Article Text

Abstract
Background Staging of disease severity is useful for prognosis, decision-making and resource planning. However, no commonly used, validated staging system exists for amyotrophic lateral sclerosis (ALS). Our purpose was to develop an ALS staging system (ALS Milano-Torino Staging) that captures the observed progressive loss of independence and function.
Methods Clinical milestones in ALS progression were defined by loss of independence in four key domains on the ALS Functional Rating Scale (ALSFRS): swallowing, walking/self-care, communicating and breathing. Stages were defined as follows: stage 0, functional involvement but no loss of independence on any domain; stages 1–4, number of domains in which independence was lost; and stage 5, death. Staging criteria were applied to patients enrolled in a Quality of Care in ALS (QOC) study; endpoints included function (ALSFRS), quality of life (QOL; Short Form-36) and health service costs. Between-stage transition probabilities were assessed in the QOC study and in a second clinical study of lithium carbonate in ALS.
Results 70/118 (59.3%) participants in the QOC study progressed to higher stages of disease at 12 months compared with their baseline stage. Functional (ALSFRS) and QOL measures were inversely related to disease stage. Health service costs were directly related to increasing disease stages from 0 to 4 (p<0.001). Probabilities for transitioning from a given stage at baseline in both studies were usually greatest for the next highest stage.
Conclusions The proposed ALS Milano-Torino Staging system correlates well with assessments of function, QOL and health service costs. Further studies are warranted to validate this system.
- ALS
- Quality of Life
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is an idiopathic neurodegenerative disease that affects motor neurons, typically leading to death within 3 years of symptom onset.1 ALS is characterised by a progressive loss of functions such as speech, swallowing, mobility and respiration. Functional rating scales such as the ALS Functional Rating Scale (ALSFRS)2 and ALSFRS–Revised (ALSFRS-R)3 are useful to measure functional decline and have been used to evaluate treatment effects on function in clinical trials.4–8 However, ALSFRS/ALSFRS-R may not fully capture the functional characteristics of later-stage ALS progression9 ,10 and there is no agreed-upon threshold at which a change in ALSFRS/ALSFRS-R score is viewed as an important transition point in functional status.
Definition of discrete stages of disease progression based on such clinical milestones can be a useful tool for prognosis, therapeutic decision-making, assessment of quality of care and resource allocation.11 A staging system also allows patients and caregivers to understand the disease and its clinical course better. In the case of ALS, a valid staging system should correlate with ALS disease progression and demarcate meaningful differences in quality of life (QOL) and economic burden. Although staging systems for ALS have been proposed,12 ,13 currently there is no commonly used system. The lack of a validated staging system for ALS makes it difficult to quantify the degree of clinical, socioeconomic or QOL impact of a therapeutic intervention.
We sought to develop an ALS staging system that captures the observed progressive loss of independence and function and to apply it to the evaluation of patients’ clinical outcomes, QOL and costs in ALS.
Methods
Patients and measures
We used data from the Quality of Care in ALS (QOC) study,14 a prospective study of consecutively enrolled patients (aged ≥18 and ≤80 years) from 11 Italian ALS centres (2001–2002) to develop and evaluate the proposed ALS staging system. Patients were included in the QOC study if they met El Escorial revised criteria for definite, probable or probable laboratory-supported sporadic ALS.15 Ethical approvals were obtained from institutional review boards at each participating study centre. Exclusion criteria included participation in ongoing clinical trials, familial ALS, ALS plus syndrome, ALS frontotemporal degeneration and serious medical conditions requiring care (eg, cancer, ischaemic heart disease, chronic obstructive pulmonary disease and renal insufficiency).
Patients were recruited between 15 February 2001 and 15 January 2002 and were evaluated at study entry and at 4-month, 8-month and 12-month follow-up visits. At each study visit, patients were evaluated for functional status using the 10-item ALSFRS, health-related QOL (HRQOL) using the Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36),16 and overall individual QOL using the Schedule for the Evaluation of Individual QOL–Direct Weighting (SEIQOL-DW).17 ,18 This is a participant-generated measure that allows an estimation of the QOL subjectively perceived by the patient. The SF-36 has been validated for the Italian population.19
Direct health service costs were obtained from ad hoc forms completed at each study visit. Patients were requested to complete a daily diary including all uses of health system provisions. All direct costs were analysed, including hospital admissions, nursing care admissions, day hospital visits, clinic visits, diagnostic examinations, pharmacologic treatments, nursing care, rehabilitation interventions, psychological support, visits by the general practitioner, provisions for mobility aids and communication. Indirect costs were not considered. The cost of each service was obtained from the official costs for years 2001–2003 provided by the Italian National Health System.
We examined between-stage transitions using both QOC study data and data from a second study, an interventional clinical trial of lithium carbonate in ALS (LiTALS study; EudraCT number 2008-001094-15) for which detailed methods have been published previously.20 Briefly, 171 patients (aged ≥18 and ≤75 years) from Italian ALS study centres were enrolled between 2 May 2008 and 15 April 2009 in a 15-month trial comparing postulated therapeutic (n=87) and subtherapeutic (n=84) levels of lithium carbonate (2008–2009). Patients had mild to moderate disease (ALS onset ≤36 months; ALSFRS-R scores: swallowing ≥3; cutting food and walking ≥2; respiratory capacity ≥3) and were allowed to take riluzole if they had been on a stable dose for at least 2 months. ALSFRS-R was performed at randomisation and follow-up months 1, 3, 6, 9, 12 and 15. The LiTALS study was terminated early due to lack of efficacy and occurrence of adverse events.
Definition of ALS Milano-Torino Staging in the QOC study
Critical milestones in ALS progression were defined by loss of independent function in four key domains that are included in both ALSFRS and ALSFRS-R and that involve loss of autonomy: walking/self-care, swallowing, communicating and breathing (table 1). Impairment in each domain was determined by thresholds that reflected loss of autonomy in the specific ALSFRS 10-item scale scores. Values of 0 (below threshold) or 1 (above threshold) were assigned, and the stages were determined as the sum of those values across the four domains. Stages were defined as follows: stage 0, functional involvement but no loss of independence on any domain; stages 1–4, number of domains in which independence was lost; and stage 5, death (table 1). The staging system was given the name ALS Milano-Torino Staging (ALS-MITOS).
Functional domains and stages
Statistical analysis
ALS-MITOS stage was calculated for each participant visit in the QOC and LiTALS studies. We examined the distribution of ALS stage at 12 months by baseline ALS stage using descriptive statistics. The distribution of ALSFRS score at each observed stage during follow-up was evaluated. Transition probabilities for each study were calculated by a Markov model.21 Cost data were analysed using analysis of variance. Trends in cost data and SF-36 comparisons among the stages and throughout the follow-up were evaluated using the Kruskal–Wallis test.
Results
In the initial analysis from the QOC study, a total of 130 patients (56 females, 74 males) met the inclusion criteria (figure 1A). The mean age of ALS onset was 57 years, with an average time of 2.5 years since symptom onset (table 2).
Baseline characteristics
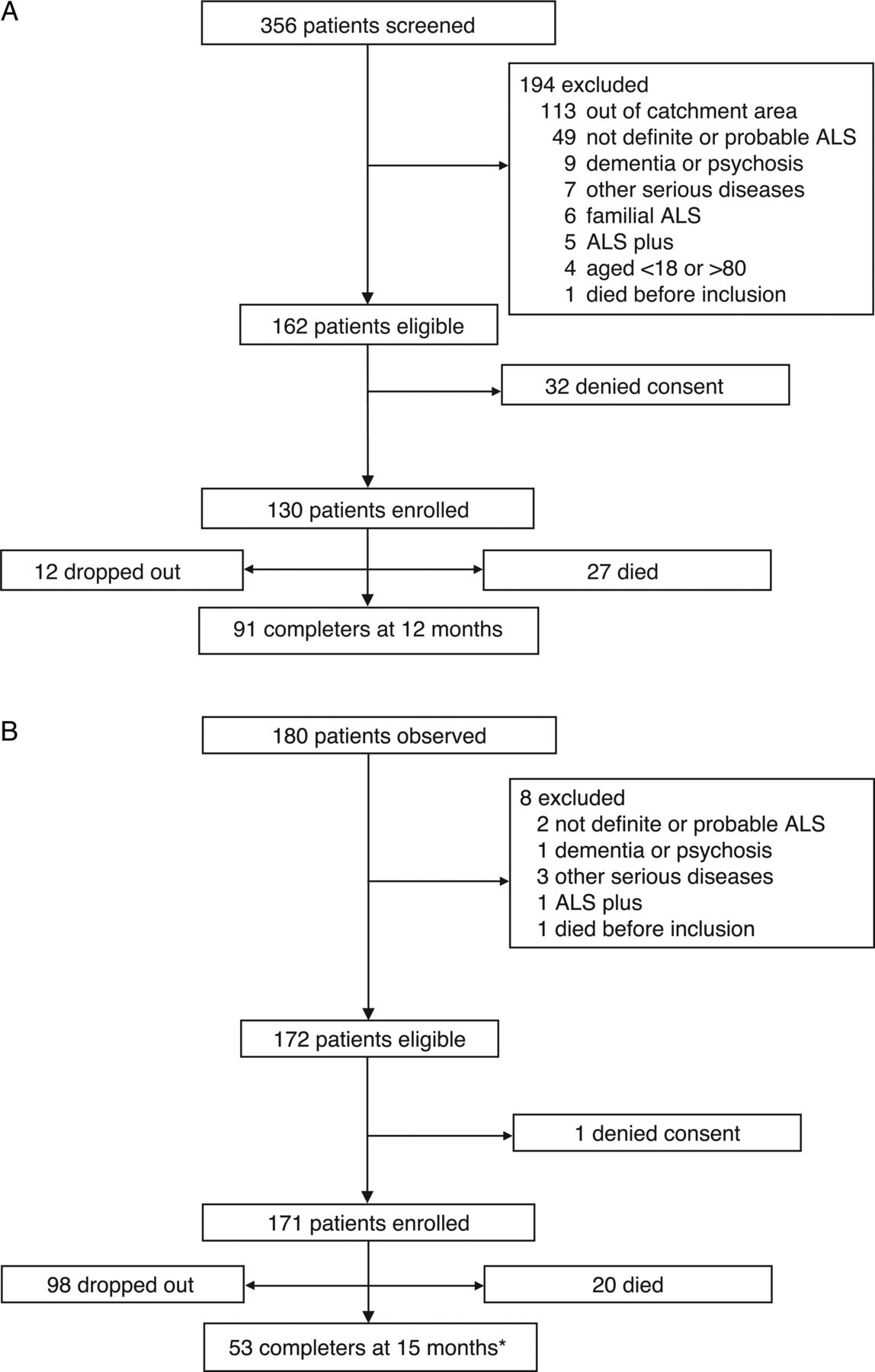
(A) Patient disposition in the Italian study of the Quality of Care in ALS. (B) Patient disposition in the LiTALS study. *Includes patients enrolled but not completed at study termination. ALS, amyotrophic lateral sclerosis; LiTALS, lithium carbonate in ALS study.
In the QOC study, most patients (64%) were diagnosed with definite ALS, followed by probable laboratory-supported ALS (22%) and probable ALS (14%). The majority (66%) of patients had spinal ALS onset. At baseline, the mean ALSFRS score was 24.5 (SD 9.7); 55% of the patients were unable to move or required adaptive aids, 21.5% could not communicate by speech, 24.6% had enteral feeding and 21% needed ventilator assistance. Rehabilitation therapies (physical and speech therapy) were used at baseline by 67% and 20% of patients, respectively. Use of adaptive aides included wheelchairs (28.5%) and walkers (14%). The remainder of the palliative care milestones had not yet been reached by most patients. For example, at baseline, fewer than 10% of patients had recourse to paid home care or psychosocial care resources, had prepared for end-of-life care or had used ameliorative or life-extending (percutaneous gastrostomy tube, non-invasive ventilation or tracheotomy) technologies. Eighty per cent of patients used riluzole and 40% used creatine or vitamin E, whereas use of a psychopharmaceutical, anticholinergic to control drooling or antispasticity drugs was rare. Finally, 2% of the cohort had used the emergency department and none was in hospice at baseline. A spouse was the primary caregiver for 72% of patients and spent a median of 13 h/day caring for the patient. Thirty-two patients received home healthcare services, of which 60% were private.
In the LiTALS study, 171 patients (71 females, 100 males) had an average age of onset of 57 years, most (75%) had spinal ALS onset and the mean ALSFRS-R score at baseline was 36.9 (figure 1B, table 2). A more complete description of the study population has been published previously.20
In the analysis of progression by baseline stage in the QOC study, among the 130 enrolled subjects, most patients at baseline were in stage 0 (n=65; 50%) or stage 1 (n=31; 23.8%); 7.7% (n=10) were in stage 2, 3.1% (n=4) were in stage 3 and 6.2% (n=8) were in stage 4. At 12 months, 12 subjects were lost to follow-up. Among the 118 subjects who either completed the study or died, 59.3% (n=70) of patients within each of the stages at baseline had progressed to more advanced stages of disease (figure 2). Overall, among the 118 subjects at 12 months, 19.5% of patients were in stage 0, 22.9% were in stage 1, 17.8% were in stage 2, 5.9% were in stage 3, 11.0% were in stage 4 and 22.9% were in stage 5 (death). In the QOC study, only three patients did not complete the SF-36 questionnaire. At the domain level, the proportion of missing replies ranged from 2% to 4%. The HRQOL in ALS patients was consistently lower than that of published Italian norms19 across all domains of the SF-36 and decreased with increasing stages (figure 3A). The SF-36 physical and mental health composite scores (mean±SD) were 30.5±10.3 and 43.3±12.3, respectively, at baseline and decreased with increasing stages (figure 3B). The Italian National Health Service mean total costs per patient per year increased with progress to each consecutive stage (figure 4).

ALS stage at 12 months by baseline stage in the Quality of Care in ALS study. ALS, amyotrophic lateral sclerosis.

(A) SF-36 domain by ALS stage for all patients in the Quality of Care in ALS (QOC) study at baseline and normal controls. *n=patient visits, numbers differ owing to number of missing values in different domains. †p Value for trend, stages 0–4, Kruskal–Wallis test. (B) Composite scores by ALS stage for all patients in the QOC study at baseline. ††p<0.001 compared with stage 0. ‡p<0.01 compared with stage 0. ALS, amyotrophic lateral sclerosis.
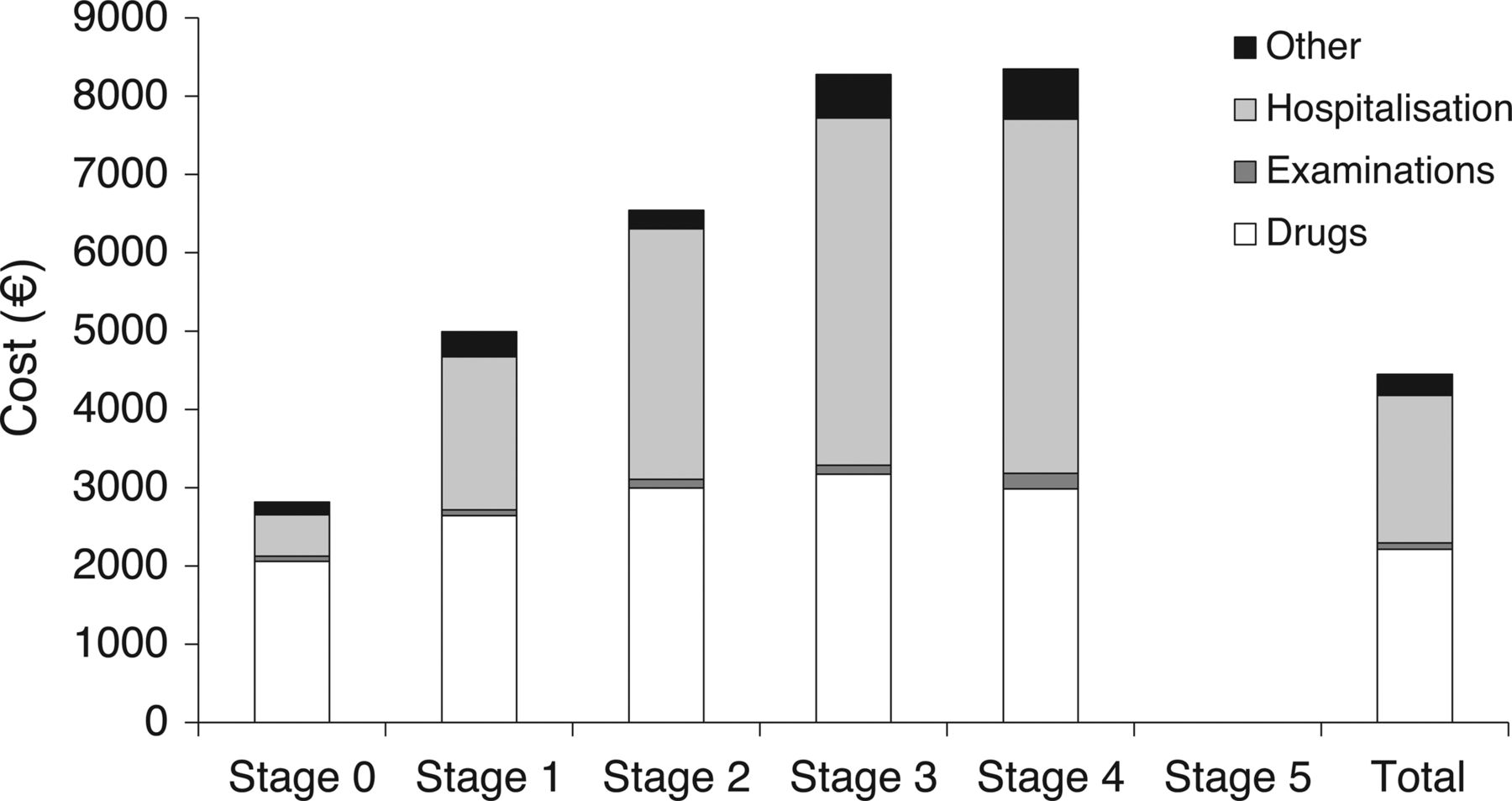
ALS costs over the 1-year study period by ALS-MITOS stage* in the Quality of Care in ALS study. *Includes each stage for all patients.ALS, amyotrophic lateral sclerosis; ALS-MITOS, Amyotrophic Lateral Sclerosis Milano-Torino Staging. p<0.001 for drugs, examinations and treatments. p=0.009 for hospitalisation.
In the analysis of progression by baseline stage in the LiTALS study, all patients at baseline were in stage 0 (80.3%) or stage 1 (19.7%), reflecting the study enrolment criteria (disease onset, 36 months; mild-to-moderate disability, as indicated by ALSFRS-R score 3 for swallowing, 2 for cutting food and walking and 3 for respiratory failure). In total at 12 months, 22.4% were in stage 0, 35.5% were in stage 1, 10.5% were in stage 2, 5.3% were in stage 3 and 26.3% were in stage 5 (death).
Probabilities for transition between stages were calculated based on the data for each study. In the QOC study, the probability of transition from a given stage was highest for the next highest stage (figure 5A). There were relatively few instances in which a stage was ‘skipped’. Only four reversions were observed, one transition from stage 1 to stage 0, two from stage 3 to stage 2 and one from stage 4 to stage 3. These reversions were related to the breathing domain (two cases, with a reversion from score 2 to score 3 in the breathing item of the ALSFRS scale); the eating domain (one case with reversion from score 1 to score 2 in the swallowing domain); and the movement domain (one case, with reversion from score 1 to score 2 in the dressing domain). The probability of death increased stepwise from stage 0 to stage 3 and 4. It should be noted that 17 patients underwent tracheostomy during the study period or were already on tracheostomy at the inclusion in the study, and of these, only one died.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Probability of transition between ALS-MITOS stages in the Quality of Care in ALS study. (B) Probability of transition between ALS-MITOS stages in the LiTALS study. ALS-MITOS, Amyotrophic Lateral Sclerosis Milano-Torino Staging; LiTALS, lithium carbonate in ALS.
As shown in figure 5B, probabilities for transition from a given stage in the LiTALS study were also usually highest for the next highest stage compared with any other higher or lower stage. For stages 0, 1, 3 and 4, the highest probabilities were evident for transitions to the next highest stage. Patients in stage 0 and stage 1 had lower probabilities of ‘skipping’ intervening steps, and only stages 1 and 2 were associated with any probability of reversion to a previous stage. However, patients in stage 2 were equally likely to progress to stage 3 or revert to stage 1. The probability of death showed stepwise increases with increasing stage up to stage 2, remained relatively constant between stages 2 and 3 and then increased to 1.0 at stage 4.
Discussion
We have shown that the proposed ALS-MITOS staging system, based on the validated ALSFRS/ALSFRS-R, identified relevant stages of disease in these patients. This approach partitions individuals with ALS into the relevant stages through which they progress according to the number of important life functions lost. The distribution of patients across these stages and the probabilities of transition between stages were consistent with sequential disease progression with increasing stage. In the QOC study, the QOL and healthcare costs of patients with ALS also were correlated with the ALS-MITOS clinical stage.
A strength of this staging system is the fact that it is based on the ALSFRS/ ALSFRS-R, which is a tool already familiar to most ALS clinicians and one that is widely used in clinical trials. Thus, this staging system can be readily incorporated as an endpoint in clinical trials to allow investigators to evaluate treatment impact on different ALS stages without a requirement for additional assessments.
Roche et al13 proposed a staging system based on clinical milestones such as symptom onset, diagnosis and subsequent disease progression. Their system, based on an analysis of 1471 patients in a tertiary referral centre clinical database, demonstrated predictability of occurrence of milestones throughout the disease course. However, it differs from the current proposed system in that it is not based on critical milestones defined by loss of independent function in key domains for the patients’ life, but rather on both clinical milestones with little direct consequence for key functions relevant to the patient (ie, diagnosis, involvement of a second or third region) and impairment or loss of two specific functions (need for gastrostomy or non-invasive ventilation). Another staging system consisting of six stages was developed to facilitate rehabilitation of patients with ALS but is not necessarily useful to ascertain overall disease progression and also cannot be applied to early disease progression.12
The use of ALSFRS items as the basis of this system should facilitate further retrospective validation studies using existing databases that collected functional data using that scale. Furthermore, this system may enhance physicians’ ability to have a meaningful discussion with patients and caregivers about what to expect as the disease progresses. In addition, resource needs evolve with progression of disease, as earlier stages require diagnostics, intermediate stages may involve various specialties and later stages require palliative care.22 Thus, a validated staging system should help with resource planning.
Although these initial analyses may support the validity of the ALS-MITOS staging system, it is important to point out the limitations of this study. For example, it was not possible to determine the amount of time spent in the baseline stage prior to study entry because stages were not assessed retrospectively. The small sample size limited an assessment of changes in the stage distribution from baseline to later assessment time points and may be too small to reach any definite conclusions. Stage transitions and the relationship between this staging system and clinical outcomes such as mortality could not be evaluated because of the short follow-up time and small sample size. The initial staging assessment may have been impacted by the long time from symptom onset to study entry (2.5 years in the initial study). The possibility that a few patients ‘skipped’ a stage or reverted to an earlier stage may reflect differences in the rates of disease progression, but confirming that possibility would require analysis of larger clinical datasets that also included long-term outcomes (eg, mortality). The study data included in the current analyses also did not include sufficient numbers of patients with bulbar onset or both bulbar and limb onset to allow any meaningful comparison with limb onset ALS. Finally, because patients with frontotemporal degeneration were excluded, and this system does not capture the impact of cognition, an important aspect of ALS, it is not clear how cognitive impairment might affect staging of disease.
The potential limitations of the ALS-MITOS system are likely be more than compensated by its utility because it is based on a well-validated and widely used rating scale. Thus, it has the potential to provide meaningful information to clinicians and patients. Furthermore, it can be readily applied to existing datasets to further establish its validity and to facilitate direct comparisons with future studies. Further investigation of transitions through stages and associated changes in costs and QOL would add to our understanding of the utility of this proposed system.
Conclusions
The results of this study are sufficiently compelling to warrant further evaluations of the ALS-MITOS system of staging.
References
Footnotes
-
Contributors AC and GM were involved in designing the QOC and LiTALS studies, and in collecting and analysing and interpreting patients’ data. GF and VB were involved in designing the QOC study, and in collecting and analysing and interpreting patients’ data. ERH performed statistical analyses for the LiTALS study. All authors reviewed drafts and approved the final version of this manuscript for submission.
-
Funding The Italian study of Quality of Care in ALS was funded by the Italian Ministry of Health (grant number 030.3/RF99.40). The Lithium Carbonate in ALS study was supported only by participating study centres in Italy. Biogen Idec provided funding for editorial support in the development of this paper; Ed Parr of Excel Scientific Solutions wrote the first draft of the manuscript based on input from authors, and Linda Cirella of Excel Scientific Solutions copyedited and styled the manuscript per journal requirements. Biogen Idec reviewed and provided feedback on the paper to the authors. The authors had full editorial control of the paper and provided their final approval of all content.
-
Competing interests AC serves on a scientific advisory board for Biogen Idec and Cytokinetics. ERH served as a paid consultant to Biogen Idec for the LiTALS study analyses. GM, VB and GF report no conflicts of interest.
-
Ethics approval Institutional approval received for original studies included in relevant citations.
-
Provenance and peer review Not commissioned; externally peer reviewed.