardiovascular mortality even after adjustment for cardiovascular risk.10 Critically, people who are more frail report more unhealthy lifestyle behaviours11 12 and have an increased risk of developing incident dementia.13
Dementia is a multiply determined, age-related condition. The risk of developing dementia reflects genetic, neuropathological, lifestyle and general health factors.1 13–15 Frailty, as an integrative measure of health, has recently been noted as having a probable role in clinical practice to support prognostic evaluations for patients presenting with cognitive complaints16; it is associated with higher dementia risk largely independently of broad neuropathological markers17 and the APOE ε4 allele,13 and from both amnestic and non-amnestic mild cognitive impairment.18 Frailty has recently emerged as a factor explaining the discordance between neuropathological burden and prevalent dementia, influencing whether AD biomarkers—measured in vivo19 or at autopsy20—are expressed as clinical dementia. These neurodegenerative processes are partly caused by complex interactions between numerous genetic variants, but whether frailty also moderates the dementia risk attributable to those genetic variants is unknown. This proposition may be tested using a polygenic dementia risk score, which captures the breadth of genetic risk for late-life dementia.3 4 14
To support dementia prevention strategies, we must understand the complex relationships between lifestyle behaviours, frailty and genetics. We aimed to address this in the UK Biobank by using established resources: a healthy lifestyle score,4 a polygenic risk score for dementia,4 and a frailty index.21 After first establishing a relationship between the degree of frailty and dementia risk, we pursued two primary objectives: (1) determine the extent to which differences in the degree of frailty account for the protective effects that a healthy lifestyle may impart on dementia development and (2) assess whether frailty moderates the expression of polygenic dementia risk.
Method
Participants
Data came from the UK Biobank, a large, UK-based prospective cohort study.22 Between 2006 and 2010, 502 493 individuals were recruited and underwent a comprehensive baseline assessment of health and function. This included self-reported data on lifestyle behaviours and medical information, measurement of physical functioning, and biomaterial sampling. We included only those participants who were aged 60 years or older and who did not have dementia at their baseline assessment (as identified via self-report or hospital inpatient records). We excluded some participants due to not having information available on date of dementia diagnosis, as well as participants who could not have polygenic dementia risk or baseline frailty index scores calculated due to missing data (figure 1).

Analytical sample flow chart.
Incident dementia
The main outcome was incident all-cause dementia. This was obtained chiefly through hospital admission records (N=1705; 97% of dementia cases), which included information on admissions and diagnoses from the Hospital Episode Statistics for England, Scottish Morbidity Record data for Scotland, and the Patient Episode Database for Wales. Additional cases of all-cause dementia were identified in death register data (N=57; 3%) from the National Health Service Digital for England and Wales and the Information and Statistics Division for Scotland. In both instances, the International Classification of Diseases, Ninth Revision and 10th Revision codes for Alzheimer disease and dementia from other causes were used,23 which are detailed elsewhere.4 In a study of UK Biobank participants recruited in Edinburgh, dementia codes sourced from a combination of hospital and mortality records had a positive predictive value for dementia of 84.5% (95% CI 72.6% to 92.7%).24
Frailty index score
The degree of frailty at baseline was measured for each participant using a 49-item frailty index, previously constructed and validated in the UK Biobank (online supplemental table 1).21 A frailty index is a health-state measure that integrates information from several physiological systems.9 The health variables used to calculate a frailty index are routinely collected in clinical examinations, such as symptoms, signs, disabilities and diseases that meet standard criteria.25 For each person, the score is calculated as the proportion of health attributes that a person has in a deficit state. Frailty index scores range from 0 (indicating no health deficits) to 1 (indicating every health deficit that was assessed). For instance, a person reporting 15 of 45 health deficits that were assessed has a frailty index score of 0.33 (15/45). Similar scoring can be done in preclinical models.26 Frailty index scores were multiplied by 10 so that HRs could be meaningfully interpreted as the change in dementia risk per 0.1 increase in frailty index score, equating to ~5 additional deficits. We classified participants whose frailty index scores were ≥0.3 as high frailty,11 intermediate frailty (score ≥0.15 and <0.3) or low frailty (score <0.15).
Supplemental material
Healthy lifestyle score
The healthy lifestyle score had also been implemented and validated in the UK Biobank and was associated with dementia risk.4 The score was calculated using information on participant adherence to behaviours known to affect dementia risk (smoking status, physical activity, diet and alcohol consumption). Depending on adherence to national recommendations, participants scored 0 (did not adhere) or 1 (adhered) on each of the four healthy behaviours. Points on the healthy lifestyle score were accumulated if participants were not current smokers, if they participated in regular physical activity as defined by the American Heart Association,27 if their consumption of at least four of seven commonly eaten food groups complied with recommendations on dietary priorities for cardiometabolic health,28 or if their consumption of alcohol was defined as moderate as per US dietary guidelines.29 Healthy lifestyle scores ranged from 0 to 4, with higher scores indicating greater adherence to behaviours known to reduce dementia risk.
Polygenic dementia risk score
We used too an existing, validated polygenic risk score for dementia.4 This score is represented by a single value and captures individual variability in the inheritance of 249 273 single-nucleotide polymorphisms (SNPs) associated with dementia risk.30 Contributing SNPs were those most strongly associated with Alzheimer’s disease in each linkage disequilibrium block, with a p value threshold of less than 0.50 used for their inclusion. The number of alleles associated with each SNP was weighted by the strength of their relationship with Alzheimer’s disease,30 summed and then standardised. Scores were calculated exclusively for individuals whose self-reported racial/ethnic background was white (British, Irish or other white background) as the genome-wide association study included only individuals of European ancestry.30 A polygenic risk group variable was also coded, in which participants were classified at low polygenic risk (lowest quintile), intermediate polygenic risk (quintiles 2–4) and high polygenic risk (highest quintile).
Covariates
Age at baseline, sex, education level, socioeconomic status, the polygenic risk score, the number of alleles included in the polygenic risk score, third-degree relatedness (a flag denoting a person to be a third-degree or closer relative of at least one other person in the cohort), and the first 20 principal components of ancestry were included as covariates in all statistical models due to possibly confounding the relationships between the key study variables and dementia risk.4 Sex and highest obtained education level were self-reported. Socioeconomic status was derived from the Townsend deprivation index,31 calculated based on the national census output area in which a participant’s postcode was located. It was categorised as least deprived (lowest quintile), intermediate deprivation (quintiles 2–4), and most deprived (highest quintile). Genetic relatedness of the sample was controlled for by using the third-degree relatedness of individuals in the sample, as well as the first 20 principal components of ancestry. Finally, as each model included the polygenic risk score, we included the number of alleles used in its calculation as an additional covariate.
Statistical analysis
Baseline characteristics were summarised using means and SDs for continuous normal variables, and medians and IQRs for continuous non-normal variables. We used Cox proportional hazards models with incident dementia time-to-event data to examine the relationships between variables of interest and dementia risk, and multiple linear regression models to examine the relationships between variables of interest and frailty index scores. Follow-up began at participants’ baseline assessments (conducted between 2006–2010) and continued until whichever occurred earlier: dementia diagnosis; lost to follow-up (primarily due to leaving the UK); death; or the last date of hospital admission (censored at 31 March 2017 for England, 31 October 2016 for Scotland and 29 February 2016 for Wales). First, we examined the links between frailty and incident dementia. Second, we conducted mediation analysis to determine whether, and the degree to which, differences in frailty explained the relationship between healthy lifestyle behaviours and dementia risk (objective 1). We followed the method of Fulcher and colleagues,32 although we used Cox proportional hazards in place of accelerated failure time models for consistency in interpretation, and estimated indirect effects using the products-of-coefficients method. Finally, we examined whether frailty moderated the expression of polygenic dementia risk (objective 2) by testing a frailty index score by polygenic risk score interaction term and investigated how combined frailty/polygenic risk groups differed in their dementia risk. Analyses were conducted in the total sample and stratified by sex. Relationships were expressed as HRs or unstandardised beta (B) values, depending on the model used, and accompanied by 95% CIs. Missing data were imputed using multivariate chained equations 35 times. Dementia may be diagnosed in hospital settings several years after its emergence, and a relationship between frailty and dementia development may be confounded by undetected dementia. In response, we conducted a sensitivity analysis to investigate the relationship between frailty and incident dementia after having excluded 2878 participants who developed dementia or who were lost to follow-up within 3 years of their baseline assessment. Sensitivity analyses were also undertaken to ensure that associations of frailty and dementia did not solely reflect the eight vascular risk factors, or the other causes and risk factors for cognitive decline, used in the calculation of frailty index scores. An alpha level of 0.05 was used to denote statistical significance. All statistical analyses were conducted using R V.3.6.1.
Results
Sample characteristics
The analytical sample comprised 196 123 participants of European ancestry (mean baseline age=64.1 years (SD=2.9); 53% women). Participants tended to be in good health at baseline, with most classified at low frailty (the highest observed value for frailty index scores in this sample was 0.55) and reporting close to three of four healthy lifestyle behaviours (table 1). Participants were followed for a median of 8.0 years (IQR=7.4–8.6), yielding 1 544 423 person-years of observation time for longitudinal analyses. During this time, 1762 cases of incident dementia were identified, equating to an absolute risk of 0.9% and an incidence rate of 0.11 per 100 years. A correlation matrix of all continuous study variables is presented in table 2. Sex differences in study variables are presented in online supplemental table 2.
Descriptive statistics of the analysed sample stratified by incident dementia
Pearson correlation matrix of continuous study variables
Frailty and dementia risk
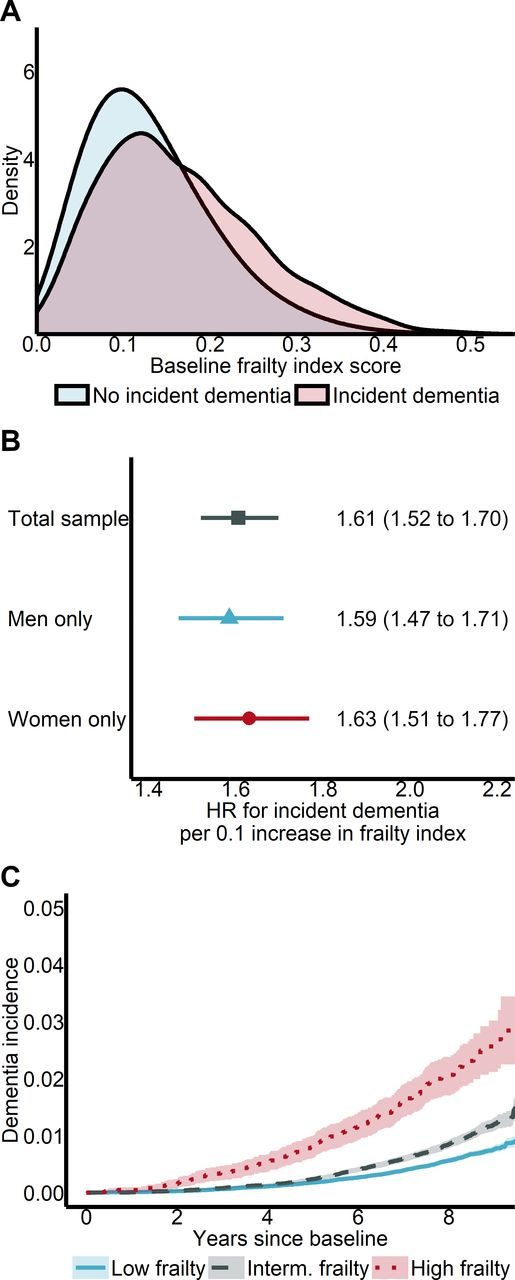
Frailty index scores at baseline were higher among participants who developed dementia than among participants who remained free from dementia (figure 2A). The absolute dementia risk was 4.0 times higher among individuals with high frailty, and 1.7 times higher among individuals with intermediate frailty, when compared with those individuals with low frailty (table 3). Each 0.1 increase in frailty index scores at baseline was associated with an increased dementia risk after adjustment for all covariates and the polygenic risk score (figure 2B). This effect was similar when participants who developed dementia or who were lost to follow-up within 3 years of their baseline assessment were excluded from the analytical sample (HR 1.59, 95% CI 1.50 to 1.69), and slightly weaker when cardiovascular health deficits were excluded from the calculation of frailty index scores (HR 1.51, 95% CI 1.43 to 1.60) and when other causes and risk factors for cognitive decline were further excluded (HR 1.49, 95% CI 1.41 to 1.58). Participants with either intermediate or high frailty had an increased dementia risk compared with those with low frailty (HR 1.55, 95% CI 1.40 to 1.71 and HR 3.68, 95% CI 3.11 to 4.35, respectively; figure 2C). Those differences in risk were similar after removing cardiovascular health deficits from the frailty index (HR 1.54, 95% CI 1.39 to 1.70 and HR 3.88, 95% CI 3.20 to 4.71) and when other causes and risk factors for cognitive decline were further excluded (HR 1.63, 95% CI 1.47 to 1.80 and HR 3.04, 95% CI 2.47 to 3.73).
Descriptive dementia incidence statistics stratified by frailty group

Frailty and incident dementia. (A) Distributions of unadjusted baseline frailty index scores in those who developed dementia (N=1762) and in those who remained free from dementia (N=194 361). (B) Associations of frailty index scores and dementia risk. HRs and 95% CIs were calculated from Cox proportional hazards models adjusted for all covariates for the total sample (N=196 123) and for men (N=92 838) and women (N=103 285), separately. (C) Cumulative dementia incidence within low (N=128 150), intermediate (N=61 931) and high frailty (N=6042) groups as calculated from a Cox proportional hazards model adjusted for all covariates. Analyses in (B, C) were adjusted for age at baseline, sex, education level, socioeconomic status, the polygenic risk score, the number of alleles included in the polygenic risk score, third-degree relatedness and the first 20 principal components of ancestry.
Lower frailty mediates the protective benefits of a healthy lifestyle
We next considered the extent to which differences in the degree of frailty account for the protective effects of a healthy lifestyle on dementia development (objective 1) by testing the hypothesised mediation model (figure 3A). After adjustment for all covariates, each point increase on the healthy lifestyle score was associated with lower dementia risk (slightly more so in men than in women; figure 3B) and with lower frailty index scores (to a similar extent in both men and women; figure 3C). We then estimated the direct effect of healthy lifestyle scores on dementia risk, as well as their indirect effect through frailty index scores (table 4). Just under half (44%) of the protective effect of higher healthy lifestyle scores on dementia risk was mediated by frailty index scores, and just over half was due to mechanisms not accounted for in this study. The size of the mediation effect was similar when participants who developed dementia or who were lost to follow-up within 3 years of their baseline assessment were excluded from the analytical sample (47% mediation), and slightly smaller following the exclusion of cardiovascular health deficits from the calculation of the frailty index (37% mediation) and when other causes and risk factors for cognitive decline were further excluded (33% mediation), but indirect effects in both analyses remained statistically significant. The mediation effect was larger in women compared with men (table 4).
Results of mediation analysis for frailty in the relationship between healthy lifestyle behaviours and dementia risk
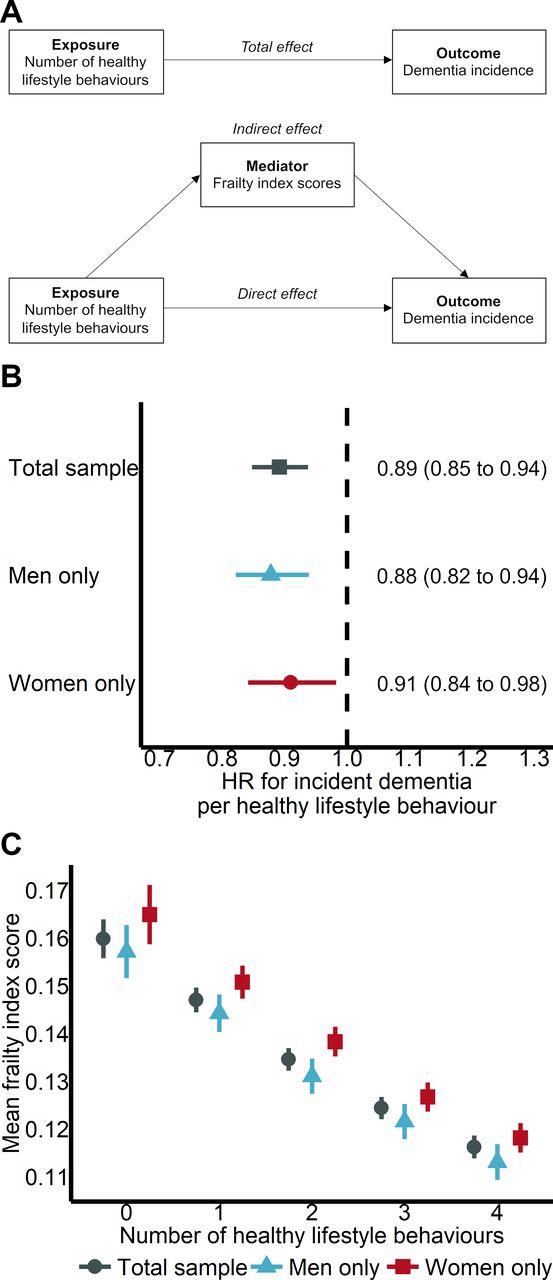
Frailty, lifestyle and incident dementia. (A) The hypothesised mediation model in which a proportion of the protective effect of higher healthy lifestyle scores on dementia development is mediated by lower frailty index scores. (B) The association of healthy lifestyle scores and dementia risk. HRs and 95% CIs were calculated from Cox proportional hazards models adjusted for all covariates (but not frailty index scores) for the total sample (N=196 123) and for men (N=92 838) and women (N=103 285), separately. (C) Relationship between healthy lifestyle scores and frailty index scores. Values represent mean frailty index scores (95% CI) for participants with 0 (N=2091), 1 (N=16 941), 2 (N=54 126), 3 (N=77 347) and four healthy lifestyle behaviours (N=45 618) and were calculated from multiple linear regression models adjusted for all covariates. Analyses in (B, C) were adjusted for age at baseline, sex, education level, socioeconomic status, the polygenic risk score, the number of alleles included in the polygenic risk score, third-degree relatedness and the first 20 principal components of ancestry.
Frailty alters the genetic contribution to dementia risk
Finally, we assessed whether frailty moderates the expression of polygenic dementia risk (objective 2). Each SD increase in polygenic risk score was associated with an increased dementia risk after adjustment for all covariates including frailty index scores (HR 1.24, 95% CI 1.19 to 1.31) and to a similar extent in both men and women. Participants with either intermediate or high polygenic risk had an increased dementia risk compared with those with low polygenic risk (HR 1.38, 95% CI 1.20 to 1.59 and HR 1.92, 95% CI 1.65 to 2.25, respectively; figure 4A). Although individuals at high genetic risk and with high frailty were at 5.8 times greater dementia risk compared with those at low genetic risk and with low frailty (figure 4B), the change in risk due to high polygenic risk was not uniform across frailty groups: each SD increase in polygenic risk was most strongly related to dementia risk in those with low frailty and not associated at a statistically significant level in those with high frailty (figure 4C). The strength of relationship between higher polygenic risk scores and higher dementia risk decreased by 5.5% for each 0.1-point increase in frailty index scores (interaction HR 0.95, 95% CI 0.90 to 1.00, p=0.039). The strength of this association was similar when participants who developed dementia or who were lost to follow-up within 3 years of their baseline assessment were excluded from the analytical sample (interaction HR 0.95, 95% CI 0.89 to 1.00, p=0.068), and when cardiovascular health deficits and other causes and risk factors for cognitive decline were removed from the calculation of the frailty index (interaction HR 0.95, 95% CI 0.90 to 1.00, p=0.046), but CIs marginally widened. This interaction effect was present in men (HR 0.90, 95% CI 0.83 to 0.97) and absent in women (HR 1.00, 95% CI 0.92 to 1.08), though a sex by polygenic risk score by frailty index score interaction term was not statistically significant (interaction HR 1.11, 95% CI 1.00 to 1.24, p=0.055).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Frailty, polygenic risk and incident dementia. (A) Cumulative dementia incidence within low (N=39 224), intermediate (N=117 674) and high polygenic risk (N=39 225) groups calculated from a Cox proportional hazards model adjusted for all covariates. (B) Difference in dementia risk between combined frailty score/polygenic risk groups as compared with a low frailty score/low polygenic risk reference group. HRs and 95% CIs were calculated from a Cox proportional hazards model adjusted for all covariates in the total sample (N=196 123). (C) Associations of polygenic risk scores and dementia risk within different frailty groups. HRs and 95% CIs were calculated from Cox proportional hazards models adjusted for all covariates for the total sample (N=196 123) and for men (N=92 838) and women (N=103 285), separately. Analyses in (A–C) were adjusted for age at baseline, sex, education level, socioeconomic status, the number of alleles included in the polygenic risk score, third-degree relatedness and the first 20 principal components of ancestry; analyses in (A) were additionally adjusted for frailty index scores.
Discussion
We investigated how general health, as expressed as a frailty index score, combined with healthy lifestyle behaviours and genetic risk to give rise to incident all-cause dementia in a large, population-based study. We report four main findings: (1) frailty was associated with a substantial increase in dementia risk that was independent of genetic risk; (2) almost half of the relationship between healthy lifestyle behaviours and dementia risk was mediated by frailty; (3) participants at high genetic risk and with high frailty had a 5.8 times greater risk of incident dementia compared with those at low genetic risk and with low frailty; (4) frailty moderated the expression of genetic risk for dementia, whereby genetic risk was influential in those with low frailty and not in those with high frailty. These results support the notion that dementia is a multiply determined condition, shed new light on how frailty and genetic predisposition interact, and frame frailty as a key modifiable risk factor for dementia targetable through healthy lifestyle behaviours.
The link between frailty and the development of both mild cognitive impairment and dementia is well established.13 17 We observed a quadrupling in the rate of incident dementia in people with high frailty compared with people with low frailty—each five additional health deficits (0.1 increase in frailty index score) represented risk equivalent to 2–3 additional years of age. A novel finding was that frailty increased dementia risk independently of a polygenic dementia risk score. This complements a recent report that frailty increased dementia risk independently of a neuropathological index comprising ten markers of brain disease.17 These data support a role for frailty in dementia development that exists on a pathway separate to known genetic, neuropathological and vascular causes of dementia. Other work has also shown frailty to increase risk for disease-specific outcomes after adjusting for traditional risk factors. For instance, cardiovascular risk and cardiovascular events and related mortality.10 Taken together, evidence implicates frailty as an indicator of generalised vulnerability to ageing-related diseases independent of known risk factors, which is hypothesised to occur, at least in part, through reduced physiological reserve causing the expression of morbidity that would otherwise not meet the threshold required for clinical detection.9 33
Polygenic risk scores are reliably associated with dementia risk and cognitive decline.3 4 14 Here, we provide greater specificity to these associations by demonstrating that the contribution of polygenic risk to incident dementia varied by the degree of frailty. The genetic risk weakened as frailty increased, and dementia developed even in people with no genetic contribution but high frailty. This interaction was strongest among men but, among women too, dementia risk was not significantly affected by genetic risk in those living with high frailty. Similarly, other work has shown frailty to vary the threshold at which dementia developed in relation to Alzheimer’s neuropathology.20 These data show genetic and neuropathological determinants of dementia risk to be less influential in people who are ageing more poorly—possibly as risk becomes saturated and the threshold for a sufficient cause of dementia is reduced by their degree of frailty.9
Adherence to national guidelines for healthy lifestyle behaviours is central to dementia risk reduction recommendations.1 Here, we provide new insight that healthy lifestyle behaviours might exert a considerable proportion of their protective effect through an associated reduction in the degree of frailty, and in a manner that is not driven solely by fewer vascular health deficits as captured by UK Biobank participant questionnaires. Given the links between healthy lifestyle behaviours, frailty and dementia,11–13 our finding was not unexpected. Interestingly, healthy lifestyle behaviours affected dementia risk through multiple independent pathways in men but relied predominantly on lower frailty in women.
Our data do not dissuade from the proposal that preventing or treating frailty could aid in efforts to reduce the burden of dementia.15 Optimally, frailty would be prevented before its emergence, and we found that people who reported more healthy lifestyle behaviours had a lower degree of frailty, which supports other cross-sectional11 and longitudinal evidence.34 In that longitudinal study, reverse causation was controlled for by excluding participants who were frail within 24 months of baseline assessment. In further support of the modifiable nature of frailty, a systematic review of 21 randomised controlled trials found multiple interventions to be effective in treating frailty, although not all interventions were shown to be useful.35 Those interventions that had the highest likelihood of succeeding involved a combination of exercise and nutrition supplementation delivered in group sessions. Longitudinal data show frailty index scores double with every 12.6 years of age,36 suggesting that even relatively small decreases in frailty may result in different clinical outcomes years later.
Our findings should be interpreted with consideration of limitations. The relationships observed may be due to unmeasured or uncontrolled confounding; despite the long follow-up period, the possibility of reverse causation remains, both in terms of frailty preceding an unhealthy lifestyle and dementia preceding frailty. Our results were, however, robust in a sensitivity analysis that excluded participants who developed dementia within 3 years of their baseline assessment. Even so, the relationship between frailty and dementia is necessarily bidirectional: dementia impacts on a person’s ability to engage in healthy lifestyle behaviours, maintain appropriate healthcare, and is associated with increased rates of other illnesses,1 all of which would lead to higher frailty. Furthermore, changes in behaviour and functioning are detectable in the preclinical phase of the disease,37 which could further exacerbate a person’s degree of frailty. Another limitation was that not all cases of incident dementia are captured by medical records or death registers, and these are likely to have been incorporated into our analyses. The consequences of such could bias the reported relationships toward statistical significance (people living with frailty are more likely to attend hospital and therefore be assessed for dementia) or towards the null (people living with frailty are often the ones in whom dementia is overlooked). Similarly, we used survival models with death treated as a censoring event and not as a competing risk; differences in the strength of relationship between a purported risk factor and incident dementia can occur when competing risks are considered.38 Despite the large sample size and the long median follow-up period, the number of incident dementia cases was low, thus limiting statistical power. Despite the detailed health records, we had sufficient data to calculate frailty index scores at baseline only, and conclusions regarding any subsequent change in the degree of frailty were not possible. The healthy lifestyle index implemented here also has limitations, such as lacking specificity due to its narrow range of values. Finally, given that the sample was comprised of volunteers of European ancestry aged 60–73 years, it is not clear to what extent these findings will generalise to other populations.
In conclusion, frailty was shown to exert a strong and reliable effect on dementia risk and to affect the risk attributable to genetic factors. Frailty should be considered an important modifiable risk factor and a target for lifestyle interventions, even among people at high genetic risk of dementia.
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. These data are available for approved researchers from the UK Biobank (https://www.ukbiobank.ac.uk/).
Ethics statements
Patient consent for publication
Ethics approval
The UK Biobank involves human participants and was approved by the National Information Governance Board for Health and Social Care and National Health Service North West Multicentre Research Ethics Committee (approval number: 11/NW/0382).
Acknowledgments
This work was supported by a Canadian Institutes of Health Research Project Grant (PJT-156114). LMKW receives salary support from the Canadian Institutes of Health Research Banting Postdoctoral Fellowship. JMR and DJL are funded by Alzheimer’s Research UK. DJL is also funded by National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) South West Peninsula, National Health and Medical Research Council (NHMRC), JP Moulton Foundation, National Institute on Aging/National Institutes of Health (RF1AG055654), and the Alan Turing Institute/Engineering and Physical Sciences Research Council (EP/N510129/1). KR receives career support from the Dalhousie Medical Research Foundation as the Kathryn Allen Weldon Professor of Alzheimer Research, and research support from the Canadian Institutes of Health Research, the Nova Scotia Health Research Foundation, the Canadian Frailty Network, the Capital Health Research Fund and the Fountain Family Innovation Fund of QEII Health Sciences Centre Foundation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DJL and KR are joint senior authors.
Twitter @David_D_Ward, @Janice_Ranson, @WallaceLindsay, @DrDJLlewellyn, @Krockdoc
Contributors DDW, JMR, LMKW, DJL and KR designed and conceptualised the study; DDW analysed the data, wrote the first draft, and revised all drafts; DDW, JMR, LMKW, DJL and KR interpreted the data; JMR, LMKW, DJL and KR reviewed all drafts; DJL and KR supervised the project. KR accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was funded by a Canadian Institutes of Health Research (CIHR) grant to Kenneth Rockwood PJT-156114, and Team 14 of the Canadian Consortium on Neurodegeneration in Aging (The Canadian Consortium on Neurodegeneration in Aging is supported by a grant from the Canadian Institutes of Health Research with funding from several partners) CIHR grant: CNA-137794.
Competing interests DDW, JMR, LMKW and DJL have nothing to report. KR has asserted copyright of the Clinical Frailty Scale through Dalhousie University’s Industry, Liaison and Innovation Office. Use is free for education, research, and not-for-profit health care. Users agree not to change or commercialise the scale. In addition to academic and hospital appointments, KR is cofounder of DGI Clinical, which in the last five years has contracts with pharma and device manufacturers (Biogen, Shire, Hollister, Novartis, Nutricia, Roche, Takeda) on individualiSed outcome measurement. In 2017, he attended an advisory board meeting with Lundbeck on dementia, and in 2020 chaired a Scientific Workshop & Technical Review Panel on frailty for the Singapore National Research Foundation. Otherwise any personal fees are for invited guest lectures, rounds and academic symposia, received directly from event organiSers, for presentations on frailty. He is Associate Director of the Canadian Consortium on Neurodegeneration in Aging, which is funded by the Canadian Institutes for Health Research, the Alzheimer Society of Canada and several other funding partners.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.