Article Text

Abstract
Functional movement disorder (FMD) is a common manifestation of functional neurological disorder presenting with diverse phenotypes such as tremor, weakness and gait disorder. Our current understanding of the basic epidemiological features of this condition is unclear. We aimed to describe and examine the relationship between age at onset, phenotype and gender in FMD in a large meta-analysis of published and unpublished individual patient cases. An electronic search of PubMed was conducted for studies from 1968 to 2019 according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Individual patient data were collected through a research network. We described the distribution of age of onset and how this varied by gender and motor phenotype. A one-stage meta-analysis was performed using multilevel mixed-effects linear regression, including random intercepts for country and data source. A total of 4905 individual cases were analysed (72.6% woman). The mean age at onset was 39.6 years (SD 16.1). Women had a significantly earlier age of onset than men (39.1 years vs 41.0 years). Mixed FMD (23.1%), tremor (21.6%) and weakness (18.1%) were the most common phenotypes. Compared with tremor (40.7 years), the mean ages at onset of dystonia (34.5 years) and weakness (36.4 years) were significantly younger, while gait disorders (43.2 years) had a significantly later age at onset. The interaction between gender and phenotype was not significant. FMD peaks in midlife with varying effects of gender on age at onset and phenotype. The data gives some support to ‘lumping’ FMD as a unitary disorder but also highlights the value in ‘splitting’ into individual phenotypes where relevant.
- functional neurological disorder
- meta-analysis
- systematic reviews
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Functional movement disorder (FMD) is common but its basic epidemiological features such as age at onset and gender differences and how these vary between phenotypes are not well-characterised.
What this study adds
This international study involving 70 authors and 4905 patients is the largest data set of any functional neurological disorder to date. FMD peaks in midlife for all phenotypes, but dystonia and weakness patients were younger, and those with gait disorder older.
How this study might affect research, practice or policy
Our data provides unprecedented resolution for the basic epidemiology of FMD, highlighting similarities and differences in phenotypes, and shedding light on ‘lumping vs splitting’ questions in this disorder.
Introduction
Functional movement disorder (FMD) is a common presentation of functional neurological disorder (FND)1 with various symptoms of altered movement, including tremor, jerks, dystonia and gait disorders, often displaying combinations of phenotypes. Although heterogeneous, people with different forms of FMD share aetiological risk factors, experience overlapping symptoms such as pain or fatigue and exhibit common findings on physical examination, including variability and distractibility.1 FMD is more commonly seen in women (70% in the largest studies).2
Despite its prevalence, the basic epidemiology of FMD is unclear. With some exceptions,3–6 large-scale epidemiological data are limited due to presentation heterogeneity, as most studies are smaller case series describing specific phenotypes. It is unknown whether different FMD phenotypes are associated with differences in age at onset (eg, whether functional parkinsonism is more common in older individuals) or if certain phenotypes exhibit gender differences (eg, the reported higher incidence of functional axial myoclonus in men).7 There is evidence that gender ratios may vary by age at onset in other forms of FND. A large case series of 698 subjects with functional seizures reported the mean age at onset in women was significantly younger than in men, yet was approximately equal between genders at the extremes of life.8 Characterising basic data in larger samples can uncover clues to underlying risk factors for developing FMD or potential underlying neurobiological mechanisms.
We collected a large data set on FMD from (1) a systematic review and individual patient data meta-analysis using published data, and (2) unpublished data from individual researchers. Adding unpublished data permits reliable augmentation of the data set beyond published studies. We also planned a comparison with a large, published set of similar data for people with functional seizures. We hypothesised that women would have an earlier age at onset than men, perhaps related to higher frequency of childhood adversity and there would be gender differences among FMD phenotypes, which may be partly explained by differing age at onset.
Methods
Study design
An individual patient data (IPD) meta-analysis was performed including published and unpublished FMD cases. The University of Toronto coordinated, collected and managed data, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.9 The systematic review protocol was not registered.
Eligibility criteria and phenotypic characterisation
Inclusion criteria for published data were applied at the study level. Studies were considered eligible if they contained individual patient data satisfying three minimal criteria: (1) diagnosis of FMD classified as either ‘documented,’ ‘clinically established’ or ‘probable;’10 11 (2) FMD age at onset (either explicitly stated or derivable from comparing age and symptom duration entries); and (3) sex/gender were reported. Only reports written in English were included. We carefully considered whether to use the term ‘gender’ or ‘sex’ for this IPD meta-analysis. Since most of the data set relied on patient/clinician self-report of identified gender, we chose to use this term. Accordingly, we use the terms ‘women’ and ‘men’ throughout this report and recognise that transgender patients would need to be included separately, which is noted further in the discussion. We could not collect both gender and sex in this retrospective study.
Inclusion criteria for unpublished data were used to ensure that the individual data aligned with the published data set as much as possible and included: (1) patients with FMD as a primary diagnosis including any hyperkinetic or hypokinetic movement disorder and limb weakness; (2) adults and children; (3) diagnosed by neurologists with movement disorders training and derived from neurological settings. Exclusion criteria were: (1) other FND types (eg, functional seizures and sensory symptoms); (2) patients with comorbid additional movement disorders (eg, Parkinson disease); (3) patients with both FMD and functional seizures; (4) paroxysmal FMD (risk of overlap between episodic FMD and functional seizures).12
FMD phenotypes were classified into the following 10 categories, based on the most common FMD presentations: tremor, dystonia, gait disorder, weakness, jerks/myoclonus, mixed, facial symptoms, parkinsonism, other and unknown/not documented. ‘Mixed’ was included as a phenotype for cases with multiple phenotypes present at onset (eg, tremor and a gait disorder). ‘Facial symptoms’ encompassed facial dystonic spasms. ‘Other’ was included for other distinct FMD phenotypes. ‘Unknown/not documented’ accommodated cases which lacked phenotype characterisation. Adults and children were considered eligible. Harmonisation of criteria for published and unpublished data are described further in the online supplemental material.
Supplemental material
Study identification and search strategy
Published data were collected from an advanced PubMed search from 1968 to 2019 using the following key words: ‘functional’, ‘psychogenic’ or ‘conversion’; in combination with any of the following: ‘motor’, ‘movement’, ‘gait’, ‘tremor’, ‘dystonia’, ‘weakness’, ‘myoclonus’, ‘tic’, ‘facial’, ‘paralysis’, ‘paroxysmal’, ‘jerks’ and ‘parkinsonism.’ Titles that included ‘seizure’, ‘epilepsy’ or ‘epileptic’ were excluded to remove reports of dissociative/psychogenic seizures. All titles using the term ‘functional’ unrelated to FMD or movement disorders were removed. The search was expanded by including all relevant references. Furthermore, additional records were identified through hand search, using the above-mentioned keywords, by one of the investigators. The results from the literature review and the hand search were combined, removing all duplicates. Papers were then excluded if they were missing the requisite variables of interest (sex/gender or age at onset), only group-level data were available and not IPD, or any cases where a ‘possible’ level of diagnostic certainty was recorded. Corresponding authors of papers only reporting group-level data were contacted and invited to share their published data in IPD format. Details of the systematic review can be found in the online supplemental methods.
Unpublished data sharing
Unpublished data were shared from experts in the field via an initial invitation to the Movement Disorders Society FMD Study Group. Members were invited to contribute de-identified, unpublished data from their personal or research databases in compliance with their own institutional research ethics boards. See online supplemental methods for details of the included individual data sets.
Outcomes
The outcomes of interest were the distribution of the age at onset and whether this exhibited gender differences and/or differed by FMD phenotype, and whether gender moderated any differences between phenotypes. We additionally compared our data set to a similar recently published data set of functional seizures,8 another well-defined subtype of FND.
Statistical analysis
Descriptive statistics were reported using means (SD) or frequencies (%), where appropriate. Histograms of age at onset were generated for the entire sample, for each of the six main FMD phenotypes, and split by gender. A Doornik-Hansen omnibus test was used to assess multivariate normality of age at onset, which was repeated for men and women separately. To formally evaluate the association with gender and phenotype, a one-stage IPD meta-analysis was performed with age at onset as the dependent variable in a multilevel mixed-effects linear regression model. Gender (men vs women) and phenotype (tremor; dystonia; gait; weakness; jerks/myoclonus; mixed; other/unknown) were included as fixed effects, whereas country (28 levels) and data source (111 levels) were included as random effects, to account for between-source heterogeneity. Parkinsonism and facial symptoms were not included in the regression analysis due to small numbers. The model was rerun using standardised age of onset (subtracting the mean and dividing by the SD to force the mean as 0 and SD as 1 to report results on both the original and SD scale) to help interpret the magnitude of effect sizes. An interaction term between gender and phenotype was included in a second model to test for potential moderating effects, that is, to detect if the effect of gender on age at onset differs by phenotype. We also planned: (1) a statistical comparison between individuals with age at onset less than 16 and those with age at onset over 60 and (2) a visual comparison of age at onset and gender with the largest sample of dissociative seizures, a distinct subtype of functional neurological disorder.8 All statistical analyses were performed using Stata V.16.1 (StataCorp). An assessment of risk of bias was waived given the minimal data set of basic demographic data.
Results
The IPD selection process is summarised in figure 1. The systematic review is presented in the online supplemental material. The total data set consisted of 4905 individual FMD cases gathered from the systematic review and hand-search (n=878), shared published group-level data (n=570) and shared unpublished databases (n=3457). In total, there were 1448 individual FMD cases from all published sources included in the analysis. Unpublished IPD was collected from 33 separate international groups from 28 countries involving 70 authors (online supplemental figure 2 and online supplemental table 3).

Data selection process including published and unpublished individual patient data. AAO, age at onset; FMD, functional movement disorder; IPD, individual patient data.
Data characteristics
A summary of the descriptive statistics is provided in table 1. The cohort comprised 3558 (72.5%) female patients. The mean age at onset was 39.7 years (median 39.8). Three hundred and eighty-three cases (7.8%) of the sample were paediatric onset (age ≤16), and 10.7% (526 cases) of the sample had age at onset over age 60. The most prevalent phenotypes were mixed FMD (23.0%) and tremor (21.6%), and the least prevalent were facial symptoms and parkinsonism. There were 479 (9.8%) individuals classified either as ‘other’ or ‘unknown’ phenotype (online supplemental table 4). Almost half (42%) of the data set came from the USA. The remaining cases were from the Europe, Australia, Mexico and Canada. Countries in Africa, Asia and South America were under-represented (online supplemental material).
Descriptive summary statistics and one-stage individual patient data meta-analysis mixed-effects linear regression model for age of symptom onset, with ‘tremor’ and ‘female’ as the reference categories
Whole sample
The distribution of the age at onset of the entire sample is presented in figure 2A. The data approached a bimodal distribution with peaks between the ages of 16–22 and 35–45. The Doornik-Hansen test for multivariate normality indicated the data were significantly different to the normal distribution, which holds for men and women separately despite there being less skewness in the male group.

Histogram of FMD age of onset for the whole sample (n=4905) (A) and separated by the six main presenting FMD phenotypes (B). FMD, Functional movement disorder.
Gender differences
When controlling for FMD phenotype (and heterogeneity between data sources within countries), men demonstrated a significantly older mean age at onset as compared with women (41.0 years vs 39.1 years) (table 1). Women represented greater than 64% of the sample across all age groups, with a tendency for more cases in the younger age groups (age 10–50) (figure 3A,C). By comparison, the age at onset of functional seizures in women, analysed from the Cognitive Behavioural Therapy versus Standardised Medical Care for Adults with Dissociative Non‐Epileptic Seizures trial database of 698 individuals, produced a different distribution with a clear early peak in late adolescence, tapering into adulthood. This is in contrast to a similar frequency across the lifespan in men (figure 3B).8

Histograms showing age of onset distribution by gender in (A) the whole sample of this study (n=4905) compared with (B) the previously published UK sample of functional seizure patients (n=698).8 3C shows the comparison of FMD (red) and functional seizure (FS, green) patients displayed as percentage women with CIs. Figure adapted from Goldstein et al.8 FMD, Functional movement disorder.
Phenotype differences
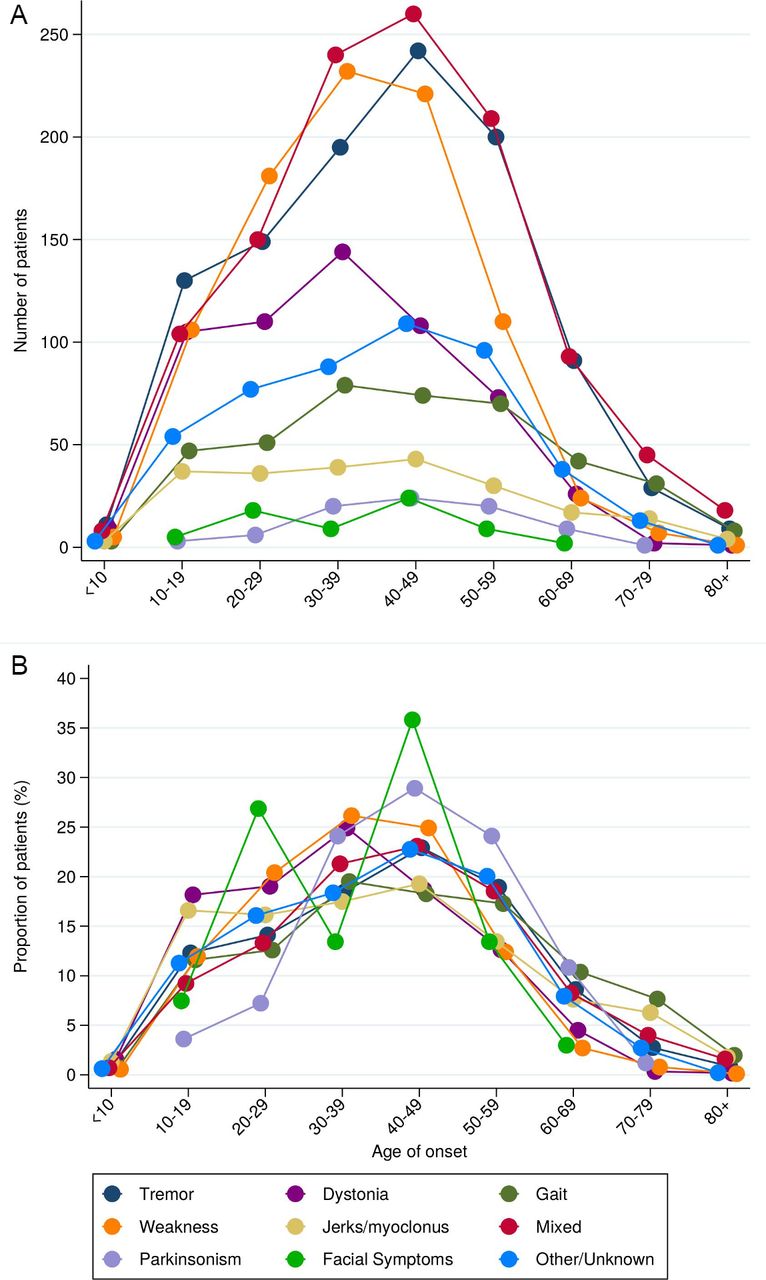
The mean age at onset was significantly different across phenotypes when controlling for gender and data source within country random effects (table 1). Compared with functional tremor, the mean age at onset of functional dystonia was younger by 4.3 years (95% CI 2.7 to 6.0 years, p<0·001), functional weakness was younger by 3.7 years (95% CI 2.1 to 5.3 years, p<0.001), while functional gait disorder presented with a significantly older mean age at onset, by 3.2 years (95% CI 1.4 to 5.0, p<0.05). The distribution of phenotypes (including ‘other’) followed roughly the same trajectory (ie, non-normal distribution with a peak in midlife) regardless of the number of cases (figure 4). Additionally, some phenotypes showed a more prominent second, early peak in the adolescent/early 20s, including dystonia, jerks/myoclonus and gait disorders (figures 2 and 4). Using a categorical division between young and old age at onset (‘under 16’ and ‘over 60’), no significant associations were found for each phenotype (online supplemental table 1).

(A) Connected dot plots showing age of onset in 10-year age bands by phenotype using number of patients in each decile compared with (B) proportion of patients within each decile within each phenotype.
Gender and phenotype interactions
Differences in age at onset in relation to both gender and phenotype are shown in figure 5. Although all cases more commonly occurred in women with proportions above 70%, compared with other phenotypes, parkinsonism (51.8%) and jerks/myoclonus (63.7%) were seen relatively more often in men, and parkinsonism also tended to occur slightly older (44.6±12.9 years). Facial symptoms and dystonia occurred considerably more often in women (83.6% and 78.4%, respectively). However, when including an interaction term between phenotype and gender into the multilevel mixed model, this was not significant (p=0.7513).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean age of onset compared with proportion of women by clinically relevant phenotype. The dashed horizontal line represents the point where the men: women ratio would be equal (50%).
Discussion
This large individual patient data meta-analysis primarily provides detail on age of onset and gender for FMD and its phenotypes with unprecedented resolution compared with previous studies. We acknowledge that age of onset curves and gender form a limited data set on which to draw nosological conclusions. Nonetheless we think this data does offer some support for considering FMD both as a single entity but also one in which distinguishable phenotypes have validity. FMD is defined clinically through common historical features and positive signs on examination including variability and distractibility, but phenomenological differences have contributed in part to segregating FMD into separate disorders. Combining a large data set across phenotypes shows that FMD subtypes also share common characteristics (eg, similar shaped curves of age at onset) and have different epidemiological features (eg, 10-year difference between the mean age at onset of functional dystonia and functional gait disorder).
These results confirm previous much smaller studies demonstrating that FMD is more common in women (73%–75%) and symptom onset occurs most commonly in midlife.2 13 14 Given the probable under-representation of paediatric and elderly cases in the sample, we cannot be confident that this ratio is stable across the lifespan in FMD, although the same gender ratio (71%–74%) has been reported in paediatric case series.4 6 Prior studies have found gender differences among FMD phenotypes, including higher rates of dystonia in women (84%),6 10 15 or axial myoclonus in men.7 Of note, our study did not differentiate between axial and other types of myoclonus. Women are well-established to be more common than men in fibromyalgia, chronic fatigue syndrome and other functional disorders including irritable bowel syndrome.16 This gender difference has been attributed to several factors including the higher reported incidence of anxiety, depression and trauma in women,17 and that women are more likely to present to health services. Gender influences on the behaviour of the community, clinicians and patients is a social and psychological modifier of disease presentation, and a factor in determining how, when and why a person accesses medical care as well as what diagnoses they receive.16 However, autoimmune disorders such as multiple sclerosis and systemic lupus erythematosus are also more frequent in women highlighting the important role of biological sex differences, alongside gender differences.
Mixed FMD was the most common phenotype, followed by tremor, weakness and dystonia. Patients with FMD commonly display multiple phenotypes, both at a cross-sectional point in time (eg, at onset) and over time.18 19 Importantly, our results show that all phenotypes share a similar distribution (figure 4B) which, together with the frequency of ‘mixed’ phenotype, further supports FMD as a unitary disorder. Indeed, distinguishing between FMD phenotypes using clinical and demographic factors is challenging.18 Paroxysmal FMD and functional seizures can overlap. Our study excluded these cases for practical purposes, but it would be important to include these, as well as FMD occurring in comorbid neurological disease, in subsequent efforts to distinguish FND subtypes.
The onset of FMD occurs in midlife, ranging from 35 to 45 years, although this probably underestimates paediatric and elderly cases.20–23 The clustering of FMD mean age at onset in midlife and a second peak in late adolescence is a new finding (ie, a non-normal distribution). Our results confirm that functional dystonia has a younger age at onset and is more often seen in women, and a relatively higher proportion of men develop functional jerks and parkinsonism than other phenotypes (figure 5), although both still more commonly occur in women. A gender difference between different types of FMD was recently reported in a series of 196 patients with similar results.6
Another advantage of the large data set is the ability to specifically look at paediatric and elderly onset cohorts. The most common phenotype in both groups was tremor followed by dystonia in younger patients and gait disorders in older patients, reflecting previous paediatric and elderly case series from which a portion of our data are drawn.2 21 22 Our analysis found no association between phenotype and age at onset or gender. This may reflect stability of FMD across the lifespan, supporting the view of a unitary diagnosis rather than a phenotype-based diagnosis.
We found different distributions of age at onset of FMD and functional seizures, two well-described FND phenotypes, which can overlap phenomenologically but tend to be clinically managed in segregated pathways.12 In women, functional seizures have a younger modal age at onset in the late teens and a mean in the late 20s, whereas men with functional seizures show a stable frequency of age at onset across the lifespan.8 This comparison also raises the possibility that, despite shared predisposing and precipitating factors in FMD and functional seizures, there may be important differences. Women may experience disproportionate trauma or adverse life events at younger ages than men, predisposing them to dissociation and developing functional seizures earlier in life, whereas physical injury or illness that may precipitate FMD24 may be more skewed towards older age groups.25
The most significant limitation of this study is that two-thirds of the IPD was derived from unpublished databases. This approach, however, enabled us to augment the data set by over 3000 cases. Harmonising published and unpublished data can result in underestimation of both eligible studies and individual cases and required efforts to try to ensure that true FMD cases were captured as reliably as possible. The clinical diagnostic criteria are shifting in the field toward the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition DSM-5, which does not reflect the older diagnostic criteria we specified in our literature search. However, as long as we could be reasonably certain that all cases included were FMD, given the bare minimal data set requested, there is value in this analysis, and in particular, because we collapsed across phenotypes. We relied on contributors to ensure that their data were accurate and that diagnostic clinical criteria were applied correctly, recognising that newer diagnostic criteria are routinely used in the clinical and may have also been used. We also relied on contributors to follow the inclusion criteria and ensure there were no duplications in their data. In addition, we did not request the timeframe for data collection nor if cases were consecutive as we felt these requirements would have substantially reduced the size of the data set. Although these cases were drawn from movement disorder specialists with a clinical interest in FMD, phenotypic characterisation can be challenging in this population. However, ‘mixed’, ‘other’ and ‘unknown’ categories, behaved as the more readily diagnosable phenotypes (eg, tremor), suggesting that diagnosis in these categories was as reliable.
These data are drawn from subspecialty clinic-based samples and do not reflect population-level epidemiological data. Furthermore, movement disorders clinics often see more complex or persistent FMD cases, underestimating mild or remitting FMD, thus recruitment bias may also influence the data. However, studying the epidemiology of FMD at a population level is inherently problematic since it normally requires secondary care expertise to make the diagnosis. FMD has high rates of comorbidity with other functional symptoms (including functional seizures) and this may have led to distortions in the data. There was an under-representation of paediatric and elderly cases, and data in these groups is less certain. We compared our case series data to the published functional seizures data set drawn from an interventional study. The systematic review was conducted in a single database, thus potentially under-representing published cases. The geographical distribution of this sample was heavily weighted to North America and Europe, however transcultural studies have not shown significant phenotypic differences in FMD.26 27 Factors determining age at onset and gender could potentially vary geographically. A post-hoc analysis using developed/developing country as a covariate in the main regression model did not impact the outcome.
Since we relied on retrospective data, we could only describe reported gender (from both published and unpublished sources) rather than both gender and biological sex. Most studies did not clarify whether sex or gender are reported so our study almost certainly conflates the two. Non-binary or transgender patients were not considered separately in our study. We are aware of four transgender patients in the data set and although unlikely to alter the conclusions, it is an important distinction that needs to be properly accounted for in any prospective data collection.
In summary, our data gives unprecedented resolution on the basic epidemiology of FMD which occurs across the lifespan but peaks in midlife with varying effects of gender on age at onset and phenotype. We do not wish to claim that our limited variable data set necessarily provides unique or novel insights in to the disorder. We do not think it can resolve, for example, whether this is a unitary disorder. Nonetheless we do see some support for ‘lumping’ FMD as a unitary disorder, at least in certain situations, on the ground that the FMD subtypes age of onset and gender profiles appear to have more in common with each other than with the ‘comparable’ movement disorder, for example, parkinsonism, tremor, and dystonia. However, with respect to the concept of ‘functional neurological disorder’ we have shown, visually at least, some potentially important differences between the basic epidemiology of FMD and functional seizures which generally appear larger than those between individual movement disorder phenotypes. Finally, there are statistical signals that not all phenotypes are equal with dystonia, myoclonus and gait disorder especially standing out.
This study provides a precedent for synthesising data across subphenotypes in functional disorders, which may reveal common, relevant underpinnings of FND worthy of hypothesis testing. Future research should follow patients longitudinally to observe shifting phenotypes over time and determine the association between treatment outcomes and phenotypes and other biomarkers. Finally, our study also offers utility for health services planning and sets a new benchmark for international collaboration in FND.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University Health Network Research Ethics Board reference number #19-5901. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @sarahlidstone, @ercolitommaso, @jonstoneneuro
Correction notice This article has been corrected since it first published. Affiliations have been added to the Collaborator section. In addition, it has been made open access under a CC BY licence. 19th May 2023.
Collaborators The FMD GAP Study Group includes the following authors: Omar Ahmad, Royal North Shore Hospital, Sydney, Australia; Sepideh Akbaripanahi. National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland, USA; Alberto Albanese, Department of Neurology, IRCCS Humanitas Research Hospital, Rozzano Milano, Italy; Selma Aybek, University Hospital Inselspital, Bern University, Bern, Switzerland; José Fidel Baizabal-Carvallo, Department of Sciences and Engineering, University of Guanajuato, Leon, Mexico; Peter J. Beek, Department of Human Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands; Kailash P. Bhatia, FRCP University College London, Institute of Neurology, Department of Clinical and Movement Neuroscience, Queen Square, London, UK; Verónica Cabreira, Department of Neurology, Centro Hospitalar Universitário de São João and Faculty of Medicine University of Porto, Porto, Portugal; Alan J Carson, Center for Clinical Brain Sciences, University of Edinburgh, Edinburgh, UK; Anna Castagna, IRCCS Fondazione Don Carlo Gnocchi Onlus, Milano, Italy; Russell C. Dale, Kids Neuroscience Centre, University of Sydney, Sydney, Australia; Carlo Dallocchio, Neurology Unit, Department of Medical Area, Pavia, Italy; Giovanni Defazio, Department of Medical Sciences and Public Health, University of Cagliari, Italy; Bertrand Degos, Department of Neurology, Avicenne University Hospital, Sorbonne Paris Nord University, Bobigny, France; Benedetta Demartini, Dipartimento di Scienze della Salute, Università degli Studi di Milano, Milano, Italy; Günther Deuschl, Department of Neurology, Christian-Albrechts University, Kiel, Germany; Galina Diukova, Loginov Moscow Clinical Scientific Center, Moscow, Russia; Kevin R. Duque, Department of Neurology and Rehabilitation Medicine, Gardner Family Center for Parkinson’s Disease and Movement Disorders, University of Cincinnati, Cincinnati, Ohio, USA; Mark J Edwards, Neuroscience Research Centre, St George's University of London, Cranmer Terrace, London, UK; Steven A. Epstein, Georgetown University School of Medicine and MedStar Health, Washington DC, USA; Alberto J. Espay, Department of Neurology and Rehabilitation Medicine, Gardner Family Center for Parkinson’s Disease and Movement Disorders, University of Cincinnati, Cincinnati, Ohio, USA; Stewart A Factor, Jean and Paul Amos Parkinson's Disease and Movement Disorders Program, Emory University, Atlanta, Georgia, USA; Beatrice Garcin, Department of Neurology, Avicenne University Hospital, Sorbonne Paris Nord University, Bobigny, France; Christian Geroin, Neurology Unit, Movement Disorders Division, Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, Verona, Italy; Muriel Hagenaars, Utrecht University, Utrecht, The Netherlands; Mark Hallett, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland, USA; Thomas Hassa, Lurija Institute for Rehabilitation and Health Sciences, Allensbach, Germany; Anhar Hassan, Mayo Clinic, Rochester, Minnesota, USA; Lorena D. Herbert, University of Texas Southwestern, Dallas, Texas, USA; Samantha K. Holden, University of Colorado Anschutz Medical Campus, Denver, Colorado, USA; Joseph Jankovic, Parkinson's Disease Center and Movement Disorders Clinic, Baylor College of Medicine, Houston, Texas, USA; Richard A. Kanaan, Department of Psychiatry, University of Melbourne, Austin Health, Heidelberg, Victoria, Australia; C.A. (Lianne) Kempe, Department of Mood Disorders, PsyQ, Parnassia Groep, The Hague, The Netherlands; Maja Kojovic, Department of Neurology, University Clinical Centre Ljubljana, Slovenia; Katie Kompoliti, Department of Neurological Sciences, Rush University Medical Center, Chicago, Illinois, USA; Vladimir S. Kostić, School of Medicine, University of Belgrade, Belgrade, Serbia; Kevin Kyle, Departments of Neurology and Psychiatry, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA; Kathrin LaFaver, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; Anthony E. Lang, Edmond J. Safra Program in Parkinson's Disease, the Morton and Gloria Shulman Movement Disorders Clinic, Toronto Western Hospital and the Division of Neurology, University of Toronto Lindsey MacGillivray PhD, MD Department of Psychiatry, University Health Network, University of Toronto, Canada; Davide Martino, Department of Clinical Neuroscience, Cumming School of Medicine, University of Calgary, Calgary, Canada; João Massano, Department of Neurology, Centro Hospitalar Universitário de São João and Faculty of Medicine University of Porto, Porto, Portugal; Carine W. Maurer, Stony Brook University School of Medicine, Stony Brook, New York, USA; Laura McWhirter, Centre for Clinical Brain Sciences, University of Edinburgh, Edinbugh, UK; Raja Mehanna, University of Texas Health Science Center at Houston and McGovern Medical School, Houston, Texas, USA; Francine Mesrati, Neurophysiology Department, Hospital Pitié Salpêtrière, AP-HP, Paris, France; John C. Morris, Washington University School of Medicine, St. Louis, Missouri, USA; Glenn Nielsen, Neuroscience Research Centre, Institute of Molecular and Clinical Sciences, St Georges University of London, London, UK; Anastasia Obukhova, I.M. Sechenov First Moscow State Medical University, Moscow, Russia; Sanjay Pandey, Govind Ballabh Pant Institute of Postgraduate Medical Education and Research, JLN Marg, New Delhi, India; David L. Perez, Departments of Neurology and Psychiatry, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA; Igor Petrović, Medical Faculty, University of Belgrade, Serbia; Seth L. Pullman, Columbia University Irving Medical Center, New York, New York, USA; Angelo Quartarone, Department of Biomedical Science and Morphological and Functional Images, University of Messina, Messina, Italy; Karin Roelofs, Radboud University, Behavioural Science Institute and Donders Institute for Brain, Cognition and Behaviour, Nijmegen, The Netherlands; Anette Schrag, Queen Square Institute of Neurology, University College London, London, UK; Yury Seliverstov, Research Center of Neurology, Moscow, Russia; Tereza Serranová, Charles University in Prague, 1st Faculty of Medicine and General University Hospital, Prague, Czech Republic; Ulf Søgaard, Psychiatric Research Unit, Slagelse, Denmark; Petr Sojka, Department of Psychiatry, Faculty of Medicine, Masaryk University Brno and University Hospital Brno, Brno, Czech Republic; Maria Stamelou, Parkinson’s Disease and Movement Disorders Department, Hygeia Hospital, Athens, Greece. European University of Cyprus, Nicosia, Cyprus. Philipps University, Marburg, Germany; Christopher D. Stephen, Movement Disorders Unit, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts, USA; John F. Stins, Department of Human Movement Sciences, Faculty of Behavioural and Movement Sciences, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands; Michele Tinazzi, Department of Neurosciences, Biomedicine and Movement, University of Verona, Verona, Italy; Aleksandra Tomić, Neurology Clinic, Clinical Center of Serbia, and Faculty of Medicine, University of Belgrade, Belgrade, Serbia; Anabela Valadas, Serviço de Neurologia, Centro Hospitalar Universitário Lisboa Norte, Lisbon, Portugal; Valerie Voon, Department of Psychiatry, University of Cambridge, Cambridge, UK; Jeff L. Waugh, University of Texas Southwestern, Dallas, Texas, USA; Allan D Wu, University of California Los Angeles, Los Angeles, California, USA.
Contributors SL—guarantor of overall content, conceptualisation, data curation, methodology, project administration, supervision, data validation, writing (original draft, review and editing). MC-P—data curation, project administration, data validation, writing (original draft, review and editing). TE—data curation, project administration, writing (original draft, review and editing). EJR—formal analysis, writing (original draft, review and editing). JS—conceptualisation, methodology, supervision, data validation, writing (original draft, review and editing). FMD-GAP Study Group—data sharing, feedback on initial manuscript, editorial, critical appraisal.
Funding SL and MC-P were supported by an anonymous donation to the Toronto Western Hospital Movement Disorders Clinic. JS was supported by an NHS Scotland NRS Career Fellowship.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographical or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests JS reports royalties from UpToDate for articles on FND and runs a free self-help website for people with FND. He carries out independent expert medicolegal work including in relation to FND. He is secretary of the FND society and on the medical advisory board for FND Hope and FND Action.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.