Article Text

Abstract
To err is human, and it is normal to make minor cognitive errors from time to time. Some people experience persistent subjective cognitive difficulties that cause distress and functional impairment, with no underlying structural, neurodegenerative, toxic or metabolic cause. This is considered a form of functional disorder. In this article, we review functional cognitive disorder and outline its core clinical features. Patients with this are typically of working age and have a source of psychological distress, such as chronic pain, work stress or family difficulties. Its distinction from incipient dementia is difficult and usually requires interval follow-up. Pointers towards possible dementia include abnormal neuroimaging or loss of insight. Many patients accept a functional cognitive disorder diagnosis and willingly engage with psychological therapies but there is no defined optimal treatment. Functional cognitive disorder is common but under-studied; future research priorities include the development of clear diagnostic criteria and robust trials of therapeutic strategies.
- COGNITION
- DEMENTIA
- SOMATISATION DISORDER
- COGNITIVE NEUROPSYCHOLOGY
Statistics from Altmetric.com
Introduction
A subjective decline in memory, attention and concentration or other cognitive difficulties is a common reason for referral to general neurology and dementia services.1 ,2 The ageing population and increased awareness of dementia are increasing the volume of work. In the cognitive clinic, we encounter many patients with persistent subjective, distressing cognitive problems, sometimes interfering with day-to-day life, but with no neurological disease process or general medical cause emerging even after several years of follow-up.3 ,4 We propose that A subgroup of these patients can best be characterised as having functional cognitive disorder, where intellectual symptoms—sometimes combined with other functional symptoms and mental health difficulties—are significantly linked to underlying psychological factors that may or may not be apparent. In a recent audit of the North Bristol Trust ReMemBr cognitive clinic database, we found one-third of patients aged <60 years had a final diagnosis of functional cognitive disorder; this is similar to the proportion of new general neurology patients diagnosed with functional neurological symptoms.5–7 It is therefore a common problem that affects people of working age. Defining such a clinical syndrome has generated some debate, and there is very little research exploring effective interventions for this group. In this article, we discuss how best to define, diagnose and manage this condition and outline common pitfalls to avoid. Clearly defining functional cognitive disorder improves diagnostic speed and accuracy, thus allaying patient anxiety and reducing the need for repeated assessments. Box 1 shows the proposed core clinical features of functional cognitive disorder, and boxes 2 and 3 describe typical case histories (figure 1).
Core clinical features of functional cognitive disorder
One or more persistent cognitive symptoms that are distressing and/or cause significant impairment in day-to-day functioning
Inconsistencies between self-reported symptoms and everyday functioning/neuropsychological test results
Symptoms are not better explained by another neurodegenerative, neurological, general medical or mental health condition.
The symptoms do not objectively progress over time (although may fluctuate)*
*We suggest at least 1-year follow-up (unless there is already objective evidence that the symptoms have not evolved over the past year or more). This provides a ‘safety net’ to catch patients with an atypical presentation of early stage neurodegeneration, who would be expected to decline significantly over 1 year. Reassessing patients any earlier may be falsely reassuring in those with early neurodegeneration.
Case history 1
A 48-year-old woman presented with memory difficulties. She was university educated but reported lifelong difficulties laying down memories. This had worsened over several years, with problems recalling recent family events and episodic word finding difficulties.
On examination, her estimated IQ was 124, and she performed in the high-average range on most neuropsychological tests. There were some inconsistencies: during tests of psychomotor speed and divided attention she was at the second percentile on an easy test, but at the 54th percentile on a more challenging task. This suggested that her poor speed on the easy task related to non-neurological factors such as anxiety. She rated her own memory as being low average, but objectively she performed in the average-to-high average range on most tests of memory. Neuroimaging and blood tests were normal.
On follow-up, she had persistent concerns about her memory, despite being shown that her performance was high average (with a few inconsistencies) and that her neuroimaging normal (figure 1A). She attended clinic alone on both occasions. There was no evidence over prolonged follow-up of neurodegeneration or other neurological or psychiatric illness. There were significant work stressors; her self-reported concerns about cognition seemed to date from around their onset. We diagnosed functional cognitive disorder after 18 months’ follow-up and reassured her that the symptoms did not reflect serious brain pathology. She had ongoing concerns about her memory at the follow-up assessment, despite scoring full marks on a Montreal Cognitive Assessment.8
Case history 2
A 58-year-old woman presented with memory and attentional difficulties. She reported losing the thread of a conversation, new problems managing personal finances, forgetting to lock her front door or to turn off the cooker, and colleagues had commented on her forgetting tasks. She had episodes of feeling ‘as if the world froze’ for minutes, followed by a sensation of dissociation.
There had been a number of stressful events over several years: she was the full-time career for her mother prior to her death 2 years before, and more recently her father had died unexpectedly. She attended clinic alone and reported that her daughter felt she had minor memory lapses but that this was ‘normal for me’. Two neuropsychological test batteries performed a year apart showed no significant decline. There was an atypical pattern of results on recall of a story, with free recall being better than delayed recognition, and she failed performance validity testing. She rated her own memory as significantly impaired, but testing did not show this. She had successfully completed a second university degree in the recent past, despite reporting significant cognitive difficulties at the time. This implied a significant degree of variability in symptoms or mismatch between her perception of her cognitive abilities and actual performance.
Interestingly, she did not volunteer that she had previously presented to another hospital with the same symptoms. The conclusion from both teams, who between them had seen her over a period longer than a year, was that her symptoms were non-progressive. The diagnosis was of functional cognitive disorder in the context of, but not fully explained by, underlying psychological distress and mood disturbance.

(A) MR image (axial T2-weighted) of case 1. (B) MR image (axial FLAIR) of case 3.
Classification of functional cognitive disorder
Functional cognitive disorder is probably best considered as a form of functional neurological symptom disorder,9 with similar root causes to other conversion disorders. The diagnostic criteria for functional neurological symptom disorder require motor or sensory symptoms that are incompatible with recognised neurological or medical conditions, cannot be better explained by an alternative diagnosis and cause significant distress or functional impairment. Functional cognitive disorder closely resembles this, but has cognitive rather than motor or sensory symptoms. The risk factors are also similar: previous childhood adversity, stressful life events and maladaptive personality traits. Patients may have a pre-existing diagnosis of a psychiatric condition, typically mild depression or anxiety. The presence of a major psychiatric diagnosis such as severe depression or bipolar disorder is an exclusion criteria for functional cognitive disorder, as major mental health problems can themselves cause significant cognitive difficulties.10
Towards a definition of functional cognitive disorder
It is often easy to tell patients what they do not have—their symptoms are not due to head trauma, epilepsy or medication side effects and dementia is unlikely if there is no evidence of decline over years. Excluding neurodegenerative, structural or metabolic problems is crucial, but as with other functional disorders it is best to put the diagnosis in a positive framework, by describing what functional cognitive disorder is, as opposed to what it is not.
Previous definitions include that of Delis and Wetter11 who classified patients as having either a cogniform disorder or cogniform condition, according to whether or not their symptoms affected day-to-day performance.
Patients with cogniform disorder have excessive cognitive complaints or low neuropsychology scores (‘excessive’ being defined as an inconsistent or non-organic pattern of performance, or failure to pass performance validity testing; see box 5), poor performance in everyday life and a lack of evidence of a neurological, neuropsychiatric or toxic cause or malingering. The cognitive difficulties are pervasive and persistent.
Patients with cogniform condition are similar, but despite reporting significant cognitive problems, they perform at a better than expected level on neuropsychological testing or in everyday life.
Delis and Wetter considered cogniform condition to be more common and less severe at a population level. However, it is often difficult to assess the everyday impact of cognitive symptoms as patients may not be in employment for reasons predating their cognitive symptoms (eg, general medical problems, physical disabilities or chronic pain) or may voluntarily change their pattern of employment or seek redundancy because of subjective cognitive decline. This is doubly problematic as health and social problems are themselves risk factors for developing a functional disorder.12 Finally, secondary gain (eg, medical retirement on cognitive grounds) may make it difficult to assess objectively the everyday impact of symptoms. Therefore, using perceived day-to-day ability as a core diagnostic criterion is of questionable value. In addition, Delis and Wetter’s diagnostic criteria are broad and could encompass some people with mild cognitive impairment due to early neurodegeneration or previous brain injury.13
Metternich et al4 developed another set of criteria based upon a ‘Questionnaire for typical symptoms of functional memory disorder’.14 This enquires about the frequency of symptoms such as word-finding difficulties, driving errors and losing the thread of a conversation. Patients with functional cognitive complaints have significantly higher scores than healthy controls, and there is good test–retest reliability. However, this questionnaire has not been validated to distinguish functional memory disorders from mild cognitive impairment or early dementia. Anecdotally, we find that people with mild dementia tend to score highly. The Metternich diagnostic criteria include perceived everyday memory failures causing distress, a questionnaire score ≥5 and normal neuropsychological test scores. However, it can be challenging to assess cognition in those with invalid test results, and the deficits in early neurodegeneration are often very subtle. We therefore feel that these criteria would not distinguish functional cognitive disorder from early dementia. These criteria also require the presence of psychosocial stressors, while these may be apparent in many cases, not everybody will disclose (or have insight into) relevant sources of stress.
People of above average socioeconomic status and educational level appear to be more vulnerable to functional cognitive disorder. This may relate to higher external and internal expectations of an individual’s cognitive abilities or more exacting professional responsibilities.15 ,16 Schmidtke et al17 followed up a cohort of 46 patients with functional memory problems over a mean of 20.1 months, and over this time only one person was reclassified as having early neurodegeneration. While we need further work to replicate this finding, it is reassuring that the misdiagnosis rate appears so low.
Typical features of functional cognitive disorder
Patients have cognitive difficulties that they consider to be significantly different from their previous baseline. The onset is usually insidious but can be more acute after a traumatic event. Memory is often affected, alongside attention and concentration, and patients may report personality change or mood disturbance. The symptoms are frequently variable and context dependent, being worse in stressful situations such as the workplace. There is often a stereotyped pattern of problems, with patients reporting episodes of forgetting information that is over-learnt but later recalling it (mnestic block, such as being unable to remember a PIN when required); failure to sustain concentration during complex tasks and forgetting a task while on the way to complete it. There is typically a discrepancy between reported symptom severity and performance in daily life.
‘Memory perfectionism’ is characteristic: patients expect a very high standard from their memory and are very concerned about minor lapses that most people would consider ‘normal’, for example, forgetting a work colleague's name or mislaying keys.4 ,21 They rate their own cognitive abilities as being much worse than that found on objective testing and may feel that they are impaired compared with how they were some years previously. However, it is difficult for clinicians to address this concern, as they typically cannot compare with an objective baseline.
Although it can be challenging to assess everyday abilities, it is helpful to look for inconsistencies between reported and actual functioning and to seek family or friends’ opinion (as in case 2, box 3). In our experience, an early pointer towards functional cognitive disorder is significant self-reported cognitive problems, but with lack of concern from work colleagues or family. This contrasts with people with dementia, who typically lack insight into their difficulties.18 ,19 Some patients with functional cognitive disorder have persistent minor symptoms that cause significant anxiety. This may arise through misinterpreting ‘normal’ cognitive errors, for example, case 1 was very worried about having forgotten the ending of a novel that she had read several months before.
Excluding other conditions
Functional cognitive disorder should only be diagnosed only after excluding other causes of cognitive decline as far as possible. Patients need particular consideration to possible very early neurodegeneration, which can be difficult to distinguish from functional cognitive disorder (as in case 3, box 4). Often the diagnosis is initially unclear, and these cases need careful follow-up to look for progressive decline. We considered including negative amyloid positron-emission tomography scanning or cerebrospinal fluid biomarkers as part of the core clinical criteria, as these are the most sensitive tests for early neurodegenerative dementia.17 However, these tests are not widely in routine clinical use and we felt that a practical definition of functional cognitive disorder should be applicable to most clinical settings.
Case history 3
A 77-year-old woman presented with a gradual decline in expressive language over 3 years. Her symptoms were variable, with no reported memory problems or difficulties with activities of daily living. Some years previously she had been diagnosed with fibromyalgia and was bed-bound with this for several months; she recovered using homeopathy. She reported low mood and poor sleep for 2 years, which she attributed to chronic back pain. She felt her speech problems were pain related but was also worried about possible dementia.
Her initial Mini-Mental State Examination20 score was 19/30; a year later this was 20/30. On a neuropsychological battery, her immediate memory was at the second percentile, visuospatial function at the 14th percentile, and language, attention and delayed memory scores were below the first percentile. She also reported depression and anxiety. Her MR scan of brain showed small vessel ischaemic change and mild generalised involutional change. Her EEG and blood tests were normal.
The initial diagnosis was uncertain. There were features to suggest a functional cognitive disorder, but also ‘red flags’ for neurodegeneration, namely age, reduced symptom insight and atrophy on brain imaging (figure 1B). We communicated this to her. On further follow-up there was progressive cognitive decline over time, leading to a diagnosis of Alzheimer’s disease.
Confounders such as medication side effects, previous brain injury (structural, metabolic or toxic) or general medical problems (eg, obstructive sleep apnoea or hepatic encephalopathy) should be sought. However, if cognitive symptoms persist after treating a systemic condition, it is important to reconsider the possibility of functional cognitive disorder (possibly triggered by health anxiety).
Functional cognitive disorder should be distinguished from dissociative amnesia, where patients lose important autobiographical information (either for a single traumatic event or for their entire life history).21 ,22 Dense retrograde amnesia before a specific time point typically occurs in dissociative amnesia, while patients with functional cognitive disorder typically have memory difficulties affecting the registration and recall of new information. Retrograde memory problems do occur in functional cognitive disorder but are not limited to specific life events, and there is usually a wider spectrum of difficulties with concentration, attention and/or executive function. A presentation with prominent amnesia for specific life events or basic over-learnt autobiographical information (eg, name, date of birth, names of close family members) suggests dissociative amnesia rather than functional cognitive disorder (after excluding organic causes).
Other possibilities to consider include illness anxiety disorder and dementia phobia. Illness anxiety disorder (also known as health anxiety) is characterised in DSM-5 by a preoccupation with having a serious illness, a high level of anxiety about health, and excessive health-related behaviours (either repeated use of medical services or abnormal avoidance of these), without somatic symptoms.21 ,23 In contrast, people with functional cognitive disorder are preoccupied by specific symptoms and appear to accept that they do not have a serious illness (although this does not alleviate their symptoms). In functional cognitive disorder, the patient’s focus is on symptoms and cognitive ability, rather than on anxiety about serious pathology. It may be difficult to distinguish functional cognitive disorder from health anxiety, particularly if a patient does not articulate their underlying concerns; physicians should proactively ask patients what they think is wrong, and why they have sought a medical opinion. There are overlapping clinical features and anxiety is common in functional disorders.24
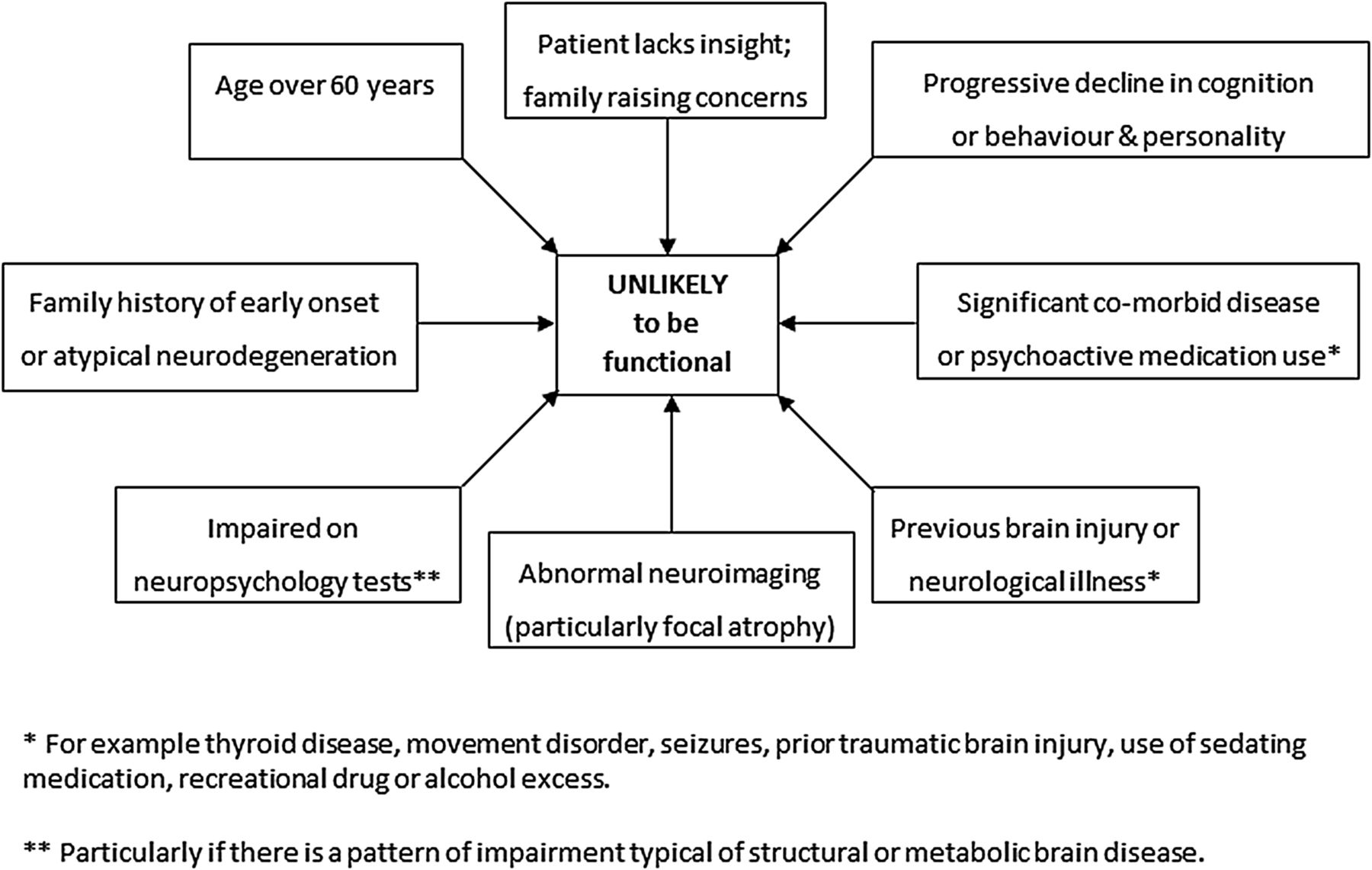
Surveys of the general public show that dementia is highly feared; with increasing life expectancy, worrying about developing dementia in the future is not in itself irrational.25 However, ‘worried well’, cognitively intact people who express concerns about having or developing dementia but who respond well to reassurance and do not seek repeated medical opinions should not be labelled as having a functional or anxiety disorder. Education about lifestyle strategies to reduce the risk of developing neurodegeneration could help to divert their attention to positive channels. Clinicians should take care to avoid missing those presenting with early stage or atypical neurodegeneration, particularly if there are red flags (illustrated in figure 2).

Red flags suggesting a neurodegenerative, systemic, toxic or metabolic cause.
It is important in the cognitive clinic always to enquire about head trauma (recent or remote). Previous significant injury (as judged by duration of loss of consciousness, degree of retro- or anterograde amnesia, need for neurosurgical intervention and structural changes on imaging) may be a direct or indirect cause of cognitive decline. Previous traumatic brain injury increases the risk of future dementia; patients may also be at risk of seizure disorders.26
Subjective cognitive problems dating from a mild brain injury or concussion suggest post-concussion syndrome.27 This a non-specific constellation of symptoms such as headache, poor sleep, fatigue, dizziness, cognitive difficulties and emotional disturbance, which is more frequent in people with pre-existing anxiety, depression and life stressors. Post-concussion syndrome may represent the misattribution of symptoms; affected individuals underestimate the prevalence of symptoms before the injury compared with healthy controls.28 This bias towards the ‘good old days’ is reminiscent of the way in which some patients with functional cognitive disorder describe their cognition being significantly better in the past. Subjective cognitive complaints attributed by the patient to a trivial head injury (especially when accompanied by somatic symptoms) better fit a diagnosis of post-concussion syndrome rather than functional cognitive disorder.
The prevalence of psychiatric diagnoses in those with functional cognitive disorders
Some authors use a psychiatric diagnosis as an exclusion criterion for the diagnosis of functional cognitive impairment.14 While depression is linked to cognitive difficulties such as reduced speed of information processing and memory deficits, this is more marked in severe depression.29–31 Mild symptoms of depression or anxiety are very common in the general population. The pattern of deficits should be considered: marked psychomotor retardation accompanied by very low mood suggests cognitive slowing due to severe depression, while intermittent minor cognitive lapses plus mild depressive symptoms is be better explained by functional cognitive disorder. Mild depression and anxiety are likely to underlie functional neurological and cognitive disorders, but not as the sole explanation.32 However, cognitive problems in the context of major mental health pathology such as bipolar disorder are more likely to result from the psychopathology or medication side effects.10 We would therefore exclude patients from a diagnosis of functional cognitive disorder only if a mental health disorder completely explains their cognitive problems. We take the view that functional cognitive disorder will at times accompany but is distinct from depression, anxiety and other psychiatric or functional diagnoses.
Investigations
Neuroimaging
CT scan, MR scan and 99mTc-HMPAO single-photon emission CT (SPECT) typically are normal. Incidental findings such as cysts should be evaluated on an individual basis. Cerebral atrophy that is out of keeping for the patient’s age or that preferentially affects the medial temporal, frontal or occipital lobes suggests early neurodegeneration and should prompt further investigations. A change to regional blood flow on SPECT is another red flag for underlying brain pathology. However, SPECT reporting is not standardised between centres and its specificity for dementia is only around 73%.33 ,34 Some centres use fludeoxyglucose positron-emission tomography during a work-up for dementia, which is more sensitive and specific than SPECT.23 Evidence of previous brain injury may indicate that a person's cognitive difficulties are in fact due to structural brain damage or epilepsy; those with prior brain injury may be more vulnerable to premature neurodegeneration;35 ,36 these patients should be carefully followed up and considered for early use of cognitive enhancers.
EEG
EEG is reserved for patients with suspected encephalopathy, epilepsy or prion disease. It should be normal in functional cognitive disorder, and abnormalities should prompt a search for encephalopathy, epilepsy or local brain injury.
Blood tests
Routine blood tests in primary care before cognitive clinic usually includes full blood count, urea and electrolytes, glucose, liver function, thyroid function, B12 and folate, plasma viscosity/C reactive protein. At the cognitive clinic we add tests according to the clinical scenario, which often include syphilis and HIV serology; antibodies (anti-voltage-gated potassium channel, anti-N-methyl-D-aspartate (NMDA) receptor, anti-glutamate decarboxylase antibodies, thyroid peroxidase) and sometimes metabolic testing such as ammonia (especially if the patient is taking a medication such as sodium valproate). Genetic testing is appropriate in selected patients, for example, those with a strong family history of neurological or neurodegenerative disease, or added features such as a movement disorder.
Neuropsychology
Most patients require a neuropsychological assessment to determine the pattern and extent of the cognitive impairments. Evaluating performance validity is essential; this encompasses formal performance validity tests (box 5), apparent anxiety or distress during testing, excessive (or lack of) concern about errors or an inconsistent or atypical pattern of results. Patients with functional cognitive disorder often have subjective memory ratings that are far lower than their objective scores, reflecting ‘memory perfectionism’, whereby patients demand an unreasonable standard of memory performance from themselves.
Performance validity tests
Tests of performance validity such as the Test of Memory Malingering and Reliable Digit Span aim to pick up underperformance on neuropsychological tests.37 ,38 They appear to be quite difficult but are in fact very easy. Healthy persons, those with mental health diagnoses or mild cognitive impairment make very few mistakes.39 ,40 However, because the task appears difficult, those consciously or subconsciously underperforming score badly. These should not be interpreted in isolation but within the context of overall performance on neuropsychological testing.
People with a high IQ and high-level education pose a particular challenge, as an average or above average test score may not exclude a decline from their previous high level of functioning.41 Enquiring about work performance and seeking opinions from their family is particularly useful, as is follow-up clinical and neuropsychological assessment after at least a year. Interval neuroimaging may also help to exclude neurodegeneration. If diagnostic doubt persists, we suggest further annual follow-ups. It is best to avoid repeating neuropsychology too soon, as this can lead to practice effects or be falsely reassuring in a patient with early neurodegeneration. Neuropsychological expertise is often also required to test people who do not speak the same language as the assessor.
The neuropsychologist's opinion of the overall cognitive performance pattern is often very useful. Focal impairment in a single domain should prompt a search for a neurological disease process, as should behavioural change, such as disinhibition.
There are specific questionnaires to detect the depression, anxiety and somatic symptoms (the Patient Health Questionnaire42) or post-traumatic stress disorder (Detailed Assessment of Post-traumatic Stress43). The Cambridge Behavioural Inventory44 can be completed by a close friend or relative, to document the extent to which symptoms interfere with activities of daily living.
In general neurology clinics, it can be difficult to access neuropsychology, or it may simply be not available. In these situations, the Montreal Cognitive Assessment (MoCA)8 and Addenbrooke’s Cognitive Examination-3 (ACE 3)45 are probably the most useful tools available. Poor effort, anxiety, undue pessimism about their performance or extremely poor performance in relatively easy parts of the test (eg, repetition of address) in the face of reasonable day-to-day function and normal neuroimaging suggest a possible functional disorder. The level of detail provided by the patient can also be informative: a comparison of histories provided by patients with functional memory difficulties and those with dementia found the patients with functional problems to give far richer accounts of their symptoms. Patients with functional difficulties also showed evidence of intact working memory during discussions by successfully answering multi-stranded questions, unlike those with dementia who required repeated prompting.46 However, there are several pitfalls for the unwary. A discrepancy between how the patient seems in conversation and their score on the ACE 3 or MoCA might indicate poor effort, but equally could be due to dementia but with the person with retaining a good social façade; isolated deficits should raise concerns about focal neurodegeneration or structural brain disease, for example, visuospatial difficulties in a person with posterior cortical atrophy.
Overview of the clinical features of functional cognitive disorder
In summary, patients with functional cognitive disorder typically have persistent mild cognitive symptoms that usually have a negative impact on everyday tasks; nevertheless, some people continue to work without difficulty in intellectually demanding jobs. Patients often show ‘memory perfectionism’, over-emphasising the importance of having a good memory and over-interpreting minor cognitive mistakes. Investigations do not show any underlying structural pathology, neurological disease or medical cause and their symptoms do not objectively progress over time. Neuropsychological assessment is typically either normal or judged to be an invalid reflection of their true abilities. Most people have underlying stressors, and mild mental health problems are very common. Clinicians must take care to avoid mislabelling functional cognitive disorder as early neurodegeneration and vice versa. Figures 2 and 3 give red flags for and against a functional diagnosis.

{kind=link}
{kind=link}
{kind=link}
Red flags suggesting a functional cognitive disorder.
How should we manage these patients?
In a patient with suspected functional disorder, we suggest explaining to patients at an early stage that this is a possible diagnosis. This involves using a framework of explaining how subjective cognitive symptoms can be caused either by internal factors such as psychological distress or pain, or by external factors such as a stressful environment or a change in working patterns.32 We recommend framing the diagnosis in terms of the positive features (such as memory perfectionism, rumination on trivial cognitive errors and objective evidence of normal cognitive abilities). Explaining to patients that functional or psychological causes of impaired memory are fairly common can also help. Depending on the context, we may try to reassure patients that the symptoms are within the normal range of adult brain functioning (eg, having minor memory lapses or losing concentration in a busy, stressful or boring situation). Neuroimaging, neuropsychological assessment and blood tests are typically requested to exclude underlying neurodegeneration or other brain pathology. Patients whose symptoms have already significantly improved may not need further tests.
It may be useful to explore underlying precipitants and to try to manage these. We refer to neuropsychiatry services those patients with very persistent symptoms or significant psychiatric issues, such as post-traumatic stress disorder. We currently offer patients a dedicated collaborative therapeutic feedback session with a neuropsychologist to discuss how and why their diagnosis was made and to explore possible therapies. We are still investigating the benefit of this, but patients report that they value neuropsychology feedback as they have more time to explore triggers and coping strategies. A previous randomised controlled trial of group therapy involving education, stress management and mindfulness showed improvements in memory self-ratings at 6 months.47 There are also guided self-help strategies available.48
There is a gap in the resources available to patients with functional cognitive disorder. They often are not reassured by normal investigations and therefore remain concerned about their memory and thinking. Information and services to help them are very limited. From a clinical perspective, we need research to help to streamline the diagnostic process, to provide better self-help resources to patients and to validate potential treatments. Group therapy (either meeting in person or virtually) appeals as a strategy to show patients that making minor cognitive errors is common and part of the normal human experience. Investigating risk factors such as personality traits or coping styles is useful, as this can assist when making and explaining the diagnosis. Finally, the entity of functional cognitive disorder is a fascinating paradigm to help to investigate metacognition—what we think about when we think about thinking.49 Patients frequently under-rate their own cognitive abilities, which implies difficulties with error monitoring and show an abnormally low level of confidence in decision making. Techniques such as functional MR imaging may help to unravel how metacognition goes awry in functional cognitive disorder.
Key points
Patients with functional cognitive disorder report recurrent, minor cognitive symptoms that are out of keeping with objective assessments and which do not suggest neurological or neurodegenerative disease; investigations are normal and patients do not progressively deteriorate over time.
The most useful tool is often follow-up for at least 1 year.
Patients need a careful explanation of the diagnosis, emphasising positive diagnostic features, with tailored neuropsychological therapy (and neuropsychiatry involvement if appropriate).
We need better resources and therapies to manage this common cause of significant cognitive symptoms in working-age adults.
The slow progression of many types of neurodegeneration makes it often very difficult to exclude dementia definitely. We try to reflect this uncertainty honestly to patients. If after year-long follow-up there are no positive findings of neurodegeneration and there are features to suggest a functional disorder, then it is in the patient's best interests to explore this diagnosis.
Acknowledgments
The authors thank Dr Jon Stone for his expert input in revising this manuscript.
References
Footnotes
Contributors Clinical assessments: EC, CP and MN. Data collection and analysis: AH and CP. Manuscript preparation: CP, EC and MN.
Funding Catherine Pennington is funded by an NIHR clinical lectureship and Drs Coulthard and Newson are funded by BRACE charity, North Bristol NHS Trust and University of Bristol. Amrit Hayre was funded by a BBSRC summer research experience placement. The authors have no competing interests to declare.
Competing interests None declared.
Ethics approval North Bristol NHS Trust.
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Jon Stone, Edinburgh, UK.
Linked Articles
- Editors' commentary
Other content recommended for you
- A unifying theory for cognitive abnormalities in functional neurological disorders, fibromyalgia and chronic fatigue syndrome: systematic review
- Predictors and prognosis of population-based subjective cognitive decline: longitudinal evidence from the Caerphilly Prospective Study (CaPS)
- Functional cognitive disorders: clinical presentations and treatment approaches
- 14 Differentiating functional cognitive disorder from early neurodegeneration: a clinic-based study
- Cerebrospinal fluid biomarkers in the differential diagnosis of Alzheimer's disease from other cortical dementias
- Performance validity test failure in clinical populations—a systematic review
- Feasibility randomised controlled trial of online group Acceptance and Commitment Therapy for Functional Cognitive Disorder (ACT4FCD)
- Fully automated cognitive screening tool based on assessment of speech and language
- Decade of progress in motor functional neurological disorder: continuing the momentum
- Management of functional communication, swallowing, cough and related disorders: consensus recommendations for speech and language therapy