Article Text

Abstract
OBJECTIVE A previous study of botulinum toxin type F (BTX-F) treatment for torticollis had shown a dose of 520 MU to be effective, but for a much shorter duration than is usual with botulinum toxin type A (BTX-A). The objective was to assess the effect of a higher dose of BTX-F.
METHODS Four of the previously treated patients, plus an additional patient, were treated with a higher dose of 780 MU BTX-F. All were secondary non-responders to BTX-A due to neutralising antibodies. A test injection of 40 MU BTX-F was also given into the extensor digitorum brevis muscle (EDB), to examine the time course of the biological effect of the toxin electrophysiologically. Patients were followed up at two, four, eight, and 12 weeks.
RESULTS All patients reported subjective improvement lasting from seven to 11 (mean 8.6) weeks accompanied by a significant reduction in mean clinical severity scores at two weeks. Four patients had pain which was substantially reduced. The electrophysiological studies confirmed biological sensitivity to the toxin in all patients, showing a significant change beginning at two weeks and returning to baseline at 12 weeks. The time course of this effect paralleled roughly that of the clinical response. The four patients who had previously received 520 MU BTX-F reported that the response was better and longer in duration with 780 MU. Dysphagia was more common than reported with the lower dose.
CONCLUSION Better results are possible with higher doses of BTX-F but the duration of benefit is still shorter than with BTX-A, seemingly due to a shorter duration of neuromuscular junction blockade.
- botulinum toxin F
- botulinum toxin A
- torticollis, resistance, EDB test
Statistics from Altmetric.com
Botulinum toxin F (BTX-F) may be an effective alternative treatment for patients with dystonia who have failed to respond to the more established serotype, botulinum toxin A (BTX-A). The use of BTX-F in patients clinically resistant to BTX-A has been investigated using a Japanese preparation of BTX-F,1-3 and recently by our group using a United Kingdom preparation (Speywood Pharmaceuticals).4 In that study, we reported the results of an open labelled trial treating both primary and secondary non-responders with BTX-F, using two doses—220 mouse units (MU) and 520 MU BTX-F. All our secondary non-responders showed improvement with the higher dose of this serotype. Unfortunately, the duration of clinical response seems substantially shorter than that usually found with BTX-A,1-5 an average of five weeks compared with 12 weeks for BTX-A.4 Animal experiments have shown a shorter duration of neuromuscular junction blockade with BTX-F,6which presumably underlies the shorter clinical response, but this has not yet been tested in humans. Furthermore, clinical experience with BTX-A has shown that a longer duration of benefit can sometimes be obtained with a higher dose, raising the question of the dose-response relation of BTX-F.
In an attempt to consider these questions, we have now treated our same group of patients with a higher dose of BTX-F, while at the same time examining the temporal course of the biological responses to BTX-F electrophysiologically with test injections of BTX-F to the extensor digitorum brevis muscle (EDB).
Patients and methods
Four of the patients from the original trial4 and an additional patient were included in this study. All five patients were secondary non-responders to BTX-A and the four original patients had all previously responded clinically to a dose of 520 mouse units (MU) BTX-F.
CLINICAL INVESTIGATION
Pretreatment clinical assessment and review at two, four, eight, and 12 weeks was performed by one of us (MKH) using the Tsui scale and Toronto western spasmodic torticollis rating scale (TWSTRS).7 The latter evaluates separately physical severity, functional disability, and pain. However, given the few patients, only the severity and pain scores were analysed for statistical reasons. Video recordings were made at the same time by an audiovisual technician using the TWSTRS videotape protocol.8 These tapes were later randomly arranged to be reviewed independently by two other examiners (AJL and GLS) who were blind to their chronological order. The examiners rated the videos for severity of torticollis using TWSTRS.
CLINICAL INJECTION PROTOCOL
Because we wanted to examine the response to a dose higher than the 520 MU previously given,4 we arbitrarily increased the dose by 260 MU, the amount contained in a single vial, to a total dose of 780 MU BTX-F. After assessment, each patient received 780 MU BTX-F divided among affected neck muscles using EMG guidance. The most often injected muscles were sternocleidomastoid, splenius capitus, and trapezius. The sternomastoids and splenii were injected at around the level of the mastoid process in single sites. Vials contained 260 MU each of the toxin and were diluted with normal saline (2.6 ml) to a concentration of 100 MU/ml.
ELECTROPHYSIOLGICAL TESTING
On the same day as the BTX-F injections were given to the neck, baseline compound muscle action potentials (CMAPs) were recorded from EDB bilaterally after supramaximal stimulation of the deep peroneal nerves at the ankle. Next, 40 MU BTX-F were injected into the left EDB with EMG guidance. To assess biological sensitivity and to follow biological response to BTX-F treatment, the CMAPs of both left and right EDBs were recorded at two, four, eight, and 12 weeks, using the right EDB as a control. The four patients who had participated in the earlier trial4 had received an injection of BTX-A into the left EDB with no biological response. The remaining patient (patient 2) had never received a test injection of either BTX serotype into EDB. The CMAP amplitude of the injected EDB was normalised by expressing it as a ratio of the amplitude of the non-injected side to minimise between trial variability resulting from temperature changes.9
STATISTICS
Serial clinical and electrophysiological data were analysed by repeated measures analysis of variance (ANOVA) using either univariate or multivariate tests as appropriate; significant results were analysed further with paired t tests. Comparisons with data from the previous study were made with a Wilcoxon signed rank test.
Results
Table 1 shows the clinical characteristics of the patients studied. There were three women and two men ranging in age from 27 to 63. All patients were secondary non-responders developing clinical resistance to BTX-A after receiving total doses ranging from 6200 to 12 300 MU (mean 9250 MU). Treatment with BTX-A had been administered on average every three months over a period ranging from 36 to 83 months (mean 59.5). The patients all tested positive for antibodies to BTX-A at intermediate to high titres using the mouse neutralisation assay (Speywood Pharmaceuticals).

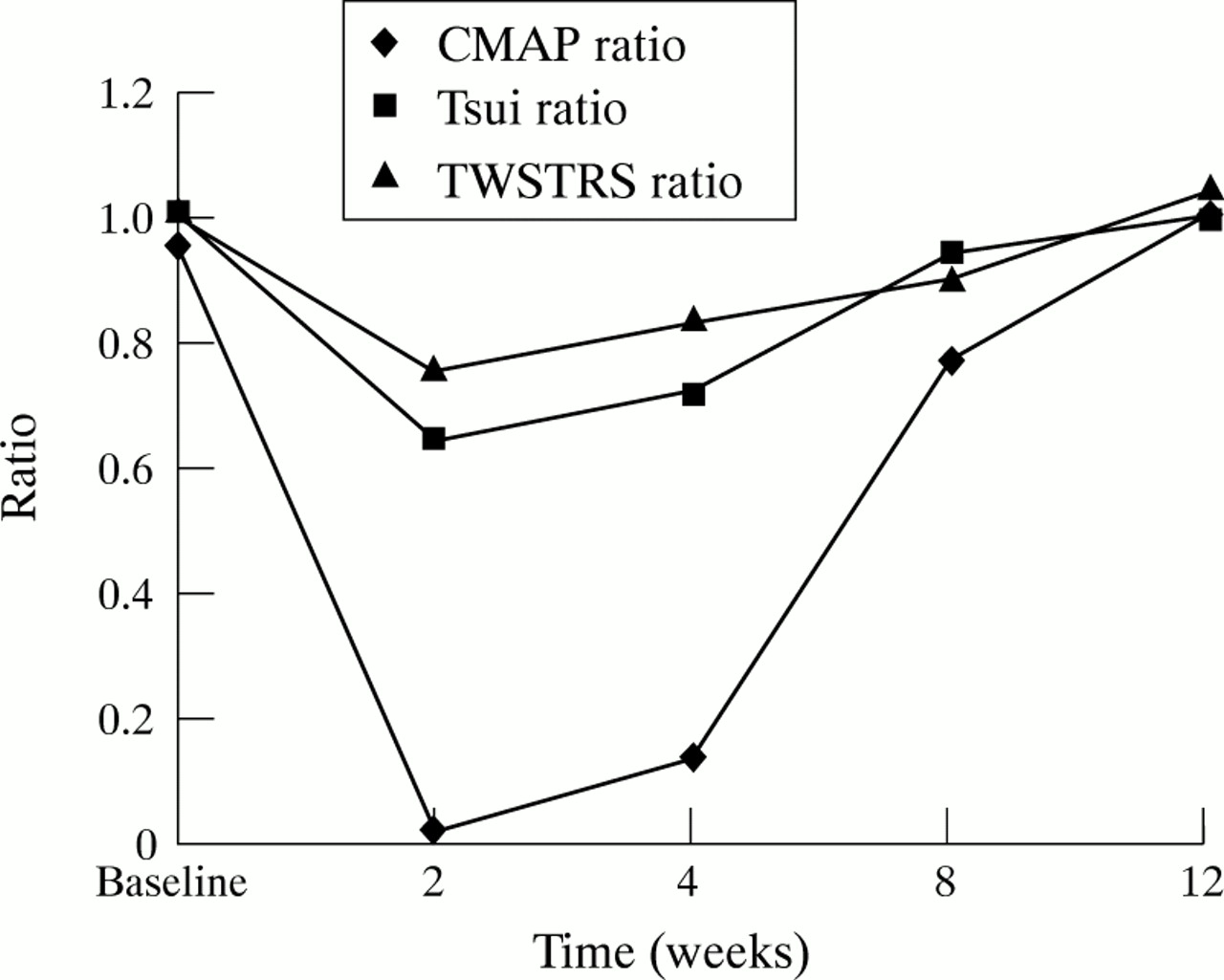{kind=link}
Comparison of the time course of the reduction in CMAP amplitude of the EDB muscle injected with BTX-F and the mean clinical (Tsui and TWSTRS severity) scores. All data are expressed as ratios of the baseline values for ease of comparison.
Clinical characteristics of patients
RESPONSE TO BTX-F INJECTIONS
After injection, all patients reported improvement of their torticollis, with an onset latency ranging from two to seven days (mean 4.5 days). Table 2 shows the Tsui and TWSTRS scores. Individual Tsui scores were reduced at two weeks in all patients, remained reduced at eight weeks in all but one patient, and by 12 weeks were back to baseline. The individual TWSTRS severity scores were likewise reduced in all patients at two weeks, but in progressively fewer patients thereafter, until only one remained reduced at 12 weeks. Repeated measures ANOVA showed a significant TIME effect for both Tsui and TWSTRS severity scores (p<0.01). Subsequent paired t test analysis disclosed that the only significant change in Tsui or TWSTRS severity scores was at two weeks (p<0.01 Tsui, p<0.02 TWSEV). The strength of this result is diminished because of the multiple comparisons. The four patients with significant pain at baseline reported improvement and TWSTRS pain scores also showed a significant change (ANOVA, p<0.05). The patients’ subjective duration of benefit ranged from five to 11 weeks, with a mean of nine weeks. Subjectively all patients had returned to baseline by 12 weeks, in agreement with their objective scores. Four patients experienced mild dysphagia and one patient had some minor pain at the injection site after treatment.
Individual clinical severity scores and electrophysiological results
The videotape assessments made by the blinded examiners generally agreed poorly with each other (correlation not examined statistically) and repeated measures ANOVA disclosed no significant changes in either Tsui or TWSTRS severity scores.
ELECTROPHYSIOLOGICAL RESULTS
Table 2 shows the electrophysiological data. The CMAP ratio (injected/non-injected amplitudes) fell substantially after injection in all patients (ANOVA TIME effect, p<0.0001). CMAP amplitudes were dramatically reduced at two weeks (p<0.001, paired ttest) and remained significantly reduced (even allowing for the effects of multiple comparisons) at eight weeks until returning to baseline at 12 weeks. Thus the biological response lasted between eight and 12 weeks and the average subjective duration of clinical benefit was around nine weeks. Figure 1 illustrates well that the changes in CMAP roughly parallelled the two clinical severity scores, particularly the Tsui scores.
COMPARISON WITH PREVIOUS STUDY OF 520 MU BTX-F
Table 3 shows that four patients had participated in an earlier trial of BTX-F4 and the clinical data after both doses of BTX-F; only Tsui scores were recorded in the earlier study. Injection of 520 MU of BTX-F in these four patients had resulted in a reduction of mean Tsui scores from 13.3 to 8.8 after two weeks, compared with a similar reduction from 12.8 to 8.8 in the present study (Wilcoxon, p>0.05). Despite the absence of a difference in the objective measures, all patients rated the response to the higher dose (780 MU) as better than that obtained from the lower dose (520 MU). The subjective duration of response ranged from four to six (mean 4.8) weeks after 520 MU, compared with seven to 11 (mean 9.5) weeks after 780 MU but this difference was not significant. Analysis of the duration of response based on the Tsui scores was not possible given the differing times of follow up after the two doses. Two patients experienced side effects in the earlier study, consisting of dry mouth in one (patient 4) and both mild dysphagia and dry mouth in the other (patient 1).
Data comparison between 520 MU and 780 MU BTX-F
Discussion
In this study, all patients showed subjective improvement in their torticollis after injection of 780 MU BTX-F, accompanied by a significant Tsui and TWSTRS score reduction at two weeks. 780 MU BTX-F was also effective in reducing the pain associated with torticollis. The lack of any significant change in Tsui or TWSTRS severity scores beyond two weeks despite continuing subjective benefit most probably reflects the small numbers; also the reputed lack of sensitivity of these measures has been emphasised.10
Of the four patients who had also been involved in the previous study using 520 MU BTX-F, three showed a greater reduction in their Tsui scores after the higher dose of 780 MU and all four reported a better response. Furthermore, the subjective duration of effect from the use of 780 MU was almost double that reported using 520 MU in most patients. However, neither of these differences were significant, possibly again reflecting the small numbers. There is only the suggestion that both the efficacy and duration of response might be improved using the higher dose. Whereas only one of the four patients developed dysphagia after injection of 520 MU BTX-F, three reported dysphagia using 780 MU, albeit mild in severity. The price of a longer duration of benefit using higher doses may therefore be a greater risk of dysphagia.
Biological sensitivity to BTX-F was established by electrophysiological testing, which showed a dramatic reduction in the CMAP amplitude of the injected test muscle (EDB) in all patients. The time course of the biological response (CMAP reduction) followed roughly that of the objective clinical scores. The CMAP amplitude had recovered fully by 12 weeks but in a similar experiment involving a roughly comparable dose (10 MU) of a BOTOX®preparation of BTX-A, the CMAP amplitude of the EDB muscle was still reduced by a mean of 40% after 100 days.11 These results are consistent with animal experiments showing that BTX-F has a shorter duration of neuromuscular junction blockade than BTX-A6 and this property seems to adequately explain the relatively short duration of clinical benefit from BTX-F. The basis of this difference may lie in the different substrates of the two BTX types in the nerve terminal. Interestingly, whereas there seemed to be a close association between clinical response and neuromuscular junction blockade from BTX-F in the present report, the study involving BTX-A suggested that neuromuscular junction blockade would well outlast the clinical response.11
In conclusion, these results suggest that a higher dose of 780 MU BTX-F may produce a subjectively better and longer duration of benefit than a dose of 520 MU. However, it is still substantially shorter than the average duration of benefit obtained from BTX-A, seemingly because of a shorter duration of neuromuscular junction blockade. The optimal dose of BTX-F for an individual patient should be determined by the practitioner, but this study suggests that dysphagia could be a potential problem with doses of BTX-F exceeding 780 MU. Thus, although not as practical as BTX-A, BTX-F can still provide some measure of symptomatic relief for those who have become immune to BTX-A. The question of immunity to BTX-F developing after long term treatment is still unknown. Larger series using higher doses of BTX-F and studies evaluating higher and more frequent dosing with regard to antibody development are needed.