Article Text

Abstract
Preventive medications reduce migraine frequency and severity, and improve migraine-specific quality of life. Recent evidence also suggests that these same medications enhance the patient’s response to acute migraine therapies, and may also reduce the likelihood of developing chronic daily headache. However, many patients who should receive or be offered preventive treatment are not. Most patients can be successfully managed when patient and physician expectations are realistic and aligned, the selection of preventive medications is individualised, and the initiation and titration strategy is appropriate and carefully followed. Rational combinations of preventive medications may also be useful. This review provides an evidence and experience-based approach to the preventive treatment of migraine.
Statistics from Altmetric.com

An illustrative case
A 32-year-old sales executive with a 20-year history of episodic migraine developed increasingly frequent attacks over 12 months. Her average monthly frequency was five attacks, each of which lasted for 18 hours, followed by a “postdromal” period of fatigue and lethargy for up to 24 hours. For each attack, she was using ibuprofen 400 mg when the pain became moderate in severity, repeating the dose in four hours if needed. She also had insomnia and mild situational anxiety associated with work-related stress. She had no comorbid illnesses and took no other medications. Her general physical and neurological examination was normal except for a body mass index of 28 and mildly raised systolic blood pressure (144 mmHg). Preventive treatment is indicated, as is more optimal acute management of her attacks. For the latter, a higher dose of ibuprofen or naproxen sodium should be used if there is an adequate period of time during which the pain is mild. However, if this is not effective, or the patient often awakens with moderate or severe pain, progresses rapidly from mild to moderate pain, or does not have a mild p0ain phase, a triptan should be used as soon as possible as first-line acute therapy. Non-pharmacological management might include biofeedback and relaxation therapy if available and feasible; this may relieve some of her stress-related anxiety and contribute to a reduction in attack frequency and/or severity. She should avoid medications which have a high potential for weight gain if possible. Topiramate or a beta-blocker would be a reasonable first choice. Each option should be presented to the patient, the advantages and disadvantages of each should be discussed, especially the adverse effect profile. She should be encouraged to assist in the drug selection. A low dose should be started, and the dose titrated by weekly increments, until she begins to notice a benefit. She should keep a daily diary that captures headache frequency, severity, associated symptoms, duration, headache-related disability and acute headache medications. If dose-limiting adverse effects occur before an effective dose is achieved, coenzyme Q10 100 mg three times daily or petasites (butterbur) 75 mg twice daily could be added, or a small dose of either a beta-blocker (if topirmate had been started) or topiramate (if a beta-blocker had been started). Once her headaches are well controlled for 3–6 months, consider slowly tapering one medication at a time.
Migraine is a highly prevalent neurological disorder that affects about 13% of the population in most western industrialised societies. It is one of the leading causes of health-related disability worldwide, it is an independent risk factor for both silent and symptomatic ischaemic stroke and ischaemic cardiovascular disease, and up to 14% of sufferers progress to a more disabling chronic form of the disorder (chronic migraine).1–4 It has a variety of clinical manifestations including headache, nausea, vomiting, heightened sensitivity to environmental stimuli such as light, sound and odours, nasal sinus pressure, neck pain/discomfort, and transient neurological symptoms and signs referred to as the migraine aura. Aura occurs in up to 30% of migraineurs and may involve the visual, somatosensory, language or motor systems. Most patients with migraine with aura also have migraine without aura, and the proportion of attacks associated with aura varies greatly from a few in a lifetime to most attacks.
The treatment of migraine involves both acute and preventive drugs, and non-pharmacological strategies. Preventive treatment is necessary when the migraine attacks are unacceptably frequent, prolonged, severe, unresponsive to acute medication, or associated with hemiparesis or prolonged aura. It is therefore designed to reduce the frequency, duration, and/or severity of the attacks. In addition, preventive treatment often makes migraine attacks more responsive to acute migraine therapies, reduces migraine associated disability, improves the patient’s ability to function, and decreases healthcare costs and use of healthcare resources.
Although there are many therapeutic agents and other approaches that have been used for migraine prevention, there is a robust evidence base for only eight drugs and two non-pharmacological approaches;5 those with the best documented efficacy are some beta-blockers, flunarizine, divalproex sodium or valproate, topiramate, methysergide and amitriptyline. The decision in clinical practice as to which of the options is optimal is based on the strength of the evidence for efficacy, the physician’s clinical experience, the drug’s adverse event profile, the patient’s preferences, headache subtype (antiepileptic drugs are generally preferred in migraineurs with aura), the presence or absence of coexisting conditions and comorbid disorders, and the potential for childbearing. Specifically, divalproex sodium and valproate are absolutely contraindicated during pregnancy because of the increased risk of neural tube defects. As unplanned pregnancies are not uncommon, these drugs are generally not used in young women of childbearing potential.
The clinician should be very mindful of any comorbid and coexistent conditions in patients with migraine, to maximise the potential for treatment efficacy and minimise the potential for adverse effects. Comorbid illnesses are those that occur more frequently in association with a specific disorder than would be expected by chance in the general population. In contrast, coexistent illnesses occur together in the same person at a rate that would be expected by chance. The comorbid illnesses associated with migraine that influence its management include depression, anxiety disorders, epilepsy and stroke. Coexistent illnesses or disorders that occur commonly in the general population that will influence the selection of preventive drugs used for migraine include diabetes mellitus, hypertension and obesity.6 Pregnancy also influences the choice of preventive agent.
MECHANISM OF ACTION OF MIGRAINE PREVENTIVE DRUGS
Despite the dramatic advances over the past several decades in our understanding of the neurobiology of migraine, there is no animal model for migraine prevention and only methysergide was developed specifically for the preventive treatment of migraine, and that was several decades ago. Most drugs used for migraine prevention were either discovered to be effective by serendipity (beta-blockers) or because of educated guesses using drugs designed to treat diseases with an overlapping pathophysiology (epilepsy, depression). Therefore, one should not be surprised that the mechanism of action of migraine preventive drugs has not been clearly elucidated. However, recent animal studies suggest that several of the drugs may work through a common mechanism; topiramate, valproate, propranolol, amitriptyline and methysergide all have a dose-dependent effect in raising the threshold for initiation of cortical spreading depression.7 Cortical spreading depression is currently widely considered to be the physiological substrate underlying the migraine aura and, although controversial, is also felt by some authorities to underlie migraine without aura as well. Interestingly, this same study7 also demonstrated that the suppression of cortical spreading depression increased over time, which provides a scientific rationale for the clinical observation that the efficacy of these drugs in clinical practice depends on dose-titration and an adequate duration of treatment.
INDICATIONS FOR AND USE OF PREVENTIVE TREATMENT
Epidemiological studies suggest that that about one third of migraineurs need preventive treatment, but only 3–13% of all migraineurs currently use preventive therapy to control their attacks.8 While recent data suggest that preventive treatment reduces the risk of progression to chronic migraine, definitive evidence must await long-term prospective observational studies.8 It is also not clear whether preventive medication reduces the risk of adverse cardiovascular events such as ischaemic stroke and heart disease. Therefore, currently, the treatment goals of preventive medications and non-pharmacological strategies include the following:
reduce attack frequency, severity and duration
improve responsiveness to acute headache therapies
improve function and reduce disability
reduce overall cost associated with migraine treatment.
As a component of the comprehensive approach to migraine prevention, all patients with migraine should be educated about potential triggers for attacks and guided on how best to avoid them.
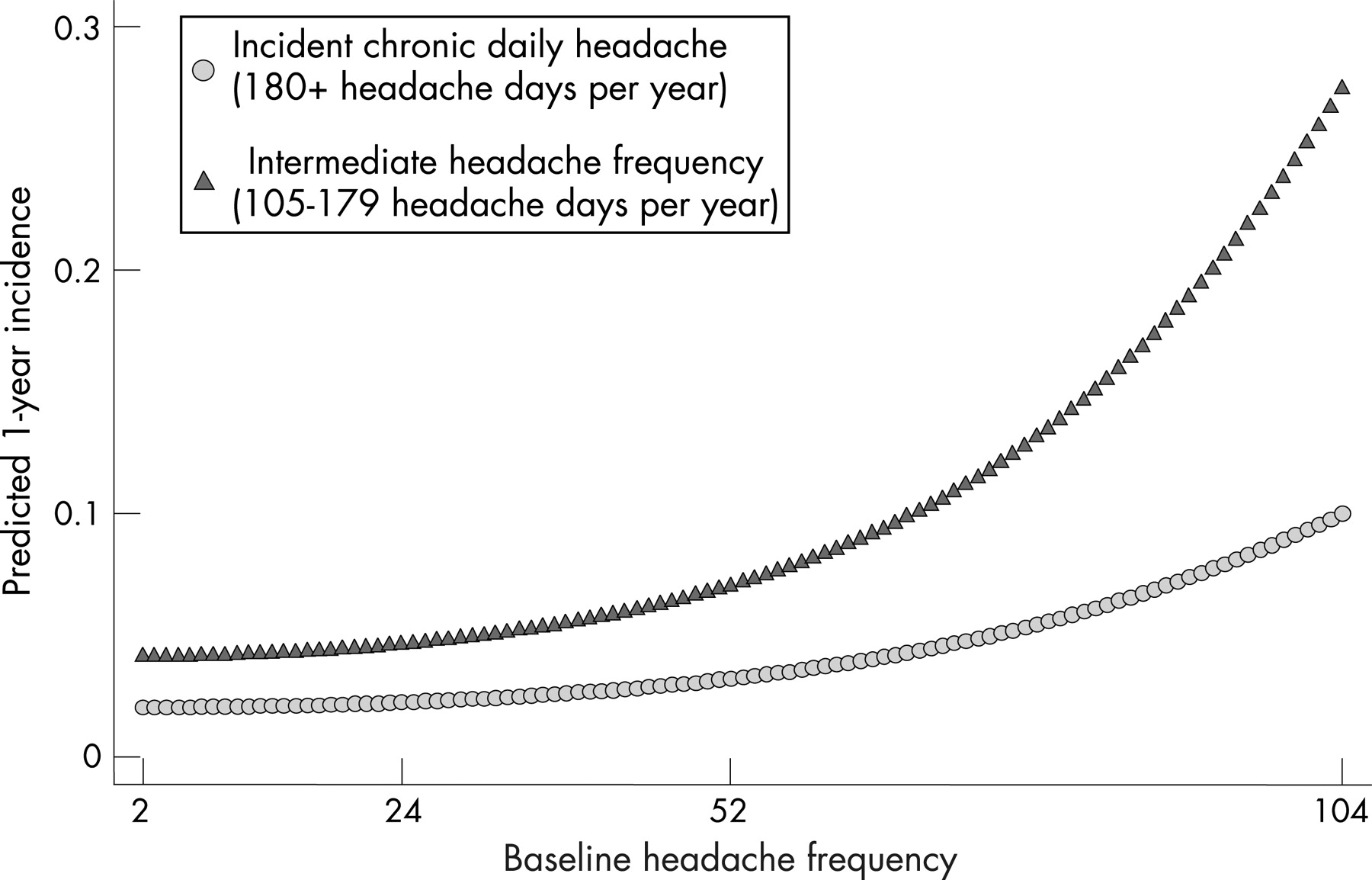
Guidelines that define the indications for preventive drug treatment have been developed in the USA and Europe9, 10 (table 1). In general, patients who experience one or more migraine attacks per week should be offered preventive therapy because recent evidence suggests that progression to chronic daily headache increases significantly at higher frequencies (fig 1).

PRINCIPLES OF PREVENTIVE THERAPY
The success of preventive therapy rests as much on the strategy employed when initiating and titrating the medications, and establishing realistic patient expectations, as it does on which drug is actually selected. The following principles, while not evidence-based, reflect practical clinical experience and can lead to a better outcome:
Minimise adverse effects
Start the chosen drug at a low dose (for example, 10 mg amitriptyline daily) and increase slowly, perhaps every 1–2 weeks by the same dose (for example, 10 mg amitriptyline week 1, 20 mg week 2–3, etc) until therapeutic effects develop.
Setting and reaching target dose
Set initial target dose (for example, 30 mg amitriptyline) advising patient to stop earlier if partial efficacy or adverse events develop. The maximal dose is reached when efficacy is optimal or adverse effects become intolerable.
Efficacy takes time and accumulates over time
Give each treatment an adequate trial of at least six weeks at the maximally tolerated dose; remember, the six-week clock begins only after this dose is achieved. However, based on experience and randomised trials, the full benefit of a drug may not be realised until six months have elapsed from the time of achieving this dose. A graph illustrating the time course and usual response to preventive migraine therapies may be helpful for the patient, and improve compliance (fig 2).

{kind=link}
{kind=link}
Setting expectations for success and adverse effects
Success is generally defined as a 50% reduction in attack frequency, a significant decrease in attack duration, or an improved response to acute medication. Unless advised what to expect, patients understandably interpret the term “prevention” literally and anything less than complete relief of attacks is equated with “failure” of the drug.
The development of adverse effects varies greatly from patient to patient and cannot be predicted on an individual basis. The most common adverse effects and their likely frequency should be discussed with patients, and rare but serious idiosyncratic adverse effects must also be discussed. Most adverse effects are self-limiting and dose-dependent, and patients should be encouraged to try to tolerate any early adverse effects that may develop when a new medication is started.
Selecting and maximising drug choice
A drug may be selected (for example, divalproex sodium/valproate in a migraineur with epilepsy) or avoided (beta-blocker in a migraineur with asthma) on the basis of the presence of a comorbid or coexistent illness. Care should be taken however not to under-treat a comorbid disorder by trying to treat two different conditions with one drug.6 For example, a low-dose tricyclic antidepressant may effectively treat migraine but not comorbid depression. In such a case, optimally treating both conditions may require two separate medications, especially because adverse effects are often inevitable and dose-dependent with tricyclic antidepressants, and selective serotonin and/or norepinephrine reuptake inhibitors are generally considered first-line agents for the treatment of depression. Drugs that are commonly associated with weight gain (for example, divalproex sodium/valproate, amitriptyline) are not the best first choices in an obese patient or one with a disease that may be exacerbated by weight gain (for example, diabetes mellitus, hypertension, cardiovascular disease).
Avoid, if at all possible, preventive drugs in pregnant or lactating women. In addition, because migraine is most prevalent in women of childbearing age, the potential for adverse fetal effects should be discussed and drugs used for prevention should be stopped if at all possible when women are trying to conceive. Drugs with unequivocal teratogenic effects (for example, divalproex sodium/valproate) should be avoided in women of childbearing age.
Re-evaluate therapy and, if possible, taper or discontinue the drug after a sustained period of remission (perhaps six months).
Maximise adherence to medication
A surprising proportion of patients do not comply with preventive medications recommended and prescribed by their physicians. Educating patients about titration schedules, expectations for success and adverse effects is critical for encouraging adherence. In particular, with drugs of equivalent efficacy, patients often select preventive medications based on the adverse effect profiles they most want to avoid. Therefore, patient preference must be taken into account as patients are more likely to be compliant with a medication they helped select.
PREVENTIVE MEDICATIONS AND STRATEGIES: EVIDENCE AND EXPERIENCE-BASED RECOMMENDATIONS
A myriad of therapeutic agents and approaches have been used and tested in clinical trials for the preventive treatment of migraine. Recently, an evidence-based practice parameter has been developed by the Quality Standards Subcommittee of the American Academy of Neurology.5 This provides an updated literature review and recommendations from a previous guideline published in 2000 and was based on 30 additional, randomised, double-blind, controlled clinical studies that had been published from 2000–7. The practice parameter concluded that there is currently level-I evidence to support the use of eight drugs available in the USA (topiramate, divalproex sodium/sodium valproate, amitriptyline, metoprolol, propranolol, timolol and extracts of butterbur (the plants commonly referred to as butterbur are found in the daisy family Asteraceae in the genus petasites)), and two non-pharmacological approaches (relaxation therapy and biofeedback). Methysergide is also effective for migraine prevention, but is limited in practice because of lack of availability and the associated severe adverse effects.
The efficacy and safety of several other therapies and all the drugs that have been tested were grouped according to the evidence, with corresponding recommendations (table 2). However, this guideline did not include drugs that were not available in the USA, but are available and used widely in other countries in North and South America and Europe (for example, flunarizine, pizotifen). Therefore, based on the evidence, availability and clinical experience, first-, second- and third-line medications are listed in tables 3–5.
BEHAVIOURAL TREATMENTS
Behavioural treatments are classified into three broad categories: relaxation training, biofeedback therapy, and cognitive-behavioural training (stress-management training). They have all been shown to be effective in the preventive management of migraine, and have been directly compared and integrated with drug treatments. For example, popranolol and amitriptyline confer additional clinical benefits when added to thermal biofeedback, relaxation, cognitive-behavioural therapy or EMG biofeedback.
Behavioural treatments are options for headache sufferers who have one or more of the following characteristics:
patient preference for non-drug interventions
poor tolerance to drug treatments
medical contraindications to drug treatments
insufficient or no response to drug treatments
pregnancy, planned pregnancy or breast feeding
history of long-term, frequent, or excessive use of analgesics or acute medications that can aggravate headache problems
significant stress or poor stress-coping skills.
There is insufficient or conflicting evidence to support the use of acupuncture, cervical manipulation and mobilisation, hypnosis, transcutaneous electrical nerve stimulation (TENS), occlusal adjustment, and hyperbaric oxygen for migraine prevention.
COMBINATION THERAPY
There is little evidence to support the use of multiple (⩾2) preventive treatment drugs for migraine prevention. Despite this, combination therapy is a useful and frequently employed strategy in clinical practice, especially in patients who seem to easily develop adverse effects, or for those who are not optimally controlled on one drug. Combination therapy is also often used in migraineurs who have “transformed” or developed chronic migraine—a more recalcitrant form of migraine where patients experience more than 15 days of headache each month and more than eight migraine attacks each month. For example, an antiepileptic drug can be combined with a beta-blocker or tricyclic antidepressant. In this fashion, the individual drugs can be kept at low dosage, minimising adverse effects, but taking advantage of a potentially synergistic effect between two medications with different mechanism(s) of action. One can also combine a conventional preventive medication with one or more of the treatments that may fall into the “alternative or complementary” medicine group, such as riboflavin, coenzyme Q10, butterbur, and/or magnesium. There are placebo-controlled studies which support the use of each of these alternative therapies, they are invariably very well tolerated, and there may be a synergistic or enhanced placebo response with their combined use.
MENSTRUAL-RELATED MIGRAINE
Preventive therapy may eliminate all headaches except those associated with menses. An alternative strategy is short-term prophylaxis just during a defined period of increased vulnerability. As menstrual-related migraine typically occurs at the same time each month or in association with symptoms that herald its occurrence, the timed use of medications is appropriate. Women who are already using preventive medication and continue to have menstrual-related migraine can increase the medication dose before their menses. Women who do not use preventive medicine or have migraine mainly with their menses can just be treated perimenstrually with short-term prophylaxis. Of course, regular periods and a predictable relation between the attacks and the periods are essential for this strategy to succeed. Drugs that have been used perimenstrually for short-term prophylaxis include non-steroidal anti-inflammatory drugs, ergotamine, dihydroergotamine, methysergide, methergine, triptans and magnesium (table 6).
Practice points
Preventive treatment reduces migraine frequency and may prevent progression to chronic migraine.
Initiate preventive medication in patients having one or more migraines per week, or using acute headache medication ⩾2 days/week.
Individualise drug selection by using a preventive that may treat a comorbid or coexistent illness/disorders and by avoiding a drug which will exacerbate another underlying condition.
Select preventive drug based on evidence; use first-line therapies when possible.
Establish expectations for a realistic response (in general, 50% of patients have at least a 50% reduction in migraine frequency), cumulative benefit over time, and the need for patience during the dose titration phase.
When there is a partial but suboptimal response, or dose-limiting adverse effects, combining two preventive drugs with different mechanisms of action may be useful.
The decision to taper and discontinue a preventive medication is for the patient. However, once excellent control has been established for a period of at least six months, then an attempt to taper the medication is reasonable, especially as the natural history of the disorder is to remit over time.
Acknowledgments
This article was reviewed by Roger Cull, Edinburgh, UK.
REFERENCES
Other content recommended for you
- Management of chronic migraine
- Pharmacological prevention of migraine
- Efficacy of migraine prophylaxis treatments for treatment-naïve patients and those with prior treatment failure: a protocol for systematic review and network meta-analysis of randomised controlled trials
- Headache-related health resource utilisation in chronic and episodic migraine across six countries
- Adverse and serious adverse events incidence of pharmacological interventions for managing chronic and episodic migraine in adults: a systematic review
- Migraine: navigating the hormonal minefield
- Chronic migraine
- Migraine and its psychiatric comorbidities
- Efficacy of patent foramen ovale closure for treating migraine: a prospective follow-up study
- Calcitonin gene related peptide in migraine: current therapeutics, future implications and potential off-target effects