Article Text

Abstract
OBJECTIVES To clarify the nosological relation among Miller Fisher syndrome (MFS), Guillain-Barré syndrome (GBS) with ophthalmoplegia, Bickerstaff's brain stem encephalitis (BBE), and acute ophthalmoparesis without ataxia. Serum samples from patients with each condition often have anti-GQ1b IgG antibody.
METHODS Information on antecedent illness, initial symptoms, neurological signs during the illness, and CSF findings were reviewed in 194 patients with anti-GQ1b IgG. It was determined whether overlapping MFS and GBS (MFS/GBS), as well as overlapping BBE and GBS (BBE/GBS), is explained by the combined action of anti-GQ1b IgG and anti-GM1 or anti-GD1a IgG, serological markers of GBS.
RESULTS Based on the diagnostic criteria, all the patients with acute ophthalmoparesis, MFS, MFS/GBS, BBE/GBS, and BBE had external ophthalmoplegia; all the patients with MFS, MFS/GBS, or GBS had hyporeflexia or areflexia; and all those with MFS and BBE showed ataxia. Tendon reflexes were decreased or absent in 91% of those with BBE/GBS, 67% of those with BBE, and 53% of those with acute ophthalmoparesis. Ataxia was present in 68% of the patients with MFS/GBS and 45% of those with BBE/GBS. Antecedent illness caused by upper respiratory tract infection had occurred in 60% to 80% of these patients, and CSF albuminocytological dissociation in 25% to 75%. Anti-GM1 or anti-GD1a IgG was present in 50% of those with GBS, 35% of those with MFS/GBS, 27% of those with BBE/GBS, 16% of those with MFS, and 8% of those with BBE.
CONCLUSIONS These findings together with the common autoantibody (anti-GQ1b IgG) suggest that a common autoimmune mechanism functions in the pathogenesis of these illnesses. In a larger study, it was confirmed clinically that MFS, GBS, BBE, and acute ophthalmoparesis are closely related, forming a continuous range. This is supported by the immunological findings. The term “anti-GQ1b IgG antibody syndrome” is not intended to be used as a clinical diagnosis, but recognition of this syndrome is useful for understanding the aetiological relation among the various illnesses and for introducing the established treatments of GBS for use with other conditions.
- anti-GQ1b IgG antibody
- Miller Fisher syndrome
- Guillain-Barré syndrome
- Bickerstaff's brain stem encephalitis
- ophthalmoplegia
Statistics from Altmetric.com
- anti-GQ1b IgG antibody
- Miller Fisher syndrome
- Guillain-Barré syndrome
- Bickerstaff's brain stem encephalitis
- ophthalmoplegia
Miller Fisher syndrome (MFS) is characterised by the acute onset of external ophthalmoplegia, ataxia of a cerebellar type, and the loss of tendon reflexes.1 It is considered a variant of Guillain-Barré syndrome (GBS), because some patients who present with MFS progress to GBS.2 Chiba et al 3found that all of six patients with MFS had serum IgG antibody to GQ1b ganglioside during the acute phase of the illness, whereas none of 16 patients with GBS had it. We found anti-GQ1b IgG antibody in one of 15 patients with GBS who had impaired abduction in the right eye.4 Chiba et al 5subsequently detected anti-GQ1b IgG in five of six patients with GBS who showed external ophthalmoplegia, whereas none of 23 patients with GBS without ophthalmoplegia had the autoantibody. Furthermore, anti-GQ1b IgG was present in all of five patients with acute postinfectious ophthalmoplegia without ataxia, “atypical MFS” in their designation. Case reports of paresis of the extraocular muscles without ataxia, which is of acute onset and self limited have been published.6 7 Such patients usually have had antecedent infections or immunisations. We designated this condition “acute ophthalmoparesis” and reported that all of eight patients with acute ophthalmoparesis had anti-GQ1b IgG.8 The autoantibody titres in acute ophthalmoparesis did not differ significantly from those in MFS. The existence of acute ophthalmoparesis cases supports the conclusion of Chiba et al 5that anti-GQ1b IgG is associated closely with external ophthalmoplegia. Kusunoki et al 9 reported that five of 149 patients with anti-GQ1b IgG had ataxia without ophthalmoplegia and stated that anti-GQ1b IgG is associated with ataxia as well as ophthalmoplegia.
Murine monoclonal anti-GQ1b antibody strongly stains the paranodal regions of the extramedullary portion of human oculomotor, trochlear, and abducens nerves, and weakly stains the deep cerebellar nuclei.5 In patients with MFS those nerves were enhanced by gadolinium on MRI.10 11 Campylobacter jejuni, cytomegalovirus, Epstein-Barr virus, and Streptococcus pyogenes have been reported as antecedent infectious agents in MFS.12 Koga et al 13 showed serological evidence ofC jejuniinfection in 12 (18%) of 65 patients with MFS, and the GQ1b epitope is present in the lipopolysaccharide of C jejuniisolated from patients with MFS.14 Infection byC jejuni that bears GQ1b-like lipopolysaccharide may trigger production of anti-GQ1b IgG antibody in some patients with MFS, whose autoantibody may then bind to the ocular motor nerves and to the deep cerebellar nuclei causing ophthalmoplegia and cerebellar ataxia.
Bickerstaff et al 15 16described patients who experienced acute onset of external ophthalmoplegia and cerebellar ataxia, a syndrome, although severe, which had a benign prognosis. Patients showing drowsiness, brisk reflexes, extensor plantar responses, and hemisensory disturbance or CSF pleocytosis usually are considered to have Bickerstaff's brain stem encephalitis (BBE) rather than MFS. Opinions differ, however, as to whether these are distinct or related conditions. We found that all of three patients with BBE had high anti-GQ1b IgG antibody titres which decreased with clinical improvement.17 The fact that BBE and MFS share common autoantibodies suggests that they are closely related, not distinct, conditions. The anti-GQ1b IgG antibody titres in BBE did not differ significantly from those in MFS. By contrast, Bickerstaff and Cloake15 speculated that the aetiology of BBE is similar to that of GBS because they detected areflexia and CSF albuminocytological dissociation. We reported necropsy findings for a patient in whom limb weakness associated with BBE had been diagnosed clinically.18 The peripheral nerves showed moderate to severe loss of large myelinated fibres. The pathological findings supported the original hypothesis by Bickerstaff and Cloake15 that BBE is closely related to GBS. That patient had anti-GQ1b IgG. Some patients with GBS have coma associated with the absence of oculocephalic reflex.18 The existence of such cases supports the hypothesis of Bickerstaff and Cloake15that BBE is closely related to GBS.
We earlier proposed that MFS, GBS with ophthalmoplegia, acute ophthalmoparesis, and BBE should all be designated “anti-GQ1b IgG antibody syndrome” to clarify their nosological relations. The first aim of this larger study was to test our hypothesis that these are related conditions that form a continuous range. The second was to determine whether overlapping MFS and GBS, as well as overlapping BBE and GBS, can be explained by the combined action of anti-GQ1b IgG with anti-GM1 or anti-GD1a IgG, serological markers of GBS.19 20
Materials and methods
PATIENTS
Serum samples obtained from patients with various neurological disorders including motor neuron disease, multifocal motor neuropathy, and chronic inflammatory demyelinating polyneuropathy were referred to us from university and district general hospitals for antiganglioside antibody assays. Serum antibodies to GM1, GM2, GD1a, GD1b, GT1b, and GQ1b were measured using the enzyme linked immunosorbent assay (ELISA) described elsewhere.21 Serum was considered positive when the antibody titre was 500 or more. Anti-GQ1b IgG antibody was positive in the samples from 245 patients tested between December 1994 and September 1998. Medical records of the patients were reviewed by one of us (MO). Information on antecedent illness, initial symptoms, neurological signs during the illness, and CSF findings were obtained from 194 patients. The following signs were assessed: consciousness disturbance; blepharoptosis, internal or external ophthalmoplegia, nystagmus, facial weakness, and bulbar palsy; limb weakness (⩽3 on the Medical Research Council scale); Babinski's sign; deep tendon reflexes (brisk, normal, decreased, or absent); truncal or limb ataxia; and deep or superficial sense impairment. In the present study, the albuminocytological dissociation was defined as high CSF protein (⩾45 mg/dl) with normal cellularity (⩽5/μl ).
DIAGNOSTIC CRITERIA
The diagnosis of GBS was based on the established clinical criteria, and extensor plantar responses do not exclude the diagnosis if other features are typical.22 The diagnostic criteria used for MFS, BBE, and acute ophthalmoparesis are given in table 1. Patients who showed limb weakness, in addition to ophthalmoparesis and ataxia, were considered to have overlapping MFS and GBS (MFS/GBS). Patients who showed limb weakness, in addition to consciousness disturbance (coma, semicoma, or stupor) or pyramidal sign as well as ophthalmoparesis and ataxia, were considered to have overlapping BBE and GBS (BBE/GBS).
Diagnostic criteria for Miller Fisher syndrome, Bickerstaff's brain stem encephalitis, and acute ophthalmoparesis
STATISTICAL ANALYSIS
Analyses were performed with Stat View Version 4.5-J software (Abacus Concepts, Berkeley, CA, USA). Differences in proportions were tested by the χ2 test or Fisher's exact test (two tailed). A p value<0.05 was used for significance in all the comparisons.
Results
CLINICAL FEATURES OF ANTI-GQ1B IGG ANTIBODY SYNDROME
Clinical profiles of the 194 patients (median age 37; 106 men; 88 women) are shown in table 2. Ninety four per cent had antecedent illnesses (upper respiratory tract infection alone 75%; diarrhoea alone 9%; both upper respiratory tract infection and diarrhoea 5%). As initial symptoms respectively, 130 patients (67%) and 56 patients (29%) complained of diplopia and gait disturbance, and 25 patients (13%) had both. Consciousness was disturbed in 11% (drowsiness 7%; stuporous or comatose 4%). External ophthalmoplegia was present in 91% and ataxia in 80% (both truncal and limb 50%; truncal alone 20%; limb alone 10%). Of 155 patients who had ataxia, 41 (26%) had deep sense impairment. Limb weakness was appreciable in 26% of the 194 patients. Deep tendon reflexes were absent in 60% of them, decreased in 30%, normal in 6%, and brisk in 4%. Extensor plantar response was present in 8%, and hyperreflexia or the Babinski's sign in 9%. Patients with external ophthalmoplegia had associated ataxia (p<0.0001; odds ratio 33.7; 95% confidence interval 8.1–139.6), whereas neither ophthalmoplegia nor ataxia were associated with hyporeflexia or areflexia (p=0.8 and p=0.5 respectively). Fifty eight per cent had CSF albuminocytological dissociation.
Clinical profiles of patients with anti-GQ1b IgG antibody
CLINICAL FEATURES OF EACH DIAGNOSTIC CONDITION
The diagnosis of MFS was made for 110 (57%), MFS/GBS for 31 (16%), acute ophthalmoparesis for 15 (8%), BBE for 12 (6%), BBE/GBS for 11 (6%), and GBS for eight (4%). The illnesses of the other seven (4%) were unclassified. Among the patients included in this study, illustrative cases of acute ophthalmoparesis,23MFS,10 BBE,24 and MFS/GBS25 have been reported previously. An illustrative case of BBE/GBS is described below.
Case report of BBE/GBS
A 24 year old man had a cough and nasal obstruction which abated over a few days. One week after resolution of this illness, he experienced diplopia and numbness of the arms (day 1). On day 2, he was unable to stand. He became drowsy with dysarthria, and was admitted to a hospital on day 3. On admission, he was stuporous. Bilateral blepharoptosis, limitation of ocular movement in all directions, bilateral facial palsy, and slurred speech were noted. Light reflexes were prompt. Distal dominant weakness in the four limbs was scored 3 on the Medical Research Council scale. Deep tendon reflexes were absent, but extensor plantar responses remained. Finger to nose and heel to knee tests showed dysmetria and decomposition. Hypaesthesia of the glove and stocking type was present. Protein in CSF was 27 mg/dl with 1 cell/μl on day 7, and 295 mg/dl with 6 cells/μl on day 14. Seven sessions of immunoadsorption therapy were given on days 3, 4, 5, 7, 9, 11, and 13. In Japan, the patients with GBS and related disorders often receive immunoadsorption using a tryptophan conjugated column (TR-350, Asahi Medical, Japan) which highly absorbs anti-GQ1b IgG.26 On day 6, he began to recover consciousness, and limb weakness diminished. He could walk without support on day 19, and diplopia disappeared on day 39.
Table 2 shows the antecedent illness, initial symptoms, and neurological signs for each condition. For antecedent illness, the frequency of upper respiratory tract infection was much higher than that of diarrhoea for all the conditions except GBS. As the initial symptom, diplopia was experienced in 100% of the patients with acute ophthalmoparesis, 75% of those with both MFS and BBE, 55% of those with BBE/GBS, and 39% of those with MFS/GBS. Gait disturbance was experienced by 75% of the patients with GBS, 42% of those with MFS/GBS, 33% of those with BBE, 32% of those with MFS, and 18% of those with BBE/GBS. On the basis of the diagnostic criteria, all the patients with acute ophthalmoparesis, MFS, MFS/GBS, BBE/GBS, and BBE had external ophthalmoplegia; all the patients with MFS, MFS/GBS, and GBS had hyporeflexia or areflexia; and all the patients with MFS and BBE had ataxia. Tendon reflexes were decreased or absent in 91% of those with BBE/GBS, 67% of those with BBE, and 53% of those with acute ophthalmoparesis. Ataxia was present in 68% of the patients with MFS/GBS and 45% of those with BBE/GBS. Consciousness was altered in 63% of the patients with BBE/GBS, 50% of those with BBE, 13% of those with MFS/GBS, and 3% of those with MFS. Albuminocytological dissociation in CSF was present in 75% of the patients with BBE/GBS, 66% of those with MFS, 43% of those with MFS/GBS, 42% of those with BBE, and 25% of those with acute ophthalmoparesis and GBS.
ANTI-GM1 OR ANTI-GD1a IgG IN EACH DIAGNOSTIC CONDITION
Table 3 shows the immunological range for all the conditions. Anti-GM1 IgG antibody was present in 38% of the patients with GBS, 16% of those with MFS/GBS, 8% of those with BBE, and 5% of those with MFS. Anti-GD1a IgG antibody was present in 50% of the patients with GBS, 29% of those with MFS/GBS, 27% of those with BBE/GBS, 13% of those with MFS, and 8% of those with BBE. Anti-GM1 or anti-GD1a IgG antibody was present in 50% of the patients with GBS, 35% of those with MFS/GBS, 27% of those with BBE/GBS, 16% of those with MFS, and 8% of those with BBE. Neither anti-GM1 nor anti-GD1a IgG was present in acute ophthalmoparesis.
Antiganglioside IgG antibodies in each condition
Discussion
OUR DIAGNOSTIC CRITERIA FOR MFS AND BBE
One of the three patients originally described by Fisher1 showed mild drowsiness. Drowsiness therefore may accompany both MFS and BBE according to the criteria used in this study. All of the three cases reported by Fisher fulfilled our criteria for MFS, but not for BBE, whereas six of eight cases described by Bickerstaff16 fulfilled our criteria for BBE, but not for MFS. In case 4 reported by Bickerstaff16 the patient showed gross flaccid weakness. That condition was diagnosed as BBE/GBS based on our criteria. Because another patient (case 6) did not show ophthalmoplegia, neither the criteria for MFS nor BBE were fulfilled.
Al-Din et al 27 (with Bickerstaff) reported 18 patients with BBE (11 with drowsiness, one with coma). Tendon reflexes were absent in 11 of them, normal in three, and brisk in four. Babinski's sign was positive in five patients, and deep tendon reflexes were normal in one and absent in one. Ropper28 criticised this report and considered that six of the cases were typical MFS and the other 12 obscure brain stem lesions without peripheral neuropathy. Based on our criteria, MFS would have been diagnosed in six cases (cases 3, 5, 11, 13, 15, and 16) and BBE in 12. Our criteria therefore should prove useful for making clinical diagnoses of MFS and BBE. Later, Al-Din et al 29 (without Bickerstaff) diagnosed MFS in three comatose patients who showed ophthalmoplegia, ataxia, and areflexia. Patients 2 and 3 showed tetraplegia. Based on our criteria, case 1 in their report would be BBE and cases 2 and 3 BBE/GBS. Among our patients primary physicians had diagnosed four cases of “MFS associated with hyperreflexia” which, in this study, were diagnosed as BBE.
CLINICALLY CONTINUOUS RANGE OF MFS, GBS, BBE, AND ACUTE OPHTHALMOPARESIS
One hundred and forty two (73%) of the 194 patients with anti-GQ1b IgG fulfilled the criteria for the syndrome of ophthalmoplegia, ataxia, and areflexia according to Al-Dinet al 30; whereas 110 had MFS, 21 MFS/GBS, six BBE, and five BBE/GBS according to our criteria. All the patients with MFS fulfilled the criteria for the syndrome of ophthalmoplegia, ataxia, and areflexia, whereas only 68% of those with MFS/GBS, 50% of those with BBE, and 45% of those with BBE/GBS did. These findings indicate considerable overlapping of the syndrome of ophthalmoplegia, ataxia, and areflexia and anti-GQ1b IgG syndrome. The patients with anti-GQ1b IgG, however, had a statistically significant correlation only between ophthalmoplegia and ataxia. Neither ophthalmoplegia nor ataxia was correlated with areflexia. This is further support for the earlier report that ophthalmoplegia and ataxia are associated closely with anti-GQ1b IgG.5 9 Anti-GQ1b IgG antibody syndrome comprises a wide range presenting with ophthalmoplegia and ataxia. Chemical analysis showed that the optic nerves and the oculomotor, trochlear, and abducens nerves had similar concentration of GQ1b.31 The GQ1b epitope localisation suggested immunohistochemically, however, was different: no accumulation of staining in the specific region of the optic nerve. Their findings could explain why none of our patients who had anti-GQ1b IgG antibody showed optic neuropathy.
Seven patients were unclassified by the criteria we used. They had ophthalmoplegia and ataxia, but their tendon reflexes were normal during the illness. We elsewhere reported on four patients withCampylobacter neuropathy associated with anti-GM1 IgG, in whom muscle stretch reflexes were preserved or hyperactive throughout the illness.32 Although loss of tendon jerks is a valuable diagnostic feature of GBS, the presence of such unclassified cases suggests that the diagnostic criteria should be extended because this loss also could apply to MFS; therefore, those cases could be diagnosed as MFS. The other cases could be diagnosed as BBE because three of the 18 patients reported by Al-Dinet al 27 showed normal muscle stretch reflexes. Furthermore, the seven unclassified cases could be considered as overlapping MFS and BBE. The existence of such cases also supports the hypothesis that these conditions form a continuous range and that ophthalmoplegia and ataxia are more important than areflexia in that range. Thirty one cases of MFS/GBS and 11 cases of BBE/GBS were reported in this study. The existence of these overlapping cases strongly supports the idea of continuity between MFS and GBS, as well as between BBE and GBS.2 18
Double vision was an initial symptom in three of four of the patients with both MFS and BBE, and gait disturbance in one of three. Some patients who have MFS or BBE may not show ataxia at the onset of neurological symptoms and therefore acute ophthalmoparesis should be diagnosed. This suggests that acute ophthalmoparesis without ataxia is a restricted and mild condition of MFS or BBE.
IMMUNOLOGICAL EVIDENCE THAT MFS, GBS, BBE, AND ACUTE OPHTHALMOPARESIS FORM A CONTINUOUS RANGE
For each condition, antecedent illness caused by upper respiratory infection was present in 60% to 80% of the patients, and CSF albuminocytological dissociation in 25% to 75%. This suggests that a common autoimmune mechanism functions in the pathogenesis of these conditions.
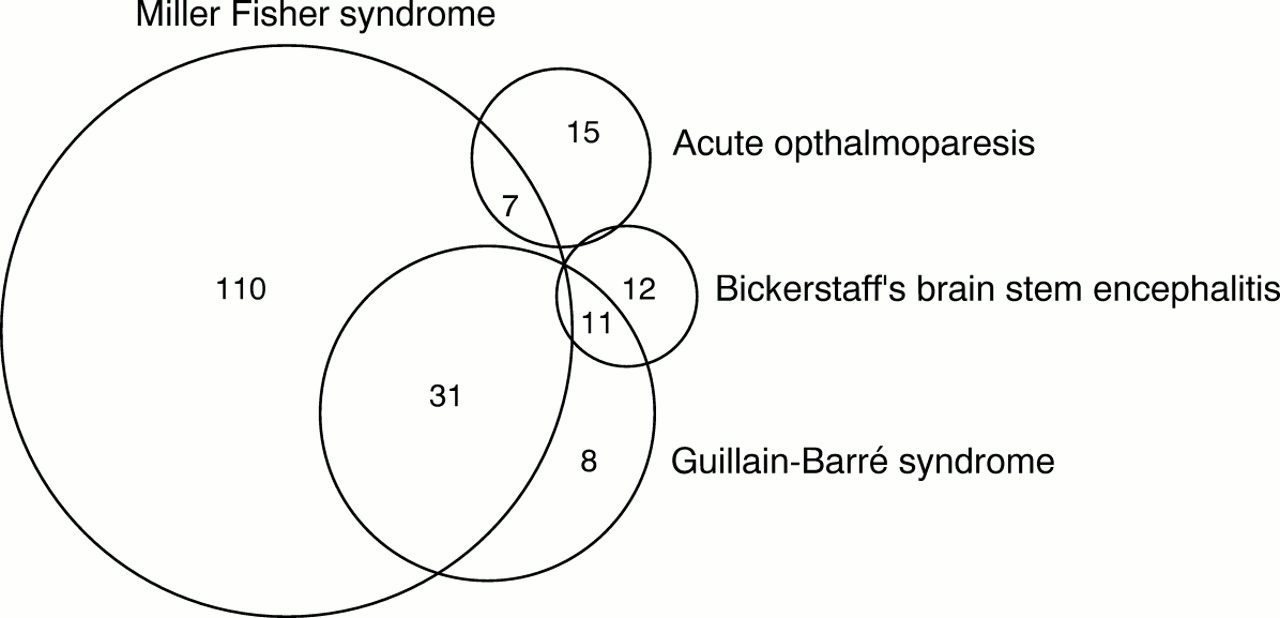
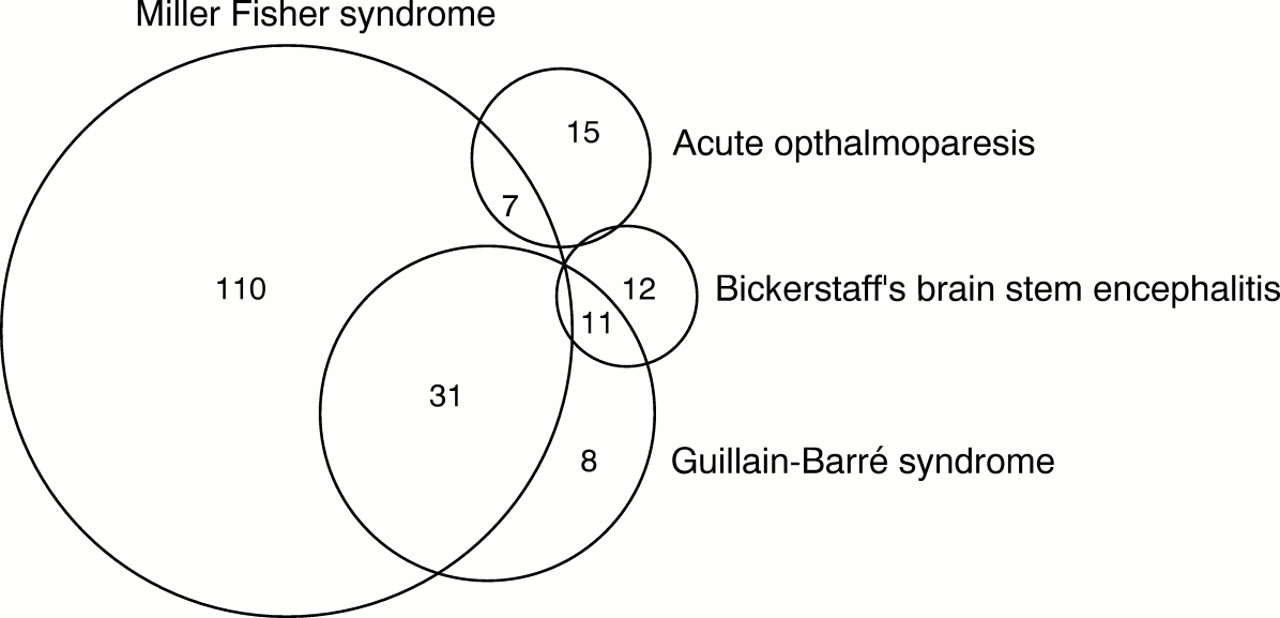{kind=link}
Nosological relations between Miller Fisher syndrome, acute ophthalmoparesis, Bickerstaff's brain stem encephalitis, and Guillain-Barré syndrome.
Whereas anti-GQ1b IgG is an immunological marker of MFS and related disorders,3-5 8 anti-GM1 IgG autoantibody may be a serological marker of axonal GBS.19 33 Anti-GD1a IgG antibody is closely associated with the axonal form of GBS,20 but was not detected in typical patients with MFS who did not show limb weakness.3 4 34 C jejuni is a common antecedent agent in MFS,13 as well as in GBS,35 36 and some patients who present as having MFS subsequent to C jejuni enteritis then progress to GBS.37 38 A single strain ofC jejuni has several lipopolysaccharides that bear epitopes common to such gangliosides as GM1, GD1a, and GQ1b.39 40 Infection by a strain ofC. jejuni may induce not only anti-GQ1b IgG, but anti-GM1 or anti-GD1a IgG in some patients with MFS/GBS. Among our patients with MFS/GBS, C jejuni actually was isolated from one with MFS/GBS who had anti-GQ1b and anti-GD1a IgG antibodies (case 4 of Ohtsuka et al 41). We therefore compared the frequencies of anti-GM1 or anti-GD1a IgG in MFS, MFS/GBS, and GBS. As expected, the frequency of anti-GM1 or anti-GD1a IgG in MFS/GBS (35%) was between that in MFS (16%) and that in GBS (50%). Moreover, the frequency of anti-GM1 or anti-GD1a IgG in BBE/GBS (27%) was between that in BBE (8%) and that in GBS (50%). In addition to the similarities in clinical presentation and share of anti-GQ1b IgG autoantibody, immunological results for the overlapping cases show that MFS, GBS, and BBE are closely related, not distinct, autoimmune mediated disorders. The patients with acute ophthalmoparesis had neither anti-GM1 nor anti-GD1a IgG. Serologically this indicates that MFS or BBE is located between acute ophthalmoparesis and GBS.
RECOGNITION OF ANTI-GQ1b IgG ANTIBODY SYNDROME AND ITS THERAPY
In this larger study, we confirmed clinically that MFS, GBS, BBE, and acute ophthalmoparesis are closely related and form a continuous range (figure). This was supported by immunological findings. We do not intend the term “anti-GQ1b IgG antibody syndrome” to be used as a clinical diagnosis, but recognition of this syndrome is useful for understanding the aetiological relations of MFS, GBS, BBE, and acute ophthalmoparesis. Moreover, established treatments for GBS (plasmapheresis and intravenous immunoglobulin) may be more readily introduced as treatments for BBE and acute ophthalmoparesis, as well as for MFS. Some patients with BBE and acute ophthalmoparesis have responded favourably to plasmapheresis and intravenous immunoglobulin8 23 24 42 Recent studies by Buchwaldet al 43 and Plompet al 44 show that anti-GQ1b IgG, at least, is a pathophysiological mediator of motor symptoms in MFS and related disorders. This is theoretical evidence that removal of the autoantibody is efficacious treatment for patients with anti-GQ1b IgG.
Acknowledgments
This research was supported in part by grants in aid for Scientific Research (10780482 and 10557063 to NY) from the Ministry of Education, Science, Culture, and Sports of Japan and the Ryoichi Naito Foundation for Medical Research and a Research Grant for Neuroimmunological Diseases from the Ministry of Health and Welfare of Japan.