Article Text

Abstract
Objective To examine mortality and factors associated with survival in a population based multiple sclerosis (MS) cohort.
Methods Clinical and demographic data of MS patients registered with the British Columbia MS clinics (1980–2004) were linked to provincial death data, and patients were followed until death, emigration or study end (31 December 2007). Absolute survival and the influence of patient characteristics (sex, disease course (primary progressive (PPMS) vs relapsing onset (R-MS)) and onset age) were estimated by Kaplan–Meier analyses (from birth and disease onset). Mortality relative to the general population was examined using standardised mortality ratios. Excess mortality associated with patient characteristics and time period of cohort entry was assessed by relative survival modelling.
Results Of 6917 patients, 1025 died. Median survival age was 78.6 years (95% CI 77.5 to 79.7) for women and 74.3 years (95% CI 73.1 to 75.4) for men. Survival from onset was longer for R-MS (49.7 years; 95% CI 47.9 to 51.5) than for PPMS (32.5 years; 95% CI 29.5 to 35.7); however, survival age was similar. The overall standardised mortality ratios was 2.89 (95% CI 2.71 to 3.07), and patients survived approximately 6 years less than expected, relative to the general population. PPMS had a higher relative mortality risk compared with R-MS (relative mortality ratio (RMR) 1.52; 95% CI 1.30 to 1.80). Women with PPMS had a relative survival disadvantage compared with men with PPMS (RMR 1.55; 95% CI 1.19 to 2.01). Relative survival within 10 years of cohort entry was similar between time periods.
Conclusions Some of the longest MS survival times are reported here but the risk of death was still greater than in the age, sex and calendar year matched general population. No evidence of increased survival over time was found when improved survival in the general population was taken into consideration.
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is thought to reduce life expectancy although findings have varied between studies; estimates of average life expectancy have ranged from around 30 to 40 years from onset.1–10 Comparisons of all cause mortality with the general population indicate a two to three times greater risk of mortality associated with MS in Europe3 4 7–9 11 and North America.5 12 Findings as to whether MS survival is improving over time have been conflicting.3 4 7 13
The study of mortality and survival with MS is highly relevant to patients, their families and healthcare providers, and is important for health and resource planning. Clues to the underlying aetiology of the disease may be gained from a better understanding of survival and from the identification of risk factors that contribute to improved survival. Furthermore, a number of studies are now examining the impact of immunomodulatory drug treatments on mortality in MS; suitable survival data from appropriate geographical regions are needed for comparison. Finally, there is conflicting evidence surrounding predictors of survival that needs to be resolved. Although most studies report a survival advantage for younger compared with older onset MS patients,2 5–7 10 14 findings regarding the influence of sex and disease course have been mixed.4–7 9–11 13–16
We assessed absolute survival in a large Canadian MS cohort in British Columbia (BC) and the influence of sex, disease course at onset (primary progressive (PPMS) vs relapsing onset (R-MS)) and age at MS onset on survival. We also examined survival relative to the general population and estimated the excess hazard associated with sex, disease course, age at onset and time period of first clinic visit.
Methods
The cohort and data sources
The BC MS database was established in 1980 and collects information on MS patients seen at the four MS clinics in BC17 18; these clinics remained the only source of MS specialist care in the province until 2005. Clinical information including date of symptom onset and disease course was prospectively documented by clinic neurologists during visits and entered into the database. The cohort included all patients in the BC MS database who first visited a BC MS clinic between 1 August 1980 and 31 December 2004 and were diagnosed with definite or probable MS by Poser criteria.19 The BC Vital Statistics Agency captures more than 99% of deaths in BC. Between 1980 and 1985, the Agency directly informed the BC MS clinics of clinic patient deaths.12 Deaths that occurred between 1986 and 2007 were captured by linkage of the BC MS cohort to BC Vital Statistics data. Patients were linked at the individual level by their personal health number, a lifelong unique number assigned under BC's mandatory universal healthcare plan. Names and birth dates were used to confirm linkage accuracy. Once data were linked, all personal identifying information was removed.
To confirm residence in BC over the course of the study, the MS cohort was linked with the BC Ministry of Health Registry and Premium Billing Files, which includes registration dates for all BC residents enrolled in the universal healthcare plan. Patients were followed until the earliest of death, emigration from BC or study end (31 December 2007). In the event of unsuccessful linkage and unknown vital status by study end, patients were censored at their most recent clinic visit.
The University of British Columbia Clinical Research Ethics Board approved the study.
Statistical analyses
Absolute survival from birth (survival age) and from disease onset was estimated using the Kaplan–Meier method. Survival was compared between subgroups using the log rank test. For comparison with observed survival, life expectancy was calculated for the sex and age matched (at cohort entry) BC general population from life tables (2000–2002).20
The potential influence of ascertainment of ‘survivors’ during the early MS clinic years on the estimates and predictors of absolute survival was assessed by sensitivity analyses. Kaplan–Meier estimates and survival comparisons between subgroups were repeated after excluding patients with disease onset prior to 1970. The results of these restricted analyses were compared with those from the main analyses.
Standardised mortality ratios (SMRs) and corresponding 95% CIs were used to estimate mortality in the cohort relative to the general population. Statistics Canada's mortality rates for BC, by sex, calendar year and 5 year age band, were used as the population standard. An SMR greater than 1 indicates an excess risk of death in the cohort compared with the age, sex and calendar year matched general population. For all relative mortality analyses, follow-up began at the first clinic visit.
A Cox regression model for relative mortality21–23 was used to examine excess mortality associated with sex, disease course and onset age. Age, sex and calendar year matched BC general population mortality rates were entered as time dependent offsets, and thus excess mortality due to MS was multiplicative to the general population mortality rates. Results are expressed as relative mortality ratios (RMRs). An RMR greater than 1 indicates that the mortality ratio for this factor is higher than that associated with the referent. Potential interactions between covariates were assessed using stratified analysis.
The relative survival model was also used to explore the effects of time period of first clinic visit (1980–1985, 1986–1991 and 1992–1997) on survival time within 10 years while taking into account changing mortality rates in the general population. Only those patients with cohort entry between 1980 and 1997 were included to allow for comparable 10 year follow-up for each time period subgroup. To account for varying lengths of disease duration, relative survival analyses were adjusted for age at first visit (at cohort entry) in addition to onset age.21
Statistical analyses were performed using Stata V.11 (StataCorp 2009), R: A Language and Environment for Statistical Computing V.2.11.1 (R Foundation for Statistical Computing, Vienna, Austria; 2010) and Statistical Package for the Social Sciences V.15 (SPSS Inc 2006).
Results
The cohort
Between 1980 and 2004, 6917 patients with definite or probable MS visited a BC MS clinic. The demographic and clinical characteristics of the cohort are shown in table 1. The ratio of women to men was 2.6:1; this ratio was 1.3:1 in the PPMS group and 2.9:1 in the R-MS group. While the median age at disease onset was 31 years (range 3–75) overall, median onset age was approximately 12 years greater for PPMS (42 years; range 5–75) than for R-MS (30 years; range 3–75). Median age at the first clinic visit was 41 years (range 11–80) and the majority of patients (65%) were registered within 10 years of MS onset; 16.8% were registered within 1 year.
Characteristics of the British Columbia multiple sclerosis cohort
Most of the patients were never exposed to immunomodulatory or immunosuppressive therapy, and 89% of the follow-up time from disease onset predated exposure. At study end, 1025 (14.8%) patients had died and 5223 (75.5%) were alive. The remaining 669 patients were censored before study end due to emigration from BC (7.2%) or no linkage and unknown vital status (2.5%).
Absolute survival
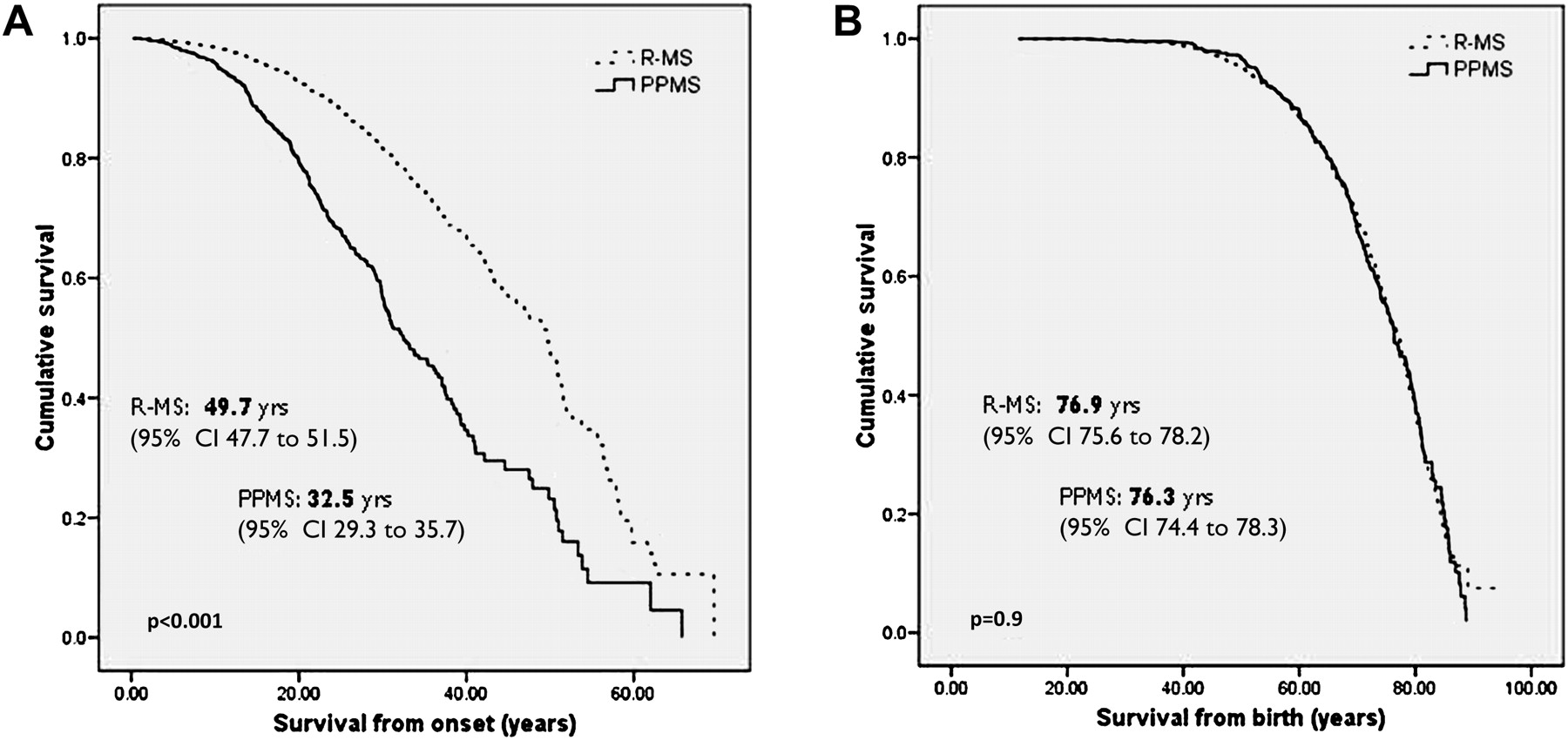
Overall median survival from onset was 47.5 years (95% CI 45.3–49.7) and median survival age was 76.7 years (95% CI 75.7–77.8). Women (figure 1A), R-MS patients (figure 2A) and those with a younger onset age (figure 3A) had significantly longer survival from disease onset. When survival was measured from birth, women survived to an older age than men (figure 1B). There was, however, no difference in survival age by clinical course at onset (figure 2B), and older onset patients (≥40 years) survived to an older age than younger onset patients (figure 3B).
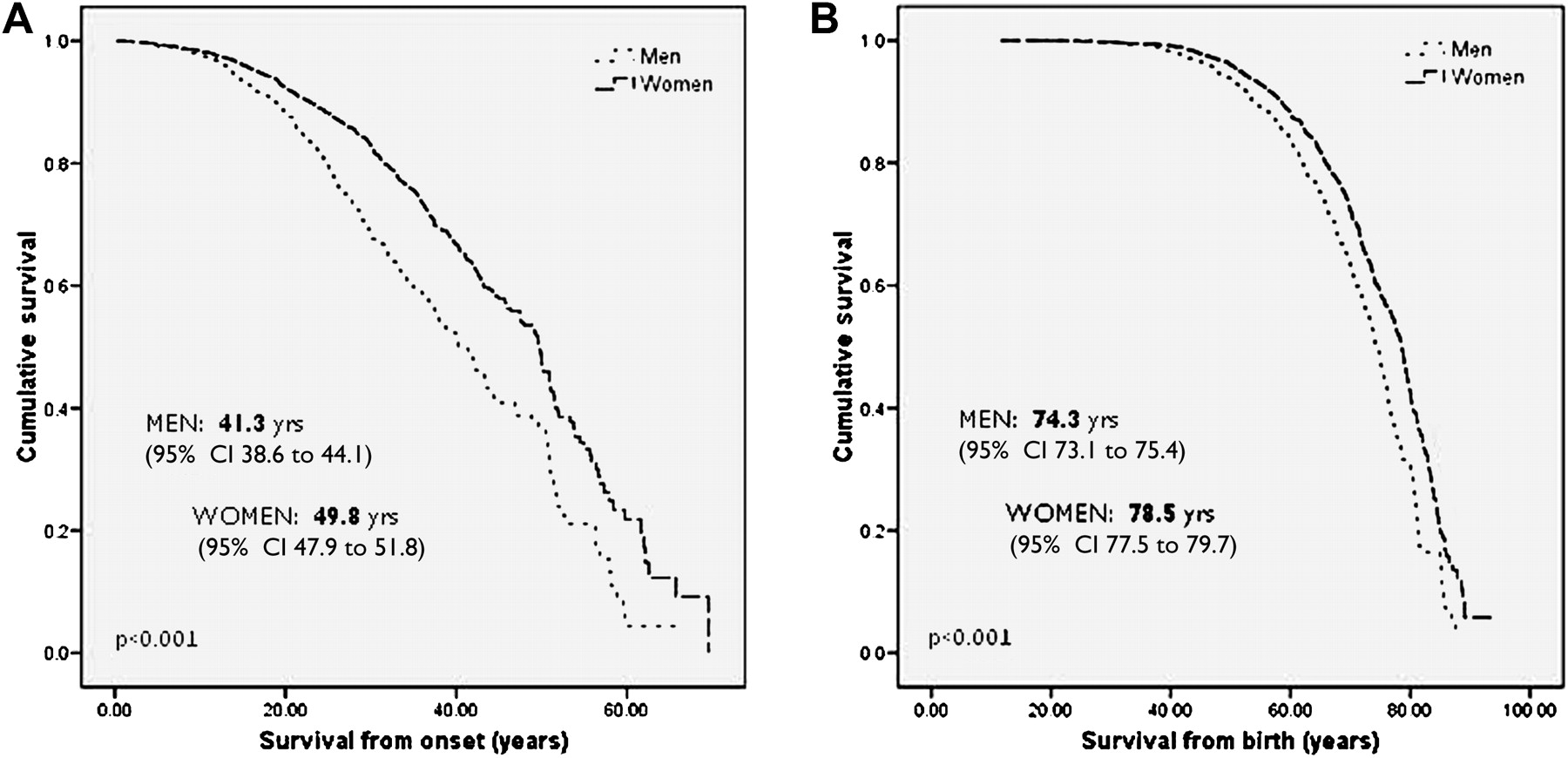
Kaplan–Meier survival curves showing survival from onset (A) and survival age (B) of the British Columbia multiple sclerosis patients by sex, with median survival times and 95% CIs.
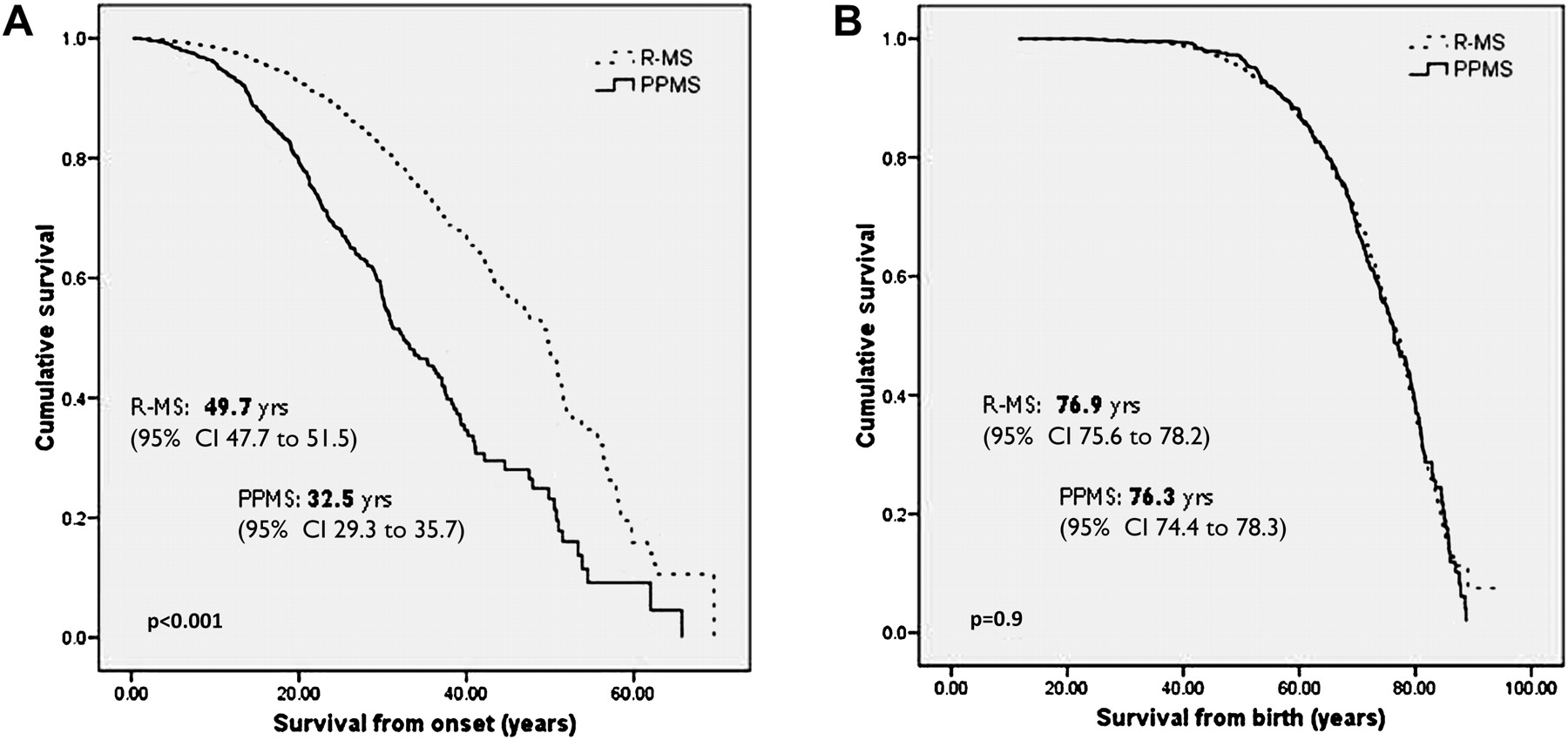
Kaplan–Meier survival curves showing survival from onset (A) and survival age (B) of the British Columbia multiple sclerosis patients by clinical course (primary progressive (PPMS) vs relapsing (R-MS)) at onset, with median survival times and 95% CIs.

Kaplan–Meier survival curves showing survival from onset (A) and survival age (B) of the British Columbia multiple sclerosis patients by age at disease onset, with median survival times and 95% CIs.
When the above analyses were restricted to patients with onset in 1970 or later (n=6223), median survival age was 77.4 years (95% CI 76.1 to 78.8). Median survival time from MS onset was not reached, however 75% survived to 30.3 years from onset; 2 years less than the equivalent survival time (32.3 years) for the entire MS cohort. Subgroup comparisons within this restricted cohort provided similar results to the main analysis.
Life expectancy relative to the BC population
Expected survival in the age matched BC general population was 84.5 years for women and 80.4 years for men; approximately 6 years longer than that observed in women and men with MS. The observed and expected survival from disease onset (conditional on surviving to age at first clinic visit) is demonstrated graphically in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves showing survival from onset of the British Columbia (BC) multiple sclerosis (MS) patients and expected survival of the BC general population (matched by sex and age at cohort entry, from 2000 to 2002 mortality rates).
Mortality risk relative to the BC population
For the SMR analysis, 6841 patients contributed 77 950 years of follow-up (76 patients from the original cohort were excluded because they contributed no follow-up time due to censoring at their first, and only, clinic visit). Of these 6841 patients, 5223 (76.3%) were followed until the end of the study period, 1025 (15%) until death and 593 (8.7%) until emigration from BC or their last clinic visit. The mortality risk in the cohort was nearly three times greater than in the general population (SMR 2.88; 95% CI 2.71 to 3.06). There was a significantly higher mortality risk for both men and women, and for those with either an R-MS or PPMS course (table 2). When stratified by onset age, relative mortality was highest in patients with onset before the age of 20 years (SMR 4.49; 95% CI 3.67 to 5.51). Relative mortality decreased with increasing onset age but remained significant in each age category. Mortality risk was between 2–3 times greater than expected when follow-up was restricted to the 10 years following cohort entry and stratified by time period of first visit (table 2).
Standardised mortality ratios and relative mortality ratios for the British Columbia multiple sclerosis cohort
Relative survival modelling (table 2) showed an increased mortality risk for PPMS compared with R-MS patients (RMR 1.53; 95% CI 1.30 to 1.80). The excess risk of death was reduced for those with an older onset age compared with those with onset before age 20 years. The relative mortality risk for women was slightly higher than that for men overall. However, further analysis with separate models for disease course indicated that there was an interaction between sex and disease course. The excess hazard for women was 55% higher than for men among those with PPMS (RMR 1.55; 95% CI 1.19 to 2.01) while the relative mortality risk for women with R-MS was no higher than that for men with R-MS (RMR 1.06; 95% CI 0.91 to 1.22).
Time period analysis
Of the 4109 patients with cohort entry between 1980 and 1997, 351 (9%) died within 10 years of their first clinic visit. Although the crude cumulative survival rate at 10 years was less (88.6%) for the 1980–1985 cohort than for the 1986–1991 (91.8%) and 1992–1997 (91.7%) cohorts, comparison of relative survival risk in the later cohorts to the earliest time period cohort provided no evidence of a change over time (table 2).
Discussion
MS in British Columbia, Canada, was associated with a 6 year reduction in expected lifespan and with nearly three times the risk of death compared with the age, sex and calendar year matched general population. However, we also report some of the longest median survival times in MS, with patients surviving approximately 48 years from symptom onset and living to an average age of 77 years (79 years for women and 74 years for men).
Our study is one of the largest of survival with MS and the largest in North America to date. We have contributed new findings by examining the average lifespan in MS according to important clinical and demographic factors, unavailable or unreported in many previous studies, including the following: sex, disease course (PPMS and R-MS) and age at symptom onset.
Others have observed a survival disadvantage for MS, ranging from 6 to 12 years; our estimate is comparable to the 6–7 year survival disadvantage reported in an earlier smaller Canadian study12 and slightly less than that reported in other cohorts.4 7 9 10 Differences in these estimates may be explained by variation in both the clinical characteristics of the MS populations and the survival expectations of the relevant general population, as well as assumptions and methods used to estimate expected survival. However, our finding that MS was associated with nearly three times the rate of mortality in the general population is similar to that reported in the majority of European3 4 7–9 and North American5 12 studies. While the SMRs cannot be directly compared because of potential differences in the age and sex distribution of cohorts, our findings together with those from other cohorts, indicate that men and women,3–5 7–9 24 as well as R-MS and PPMS patients,7 all have approximately three times the mortality risk of the general population.
Patients with MS onset at an older age did not survive as long from disease onset as younger patients, a finding that concurs with others.2 5 6 9 10 We found, however, that patients who were older at onset survived to an older age than their younger onset counterparts. Although this has not previously been demonstrated by survival studies in MS, studies of disease progression have reported a similar differential influence of predictors depending on whether the time to reach specific progressive milestones is evaluated in terms of age (from birth) or disease onset.25–29 In addition, whereas MS patients with a later onset age (≥40 years) had twice the mortality risk of the general population, mortality risk was four times greater for those with an early onset (<20 years of age). The relative impact of MS on mortality is higher in younger adults due to fewer competing risks for death at a younger age and, by definition, older onset patients cannot die with clinically recognised MS at a young age. Overall, patients who are older at disease onset may be considered to have a better outcome than those with a younger onset; not only have they lived disease free for a greater number of years, they can also expect to live to an older age, on average.
In terms of absolute survival, women with MS survived longer than men, irrespective of whether survival was measured from birth or onset. A longer survival for women from disease onset has also been reported for other cohorts,2 5 7 13 although not universally.1 6 10 14 On the other hand, our relative survival analysis, which accounts for the shorter life expectancy of men in the general population, showed that overall, women with MS fared no better than men with this disease. This also concurs with observations from other cohorts.2 5–7 11 14 15 Our findings were not consistent by disease course, however, and an excess hazard of death was evident for women with PPMS. The reason why women with a progressive course from onset carry a heavier relative mortality burden than men with the same clinical course is unclear, but warrants further study.
When measured from onset, we found longer survival for R-MS compared with PPMS. This is consistent with findings from other studies,1 6 7 9–11 14 and is perhaps not surprising considering that symptoms of PPMS typically present at a later age. On the other hand, we found that PPMS and R-MS patients survived to the same age; a similar observation was made in the only other study examining this outcome.9 Nonetheless, a greater risk of mortality for those with PPMS became evident once onset age and the general population mortality risk were taken into account. The reduced survival time for primary progressive patients coupled with the extended delays that they experience to diagnosis or referral to a specialist neurologist30–32 leaves a relatively brief window of time during which any new potential interventions that may influence quality of life, disease progression or mortality can be offered.
We found no evidence of improved relative survival over time (1980–2007). Survival increased for those with MS but this improvement mirrored that seen in the general population. Results were similar for a small Norwegian study7 although a small increase in relative survival has been observed in Denmark since the 1950s.3 4 Others have reported either no evidence of changing trends in MS mortality over time6 13 14 or improved survival;1 these studies did not, however, consider changes in general population mortality rates.
The potential influence of ascertainment bias was assessed by estimating survival only for patients with a maximum disease duration of 10 years when the clinics first opened in 1980, allowing for a reasonable diagnostic delay of up to 10 years during that period.31 33–35 The survival age of these patients was similar to that of the whole cohort but survival from onset was approximately 2 years shorter. This is not unexpected and indicates that our absolute survival estimates may be slightly longer than that experienced by the incident BC cohort while the overall estimated survival times still appear robust. Nonetheless, direct comparisons of survival estimates from MS cohorts are complicated by different ascertainment methods such as whether incidence, prevalence or mixed cohorts are used.4 6–11 14 15 36 We have based our findings, like many others, on the mixed approach.
The strengths of our study include: the substantial population of MS patients with 27 years of prospective follow-up and all with a clinical diagnosis confirmed by an MS specialist neurologist; and the population based nature of the BC MS database, which captures approximately 80% of MS patients in BC. The reasons why the remaining patients do not attend BC MS clinics are unknown but might include issues with physical access to the clinics or very mild disease. We have no reason to believe that the survival of patients who attend BC MS clinics is different to those who do not. Furthermore, the distribution of sex, age at onset and clinical course in the BC MS cohort is comparable with that reported in other MS cohorts.7 11 18 Linkage of the BC MS data to BC administrative data ensured reliable coding of death and minimal loss to follow-up; vital status was unknown for less than 10% of the patients at the study end due to either emigration or unsuccessful linkage with the administrative databases. Some cases with a severe disease course may have been missed if they died soon after diagnosis but before they attended a BC MS clinic; this scenario is considered rare and the potential impact of such severe missed cases is likely to be minor. The vast majority of patients in the BC MS database are of Northern European descent; it is estimated that less than 5% of the cohort is of Asian, North American, Aboriginal or other ethnicity.37 38 These findings are therefore mostly generalisable to MS patients of Northern European descent; other ethnicities may experience different survival outcomes.
As with any study that relies on diagnosis, identification or registration of patients some time after symptom onset, our findings are only generalisable to patients who survive long enough to be diagnosed with MS and registered at a clinic. Our study was not designed to address the impact of disease modifying therapies on mortality, and the cohort included treated and untreated patients. Very little of the follow-up time from disease onset post dated first exposure to therapy, however, and the vast majority of deaths were among unexposed patients; any potential effects of treatment on the overall findings are therefore likely negligible.
In summary, we report some of the longest survival times in MS although the mortality risk was still greater, and the average lifespan was 6 years shorter, than that seen in the general population. Onset over the age of 40 was associated with a longer lifespan compared with younger onset patients. While women lived longer than men with MS, the sex difference among R-MS patients was no greater than that observed in the general population. Among those with PPMS, women had a greater relative survival disadvantage than men; this deserves further study. Survival within 10 years of first clinic visit remained stable over 18 years of patient enrolment.
Acknowledgments
We are grateful to Tom Duggan, Research Assistant, Division of Neurology, University of British Columbia, for his help with data manipulation and coding, and to Population Data BC and the BC Ministry of Health for support with accessing BC administrative health and Vital Statistics data. Special thanks to the BC multiple sclerosis clinic neurologists: D Adams, D Craig, L Daly, V Devonshire, S Hashimoto, O Hrebicek, J Hooge, B Jones, L Kastrukoff, S Meckling, D Parton, D Paty, A Sayao, P Smyth, W Shtybel, T Traboulsee and to the BC multiple sclerosis clinic patients for sharing clinical information.
References
Footnotes
Funding This study was funded by the Canadian Institutes of Health Research (MOP-82738; PI: HT). EK is funded by a Postdoctoral Fellowship from the Multiple Sclerosis Society of Canada. AS is funded through grants from the Canadian Institute of Health Research (MOP-93646; PI: HT) and the National Multiple Sclerosis Society (RG 4202-A-2; PI: HT), and a Postdoctoral Fellowship from the Multiple Sclerosis Society of Canada. YZ receives research funding from the Canadian Institutes of Health Research, the Multiple Sclerosis Society of Canada and the National Multiple Sclerosis Society. JO receives financial support from the Christopher Foundation (Vancouver) and the University of British Columbia. HT is funded by the Multiple Sclerosis Society of Canada (Don Paty Career Development Award); is a Michael Smith Foundation for Health Research Scholar and the Canada Research Chair for Neuroepidemiology and Multiple Sclerosis. HT receives research support from CIHR, the MS Society of Canada and the US National MS Society. The BC MS database has been funded by an unrestricted grant from Dr Donald Paty and the MS/MRI Research Group. The funding agencies had no role or involvement in the study design or conduct, data collection, analysis or interpretation, manuscript preparation or the decision to submit the paper for publication.
Competing interests EK has received reimbursement of travel and accommodation costs to present at and attend conferences from the endMS Research and Training Network, the International Society for Pharmacoepidemiology and Bayer Schering Pharma. AS has received travel grants to present and attend conferences from the endMS Research and Training Network and the European Committee for Treatment and Research in Multiple Sclerosis. JO has received speaker honoraria, consulting fees, travel grants, research grants or educational grants from Aspreva, Aventis, Bayer, Biogen-Idec, BioMS, Corixa, Genentech, Novartis, Serono, Talecris and Teva-neurosciences and receives fees for services from Bayer, Novartis and Biogen Idec to serve on advisory committees. HT has received research support from the MS Society of Canada, the US National MS Society, Canadian Institutes of Health Research and UK MS Trust. She has received speaker honoraria and/or travel expenses to attend conferences from Consortium of MS Centres, US National MS Society, Swiss Multiple Sclerosis Society, the University of British Columbia MS Research Program, Bayer Pharmaceuticals (speaker; honoraria declined) and Teva Pharmaceuticals (speaker). Unless otherwise stated, HT's speaker honoraria are donated to an MS charity or to an unrestricted grant for use by her research group.
Ethics approval This study was conducted with the approval of the University of British Columbia Clinical Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.