Article Text

Abstract
Objective: To investigate the effects of topiramate on Tourette syndrome (TS).
Background: Dopamine-receptor-blocking drugs have been traditionally used to control tics in patients with TS, but these neuroleptics are associated with potentially limiting side effects.
Methods: This is a randomised, double-blind, placebo-controlled, parallel group study. To be included in the study, subjects required a DSM-IV diagnosis of TS, were 7–65 years of age, had moderate to severe symptoms (Yale Global Tic Severity Scale (YGTSS) ⩾19), were markedly impaired as determined by the Clinical Global Impression (CGI) scale severity score of ⩾4 and were taking no more than one drug each for tics or TS comorbidities.
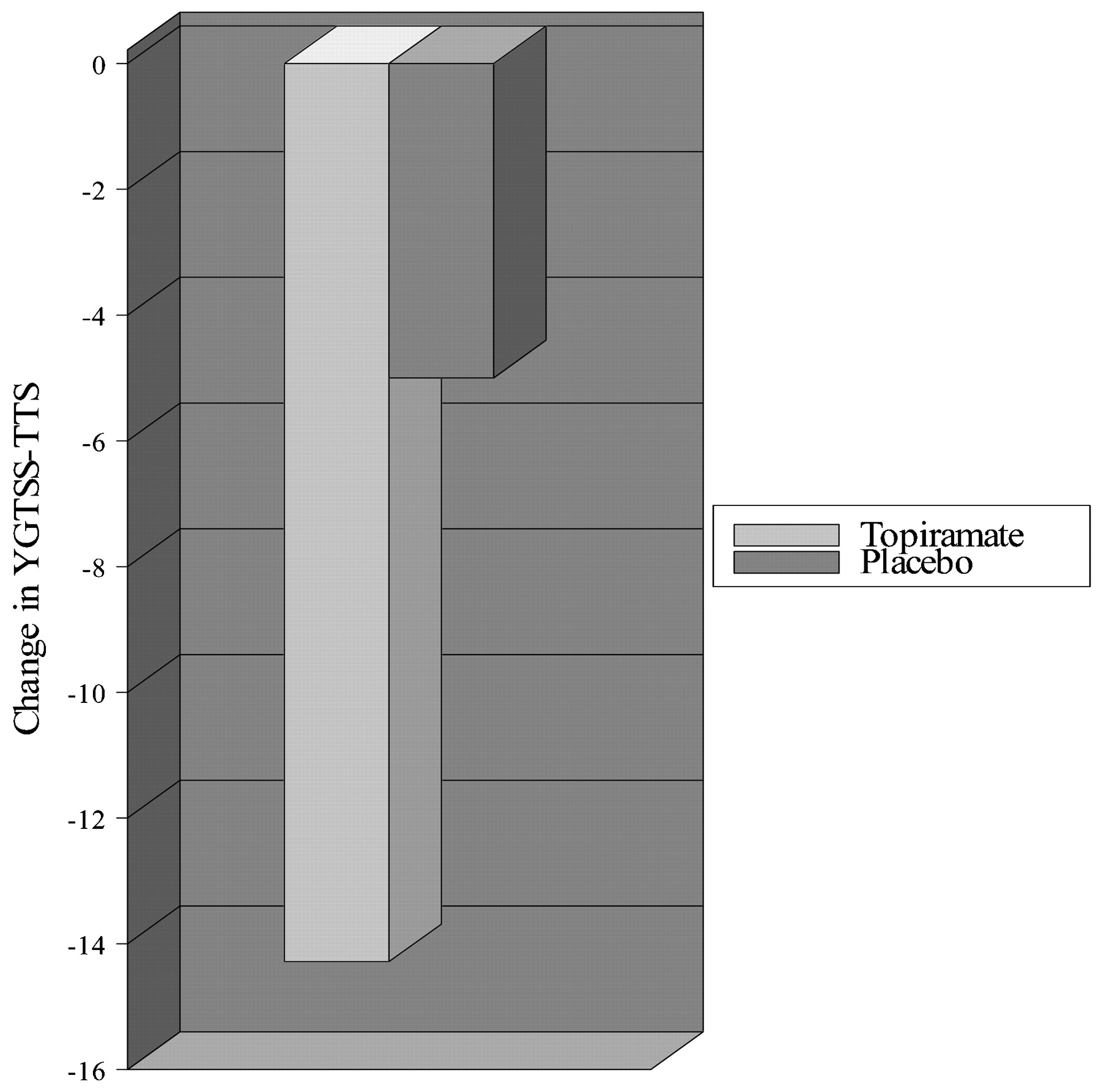
Results: There were 29 patients (26 males), mean age 16.5 (SD 9.89) years, randomised, and 20 (69%) completed the double-blind phase of the study. The primary endpoint was Total Tic Score, which improved by 14.29 (10.47) points from baseline to visit 5 (day 70) with topiramate (mean dose 118 mg) compared with a 5.00 (9.88) point change in the placebo group (p = 0.0259). There were statistically significant improvements also in the other components of the YGTSS as well as improvements in various secondary measures, including the CGI and premonitory urge CGI. No differences were observed in the frequency of adverse events between the two treatment groups.
Conclusion: This double-blind, placebo-controlled trial provides evidence that topiramate may have utility in the treatment of moderately severe TS.
Statistics from Altmetric.com
Tourette syndrome (TS) is a complex neurological disorder characterised by multiple motor and phonic tics, and a wide range of behavioural problems, including attention deficit with or without hyperactivity, obsessive–compulsive behaviour and impulse control problems.1 The pharmacological treatment of TS usually consists of antidopaminergic drugs2 3 4 and a wide array of other drugs, but the frequent occurrence of side effects limits their usefulness. Furthermore, many patients fail to obtain satisfactory relief of their symptoms, and some patients with disabling symptoms require surgical intervention.5 There is, therefore, an unmet need for safer and more effective pharmacological treatments of tics and TS behavioural comorbidities.
Topiramate is a broad-spectrum antiepileptic drug used as adjunctive and monotherapy in a wide variety of seizures. It has also been reported to be effective in the management of headache, mood and behavioural disorders, pain and tremors.6 The exact mechanism of action of topiramate is unknown, but the drug has been found to enhance γ-aminobutyric acid subtype A (GABAA)-receptor-mediated chloride flux and thus may potentiate GABA-mediated inhibition. Topiramate also blocks the AMPA/kainate subtype of glutamate receptors without affecting the N-methyl-d-aspartate (NMDA) subtype. In humans, topiramate has been found to increase cerebral GABA, homocarnosine and pyrrolidinone concentrations; it also acts as a weak carbonic anhydrase inhibitor.7 Topiramate is rapidly absorbed, with peak serum concentrations observed 1–4 h after ingestion, readily enters the brain and has over 80% bioavailability. Topiramate has clear advantages over neuroleptic medications in that it carries no risk of tardive dyskinesia or excessive weight gain. We designed this double-blind, placebo-controlled trial to evaluate the efficacy and tolerability of topiramate in TS.
Methods
This is a multicentre, randomised, double-blind, placebo-controlled, parallel group study designed to investigate the change in severity of TS tic symptoms following treatment with topiramate when compared with placebo (ClinicalTrials.gov identifier: NCT00206323). After giving an informed consent approved by the Review Boards for Human Research of the participating institutions, the subjects were screened for inclusion and exclusion criteria. In order to meet the inclusion criteria, the subjects must have a DSM-IV diagnosis of TS for at least 3 months, be between 7 and 65 years of age and weigh over 25 kg. Subjects must have a minimum Yale Global Tic Severity Scale (YGTSS) rating scale of ⩾19 and a Clinical Global Impression (CGI) scale severity score of ⩾4 at visit 1 (day −10 through day −7) and visit 2 (day 1). Subjects taking more than one agent for the treatment of tics or more than one agent for the treatment of comorbid behavioural symptoms were excluded.
The selected subjects underwent a screening/washout visit (up to 30 days prior to randomisation, 90 days if the subject had been treated with botulinum toxin), before being randomised to receive either topiramate or placebo in a 1:1 ratio according to a computer-generated code. The subject and investigator were blinded to treatment assignment. During the titration phase, the study medication, consisting of 25 mg of topiramate or a matching identically appearing placebo tablet(s), was gradually increased over 6 weeks up to 200 mg/day, depending on tolerance. All subjects had to reach a minimum dose of 50 mg/day in order for them to proceed to the 4-week maintenance phase, followed by a 12-day taper phase.
The following evaluations were performed on visit 2 (day 1) and visit 5 (day 70): YGTSS, CGI, Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) or Children’s Yale–Brown Obsessive–Compulsive Scale (CY-BOCS) (subjects ⩽17 years), and Conners’ Parent Rating Scale—Revised (L) (CPRS-R:L) (parent of subjects ⩽17 years) or Conners’ Adult A-D/HD Rating Scale—Self-Report: Long Version (CAARS-S:L) (subjects ⩾18 years). Some of the instruments were also administered during visit 3 (day 28) and visit 4 (day 56), and the subjects were contacted by telephone weekly in between the visits. In addition to these assessments, vital signs and a variety of laboratory tests were performed as part of safety monitoring.
The efficacy analyses were based on the intent-to-treat population that included all subjects who had taken at least one dose of study medication and had at least one postbaseline efficacy evaluation. The primary efficacy variable was the change in Total Tic Score of the YGTSS at the last visit compared with day 1. Changes of individual components of YGTSS were compared using analysis of covariance with the baseline score at day 1 as a covariate. Secondary efficacy variables included CGI, premonitory urge CGI, Y-BOCS/CY-BOCS and CPRS-R:L/CAARS-S:L. Results reported for the last visit are based on results obtained at visit 5 (day 70) and were not imputed if missing. Treatment groups were compared based on the incidence of adverse events and of adverse events of special interest based on the Fisher exact test. All statistical tests were two-sided at the 5% level of significance. Safety assessment was performed on the safety population, defined as all randomised subjects who received at least one dose of study drug. In the case of early withdrawal, data were obtained using the last observation carried forward (LOCF) method.
Results
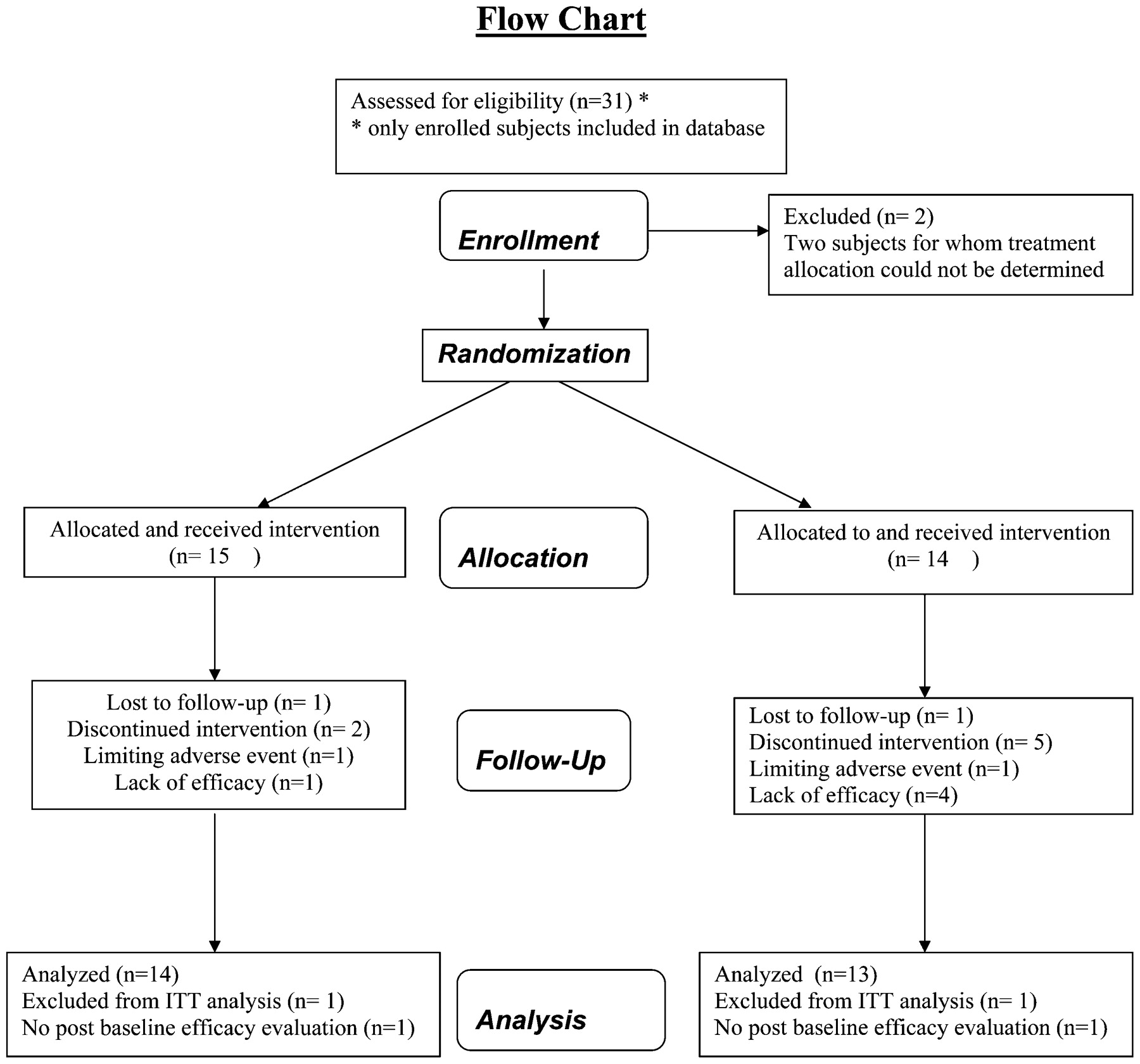
There were 29 patients (26 males), mean age 16.5 (9.89) years, randomised to topiramate (N = 15) or placebo (N = 14) arms (table 1). The three most common comorbidities were attention-deficit disorder (with our without hyperactivity), present in 6/15 (40%) in the topiramate group and in 4/14 (28%) in the placebo group, obsessive–compulsive disorder, present in 4/15 (26%) in the topiramate group and 2/14 (14%) in the placebo group, and migraine headaches, present in 4/15 (26%) in the topiramate group and 4/14(29%) in the placebo group. Twenty (69%) patients completed the double-blind phase of the study. The Total Tic Score (TTS), the primary endpoint, improved by 14.29 (10.47) (CI −18.43 to −1.31) points from baseline to visit 5 (day 70) with topiramate (mean dose 118 mg) compared with 5.00 (9.88) point change in the placebo group (p = 0.0259) (fig 1). In addition to TTS, there were also statistically significant improvements in the other components of the YGTSS, including the Total Motor Tic Score (TMTS), Total Phonic Tic Score (TPTS) and the Global Severity Score (GSS) (table 2). In addition, the CGI and the premonitory urge CGI improved. No clinically significant differences were observed in the secondary measures, the frequency of adverse events or the laboratory values between the two treatment groups (table 3).

Flow chart.
Demographics and baseline characteristics (based on the randomised population)
Efficacy results (based on the intention-to-treat population)
Adverse events (based on the safety population)
Discussion
Currently, there are only two drugs, haloperidol and pimozide, approved by the United States Food and Drug Administration for the treatment of TS. These drugs, however, have limited usefulness, as they are frequently associated with undesirable side effects, particularly drowsiness and weight gain, and both have a potential to cause tardive dyskinesia. The double-blind, placebo-controlled study described here provides evidence that topiramate, at a dose of about 100 mg/day, may be a safe and effective antitic drug as demonstrated by the robust improvement in the TTS, the primary endpoint (fig 1). There were also improvements in other components of the YGTSS (table 2) and in CGI and premonitory CGI. Our results are consistent with a report describing two adult TS patients whose symptoms apparently improved with topiramate (50–200 mg/day) while previous medications were tapered and discontinued during the first 2 weeks of treatment.8 Topiramate in our study was well tolerated, but some of the commonly observed topiramate adverse effects, such as somnolence, cognitive problems and weight loss, may not have been evident because the trial duration was relatively short.
{kind=link}
{kind=link}
Change from baseline to visit 5 (day 70) in Total Tic Score component of Yale Global Tic Severity Scale (YGTSS-TTS) in response to topiramate.
Since there is essentially no risk of tardive dyskinesia or weight gain, two potential adverse effects of typical or atypical neuroleptics, topiramate has a potential advantage over the dopamine-receptor-blocking drugs, frequently used in the treatment of tics associated with TS. Although tetrabenazine, a dopamine-depleting drug recently approved by the Food and Drug Administration for the treatment of chorea associated with Huntington disease,9 10 also has a low risk for these two side effects, the drug may cause depression, parkinsonism and akathisia. Nevertheless, tetrabenazine has been found to be effective in the treatment of tics2 and may possibly be combined with topiramate to optimise the desired therapeutic effects.
In conclusion, topiramate, as monotherapy or as an add-on to established therapy, may be an important addition to the armamentarium in the treatment of TS. A larger trial with a longer follow-up, however, is needed before topiramate can be recommended as a routine treatment of tics.
Acknowledgments
We thank P Weisleder and F Leigh (Duke University) and T Nelson (Carolina Neurological Clinic) for their participation and enrolment of some patients. We also thank C Hunter and E Jimenez (Baylor College of Medicine) and Y Collins and S Melamed (Children’s Hospital of Philadelphia) for their assistance.
REFERENCES
Footnotes
Funding The investigator-initiated study was supported by a grant from Ortho McNeil Janssen Scientific Affairs, LLC.
Competing interests None.
Ethics approval Ethics approval was provided by the Review Boards for Human Research of the participating institutions.
Patient consent Obtained.
Provenance and Peer review Not commissioned; externally peer reviewed.