Article Text

Abstract
Objective The role of diet in multiple sclerosis (MS) course remains largely unknown. Children with MS have a higher relapse rate compared with MS in adults. Thus, studying the effect of diet on relapse rate in this age group is likely to provide more robust answers.
Methods This is a multicentre study done at 11 paediatric MS centres in the USA. Patients with relapsing-remitting MS (RRMS) or clinically isolated syndrome (CIS) with disease onset before 18 years of age and duration of less than 4 years were included in this study. Dietary intake during the week before enrolment was assessed with the validated Block Kids Food Screener. The outcome of the study was time from enrolment to the next relapse. 219 patients with paediatric RRMS or CIS were enrolled. Each 10% increase in energy intake from fat increased the hazard of relapse by 56% (adjusted HR 1.56, 95% CI 1.05 to 2.31, p=0.027), and in particular each 10% increase in saturated fat tripled this hazard (adjusted HR: 3.37, 95% CI 1.34 to 8.43, p=0.009). In contrast, each additional one cup equivalent of vegetable decreased the hazard of relapse by 50% (adjusted HR: 0.50, 95% CI 0.27 to 0.91, p=0.024). These associations remained with mutual adjustment and persisted when adjusting for baseline 25(OH) vitamin D serum level. Other studied nutrients were not associated with relapse.
Conclusions This study suggests that in children with MS, high energy intake from fat, especially saturated fat, may increase the hazard to relapse, while vegetable intake may be independently protective.
- Pediatric
- Multiple sclerosis
- relapse
- Diet
- Fat intake
- Vegetable intake
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is a disease with unknown aetiology, but in which environmental factors and genetic polymorphisms play a role.1 Prior infection with Epstein-Barr virus, vitamin D insufficiency and exposure to cigarette smoking have shown a consistent association with increased risk of MS development and disease course in adults.2–4
The role of diet in disease susceptibility and course remains largely unknown. In an animal model of MS, a high-fat diet increases immune cell infiltration and inflammatory mediator production in the central nervous system (CNS).5 In humans, MS susceptibility may be higher in individuals with higher saturated fat intake,6 while consumption of fruit and vegetables may be associated with reduced patient-reported relapse rate and disability.7 Neither of these reports have been confirmed nor have used medically confirmed MS relapses or longitudinal prospectively collected data.
Children have a higher relapse rate compared with MS in adults. Thus, studying the effect of diet on relapse rate in this age group is likely to provide more robust answers.8 Our large ongoing study of environmental and genetic risk factors for paediatric MS includes the collection of dietary intake at enrolment. We report findings from the first multicentre cohort of patients with paediatric MS investigating the longitudinal and prospective association between dietary intake and relapse risk.
Methods
Data were derived from a collaborative paediatric MS study conducted at 11 paediatric MS centres in the USA. Cases were recruited between December 2011 and January 2016. Institutional review boards at each of these sites approved the study. All the participants and one of their parents/legal guardians signed the informed assent and consent.
Study participants
Eleven centres participating in the study on risk factors for paediatric MS entered prospective relapse information into the US Pediatric MS Network database.9 The study enrolled patients with relapsing-remitting MS (RRMS) or clinically isolated syndrome (CIS) at high risk of MS who had at least two silent MRI lesions, with disease onset before 18 years of age and disease duration of less than 4 years.10 Patients who completed the food frequency questionnaire and had available prospective relapse data subsequent to enrolment in the study were included in this analysis.
Clinical and demographic information
Case ascertainment was performed by a panel of at least two paediatric MS experts listed as coauthors. Race and ethnicity were self-reported according to National Institutes of Health criteria. Medical history including relapse rate was collected by each participating centre at the time of follow-up clinic visits. Relapses were defined as new or recurrent neurological symptoms localising to the CNS, lasting for at least 24 hours after a remission of 30 days or more since the previous attack in the absence of an infection or fever.11 Only relapses that occurred after enrolling in the study were used for the analyses. Disease duration at the time of enrolment was calculated from the date of the first demyelinating event to the time of study enrolment. Follow-up duration was calculated from the time of study enrolment to the end of available follow-up. Baseline serum 25(OH) vitamin D level was measured as a batch by chemoluminescence at Heartland Assays laboratory.
Nutrient and energy intake assessment
Dietary intake was assessed using the Block Kids Food Screener (BKFS) (NutritionQuest, 2007).12 BKFS is a validated food frequency questionnaire designed for children between 2 and 17 years of age and is available in English and Spanish. The questionnaire was completed by children or their caregiver one time at the enrolment in the study after getting instruction from a research staff member. The questionnaire consists of 41 questions evaluating the frequency and portions of food and beverages consumed during the past week. Patients were instructed to select the frequency (none last week, 1 day, 2 days, 3–4 days, 5–6 days and every day) and then the food-specific portion size (eg, one slice, two slices and 3+ slices) that most closely matched their intake in the preceding week. Five age–sex categories were used to provide dietary estimates: males/females 4–8 years old, males 9–13 years old, males 14–17 years old, females 9–15 years old and females 16–17 years old. Subjects were excluded if >15 answers were missing or if reported estimates reflected biologically implausible daily energy intakes (<500 or >5000 kcal/day) based on NutritionQuest food screener analysis. The BKFS has been validated against three 24 hours dietary recalls in children aged 10–17.13
We examined average daily intake of energy, saturated and unsaturated fat, vegetables (measured as cup equivalents, excluding potatoes and legumes), fruit (measured as cup equivalents), cholesterol, fibre, carbohydrate, dairy and iron. Energy intake from fat was calculated as a percentage of daily calories that come from fat, which is equal to 100*(9*fat)/energy. Similarly, energy intake from carbohydrate or protein is the percentage of daily calories that come from carbohydrates or protein and are equal to 100*(4*carbohydrate)/energy and 100*(4*protein)/energy, respectively.
Statistical analysis
The group of patients who experienced a relapse during follow-up was compared with the group of those without relapse with respect to baseline characteristics. For continuous variables, a Wilcoxon rank-sum test was used, with a χ2 test used for categorical variables.
We estimated the risk of relapse using the multivariate Cox proportional hazard model by calculating the HR and 95% CI. The outcome of the study was time from enrolment to the next relapse. Descriptive statistics for patient characteristics were presented either as percentages (%) or using mean and SD. Nutrient intakes were calculated as continuous variables, and some were categorised based on the minimally recommended total intake for the child’s age group or using tertiles. For all models, we adjusted for total energy intake.
The multivariate Cox proportional hazard regression model was adjusted for age, gender, race, ethnicity, duration of disease, body mass index (BMI) and disease-modifying treatment (DMT) use. These adjusting variables are known to possibly change risk of relapse. DMT use was categorised into four groups: (1) subjects on no DMT; (2) subjects receiving interferon beta, glatiramer acetate or teriflunomide; (3) subjects receiving dimethyl fumarate or fingolimod and (4) subjects on natalizumab, rituximab or alemtuzumab. Subjects who switched treatment during the follow-up period were counted in the treatment group with the longest follow-up time. The model was also further adjusted for baseline 25 (OH) vitamin D serum levels, which are associated with clinical and MRI markers of disease activity.14 Model checking, including testing and visual inspection for proportional hazard assumption, was performed. The assumption of proportionality was not violated in the Cox models. All statistical analyses were performed using R language and environment V.3.1.1.
Kaplan-Meier curves were used to depict energy intake from fat and vegetable consumption and time to the next relapse of MS.
Results
Patient characteristics
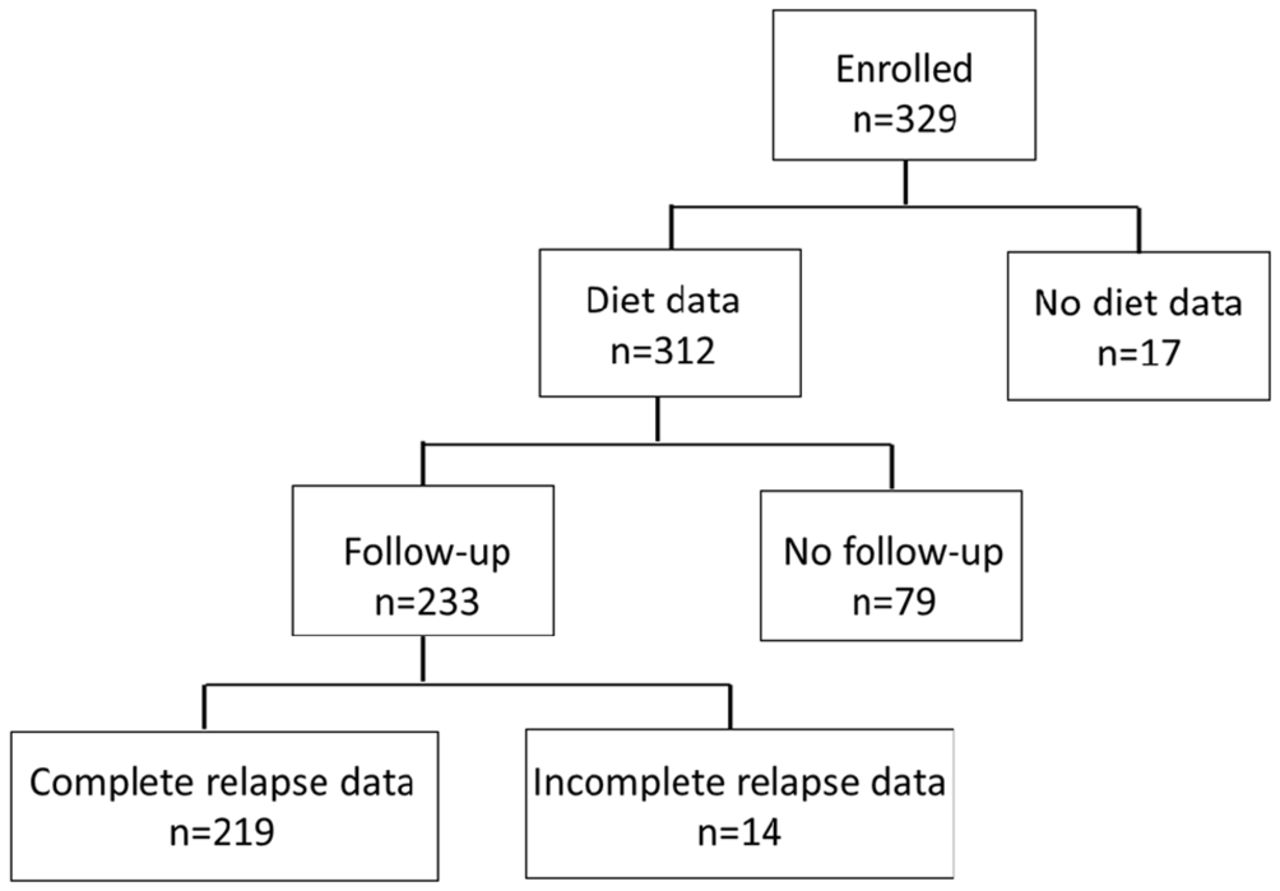
The number of paediatric MS cases with food frequency questionnaire and follow-up information was 219 (figure 1). Median duration of follow-up time after enrolment in the study was 1.8 years (range 0.1–4.1). Ninety-three (42.5%) patients experienced relapses during follow-up. Table 1 presents baseline characteristics.
Demographic characteristics (n=219)

Flow chart of study participants.
Diet and relapse association
Univariate and multivariate associations between various nutrients and risk of MS relapse are shown in table 2. In multivariable analyses, each 10% increase in energy intake from fat increased the hazard of relapse by 56% (adjusted HR: 1.56, 95% CI 1.05 to 2.31, p=0.027) adjusting for age, gender, race, ethnicity, duration of disease, BMI, total energy intake and use of DMT (table 2). When we added baseline 25(OH) vitamin D serum level to the above model, the adjusted HR remained at 1.58 (95% CI 1.06 to 2.36, p=0.026). Each 10% increase in saturated fat tripled the hazard of relapse (adjusted HR: 3.37, 95% CI 1.34 to 8.43, p=0.009). When we added baseline 25(OH) vitamin D serum level to the above model, the adjusted HR remained at 3.22 (95% CI 1.26 to 8.17, p=0.014). In contrast, each additional one cup equivalent in vegetable intake decreased the hazard of relapse by 50% (adjusted HR: 0.50, 95% CI 0.27 to 0.91, p=0.024). When we added baseline 25(OH) vitamin D serum level to the above model, the adjusted HR remained similar (HR: 0.53, 95% CI 0.28 to 0.98, p=0.043).
Various nutrients intake and MS relapse risk using univariate and multivariate Cox proportional hazard model
The associations reported for per cent calories from fat and vegetable intake were independent when combined in the same model. The HR for each additional 10% of energy intake from fat adjusting for age, gender, race, ethnicity, duration of disease, BMI, total energy intake from fat, use of DMT, total energy intake and vegetable intake was 1.48 (95% CI 0.99 to 2.19, p=0.05). The HR of relapse for each additional cup of vegetable intake while mutually adjusted for fat intake and other possible confounding factors was 0.53 (95% CI 0.29 to 0.98, p=0.04). Results did not change when socioeconomic status added to the model (data not shown). Total energy intake, fruits, fibres, carbohydrate, sugar, iron, cholesterol and dairy intake were not associated with risk of relapse (table 2).
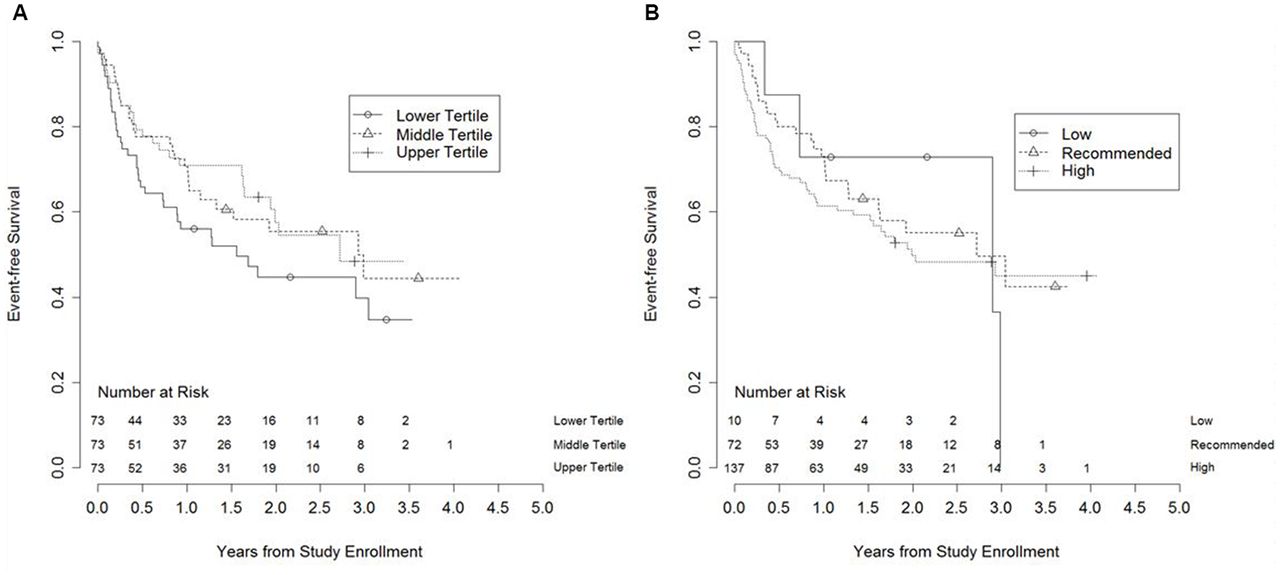
Figure 2A,B highlight respectively the increased risk of relapse in subjects with fat intake higher than recommended level for child’s age and in those with lowest tertile of vegetable intake.
{kind=link}
{kind=link}
Kaplan-Meier survival curves depicting time to the first relapse. (A) Among patients who had recommended (or low) per cent of energy intake from fat versus high energy intake from fat (low (<25%), recommended (25%–35%) and high (>35%)). (B) Among patients in different dietary vegetable intake tertiles (vegetable tertile cut-offs are 0.495 and 0.905 cup equivalent).
Discussion
We report a significant and independent association between dietary intake of fat and vegetables, with risk of relapse in early paediatric MS. Saturated fat intake was the main source of fat associated with risk of relapse when adjusting for total energy intake. Our data suggest a potentially protective influence of vegetable intake and harmful effect of fat intake on risk of relapse. While we have previously investigated the association between dietary sodium intake with MS susceptibility and relapse risk,15 16 no other study has prospectively investigated the association between nutrients and relapse risk in early paediatric MS.
High-fat diet upregulates the metabolism of cells, including the release or expression of proinflammatory molecules, contributing to low-grade systemic inflammation. It also results in dysbiotic gut microbiota and alters intestinal immunity.17–19 Moreover, the consumption of animal fat is often linked to high-calorie intake, which is itself a detrimental factor for many chronic inflammatory diseases.17 18 It has been shown that a high-fat diet results in immune cell infiltration and an increase in inflammatory mediator production in the CNS in an animal model of MS.5 Consumption of animal fat may be associated with MS prevalence.20 Saturated fat produces inflammatory response predominantly through activation of toll-like receptor 4.21 In addition, in a case–control study, high-energy and animal-based food intake were associated with a higher risk of MS,22 while higher intake of omega-3 polyunsaturated fatty acids was associated with a decreased risk of a first clinical diagnosis of CNS demyelination.23 More recently, no relationship between intake of total fat or major specific types of fat and the risk of MS was reported.24 While diet may also affect MS course, very few studies have focused on this. A small trial of low-fat diet intervention with omega-3 fatty acid supplementation suggested it may improve fatigue and relapse rate in patients with RRMS.25 In an observational study (ie, not blinded, not randomised), adult MS patients with consumption of ≤20 g of fat per day had a slower disability progression and lower mortality than those with higher intake after 34 years of follow-up.26 Several of these observational studies did not have prospective data collection, and all investigated the role of high-fat diet in adult but not in paediatric MS. Another recent randomised control trial in adults with RRMS with 1-year follow-up showed no significant improvement on relapse rate in the group with very low-fat diet.27
Cholesterol is an essential component of myelin membranes.28 Glial and neuronal membranes are composed of lipids, cholesterol and phospholipids.29 A few studies have suggested that cholesterol level and markers of cholesterol turnover in the peripheral blood may be associated with adverse clinical and MRI outcomes in MS,28 30–33 while another observational cohort study did not report any association with relapse risk.34 In our study including conservative adjustments for potential confounders, we have not detected any association between cholesterol intake and subsequent risk of relapse in children with MS; however, serum cholesterol level was not tested in our study.
In contrast to high-fat diet and saturated fat, vegetable intake downregulates the synthesis of proinflammatory molecules and restores or maintains a healthy symbiotic gut microbiota.35 Prior studies have shown conflicting results about the association of vegetable intake and MS development in adults.22 36 In an online brief survey of dietary habits in Australia, ‘healthy’ consumption of fruit and vegetables was associated with reduced self-reported MS relapse rate in the 12 months prior to survey and disability at the time of the survey.7 Our study confirms and expands findings from this report using a detailed validated dietary assessment and relapse data collected prospectively by participating neurologists after dietary assessment. Lower serum vitamin D3 levels is associated with a substantially increased subsequent relapse rate in paediatric-onset MS or CIS.4 To account for this association, we controlled for the confounding effect of vitamin D in multivariable models.
Despite reports that meals rich in refined carbohydrates and sugar increase insulin level and production of proinflammatory molecules and free radicals,37 our study findings did not support the association between sugar intake and relapse risk in paediatric MS. In addition, another nutrient of interest, iron, essential for normal neuronal functioning, has been proposed to contribute to MS pathogenesis, calling into question whether an MS patient’s diet should be adjusted to lower their dietary iron intake.38 39 A small study (n=9) using iron chelation for 2 years however did not support a disease-modifying effect of iron in established progressive MS.40 Our data do not show evidence for an association between iron intake and relapse risk in the paediatric MS population.
The strengths of our study include the size of the cohort (recruited across 11 US sites) with a diverse paediatric MS population in early stages of the disease with low disability scores, the evaluation of several dietary components using a validated questionnaire and careful case and relapse ascertainment collected prospectively in the paediatric MS Network database after enrolment. Analyses were carefully adjusted for possible confounding factors including known risk factors associated with relapse rate such as 25(OH) vitamin D levels.4 We acknowledge a few limitations. First, dietary data were only collected at baseline, and the food frequency questionnaire was a screener (BKFS) that may have overall underestimated caloric intake thus possibly overestimating the proportion coming from fat. Second, we cannot exclude the possibility that subjects changed their dietary habits after enrolment, which may have influenced subsequent relapse rate; however, there are no specific dietary recommendations for patients with MS. Confirmation of these results using prospective food diaries in the future might be helpful. Third, results could be attributable to other unmeasured but correlated nutrients, and therefore it is important to study in the future. Fourth, caloric consumption may have been underestimated in teenage age groups (specifically 18–19 years) due to increased alcohol and coffee intake, which are not assessed with the BKFS. Fifth, we do not report the effect of different polyunsaturated fatty acids such as alpha linolenic acid or omega-3 in this study. There are also other possible confounding factors that may not have been included in our models such as exposure to cigarette smoking. Finally, our study does not establish causality but only demonstrates an association.
In conclusion, we observed that fat intake is associated with an increase in the risk of relapse in paediatric MS, and saturated fat seems to drive this association, while vegetable intake may be independently protective. Further work confirming and refining any relationship between fat, vegetable and other nutrients and MS relapse is needed. Our results provide preliminary evidence for healthy dietary recommendation for paediatric patients with MS. These findings must be confirmed, and their causality must be established with future dietary intervention trials.
Acknowledgments
We would like to thank the parents and children who have participated to this study and the study coordinators who have tirelessly helped enroll and evaluate subjects.
References
Footnotes
Contributors SA helped on preparing the plan of analysis and first draft of the manuscript. EW designed the study, obtained funding, edited the plan of analysis and the first and subsequent drafts of the manuscript. She helped with case recruitment and interpretation of the findings. TS, JG, AW, TL, AB, BWG, GA, J-MT, JH, JN, YH, LK, MG, LB, MR, TC and SM enrolled cases and edited the manuscript. JR, SR and CTC provided support to coordinate the study, prepared plan of analysis, analysed data and edited the manuscript. LFB helped with design of the study. SLC helped with the interpretation and analyses of the data.
Funding The National Institutes of Health NS071463 (PI Waubant) and the National MS Society HC 0165 (PI Casper).
Competing interests Dr JG was supported by grants from Race to Erase MS, NMSS, Biogen and Genentech during this work. Dr AW is funded by the NIH (NINDS, K23NS069806) and has received research funding from Biogen Idec. Dr CTC has been supported by the National MS Society and the NIH (R01NS071463). He is an ad hoc consultant for Biovest International, Inc. Dr EW is funded by the National MS Society, the NIH and the Race to Erase MS. She volunteers on an advisory board for a clinical trial of Novartis. Dr LK is supported by the National MS Society, NIH, Robert and Lisa Lourie Foundation, Department of Defense. She has received honoraria, consulting payments, grant support or royalties from Biogen, Medimmune, Novartis, Teva Neuroscience, Sanofi-Aventis and EMD Serono. Dr BWG received honoraria for serving in advisory boards and educational programmes from Teva Pharmaceuticals, Biogen Idec, Novartis, Acorda EMD Serono, Novartis, Genzyme and Sanofi. She also received support for research activities from the National Institutes of Health, National Multiple Sclerosis Society, National Science Foundation, Department of Defense, EMD Serono, Biogen Idec, Teva Neuroscience, Novartis, Acorda, Genzyme and the Jog for the Jake Foundation. Dr TC has served as a consultant for Biogen Idec, Teva Neurosciences, Novartis and Sanofi-Aventis and has received grant support from NIH, National MS Society, Guthy-Jackson Charitable Foundation, CMSC and Merck-Serono, Novartis, and Biogen and Verily. Dr JR has research funding from Teva Neuroscience and Biogen. He is a member of the Medical Advisory Board for the DECIDE trial, which is funded by Biogen and AbbVie. Dr GA has received research support from Biogen-Idec. Drs AB, JN, MG, TL, MR and GA have no disclosures. JH has no disclosures. Dr J-MT received funding from the NIH (NCATS) during this work.
Provenance and peer review Not commissioned; externally peer reviewed.