Article Text

Abstract
The effect of hemianopia on line bisection is not known. To study this, manual line bisection in 30 patients with unilateral cerebral hemispheric lesions was examined. The mean bisection point in a group of eight patients with left hemineglect was biased rightward (ipsilaterally), as expected. Among the remaining 22 patients, eight had right hemianopic visual defects, eight had left hemianopic visual defects, and six had normal visual fields. Both groups of patients with contralateral visual field defects had mean bisection points biased contralaterally, compared with 68 normal subjects. This bias was less than the ipsilateral (opposite) bias of patients with hemineglect. Contralateral bisection bias was more evident in those whose field defect involved the macular region. No bias was seen in patients with neither field defects nor hemineglect. The contralateral bias in hemianopia may represent either non-veridical spatial representation within a visual hemifield or a consequence of the strategic adaptation of attention into contralateral hemispace after hemianopia.
- line bisection
- hemianopia
- neglect
- attention
Statistics from Altmetric.com
Line bisection is used to diagnose hemineglect after unilateral cerebral lesions.1 2 Patients with hemineglect place their bisection marks in the hemispace ipsilateral to their lesion,3 4 whereas bisection is more accurate in normal subjects5 6 and patients with hemispheric damage but no other signs of hemineglect.2
One variable that has received little attention is the presence of visual field defects. Most studies combine patients with normal and hemianopic fields as controls.7 However, there are grounds to think that such visual defects may alter line bisection. With complete hemianopia, the line is perceived in only one hemifield. Spatial representation within a hemifield may not be veridical: Reuter-Lorenz et al 8 found that normal subjects skewed bisection of lines in the right hemifield rightward, and leftward in the left hemifield. On the other hand, the ocular search of hemianopic patients displays a gradient weighted towards contralateral space9: this likely reflects a strategic adaptation of attention favouring their blind side, and a contralateral bisection bias may be one consequence.
In a study of ocular search during line bisection in hemineglect and hemianopia,10 we found that hemianopic patients did display a contralateral bisection bias. Also, their eye movements had a central peak of fixation activity that was biased into contralateral hemispace, whereas normal subjects bisected and fixated at the true line centre. To corroborate this unexpected finding, we reviewed data from 30 patients who had performed line bisection as part of a neglect battery administered during other studies.11 12
Methods
We examined 30 patients with unilateral cerebral hemispheric lesions on CT or MRI. All patients gave informed consent. Patients with optic neuropathy, glaucoma, and comprehension problems were excluded. All had corrected visual acuity of 20/40 or better. Visual fields were assessed by Humphrey 30–2 perimetry. Field defects were classified as quadrantic, incomplete hemianopia, and complete hemianopia.
The neglect battery13 was administered under standard lighting conditions. It contained clock and flower copying and drawing tasks,14 a line cancellation task,15 four line bisection tasks, and a figure cancellation task,16given in that order. The line bisection component consisted of two lines of 15 cm length on one sheet of paper, 16 cm apart, and two of 20 cm length on another, 14 cm apart. All lines were 0.5 mm thick and had 2 cm long vertical lines marking the line ends. Unlike our prior study, viewing distance was not standardised: for approximate comparison, the lines subtend 22 and 29° of visual angle at viewing distances of about 40 cm. The examiner sat on the patient’s right and centred each sheet to the patient’s body axis. All patients used their right hands. Eye and head movements were not restricted. Results were expressed as the % of line length deviated from centre, with rightward deviation positive.
The entire battery gave a score out of 100. A score greater than 6 indicated neglect: this was found in eight patients with right hemispheric lesions (RHDneg). Of the remaining 22 patients, five patients had right hemispheric lesions and normal visual fields (RHDnf), eight had right hemispheric lesions and hemifield defects (RHDhh), one had a left hemispheric lesion and normal visual fields (LHDnf), and eight had left hemispheric lesions and hemifield defects (LHDhh). There were no significant differences in ages. For controls we had 68 normal subjects spanning ages 17 to 77.
Differences between controls and the groups without hemineglect (excluding LHDnf) were tested by analysis of variance (ANOVA). We did not include patients with hemineglect because they are expected to have abnormal bisection, and would inflate the significance of the analysis. We then used pairwise comparisons to test for differences between patient groups and normal controls. Also, individual patients were classified as abnormal with reference to 95% prediction intervals from the 68 controls.
Group bisection results

{kind=link}
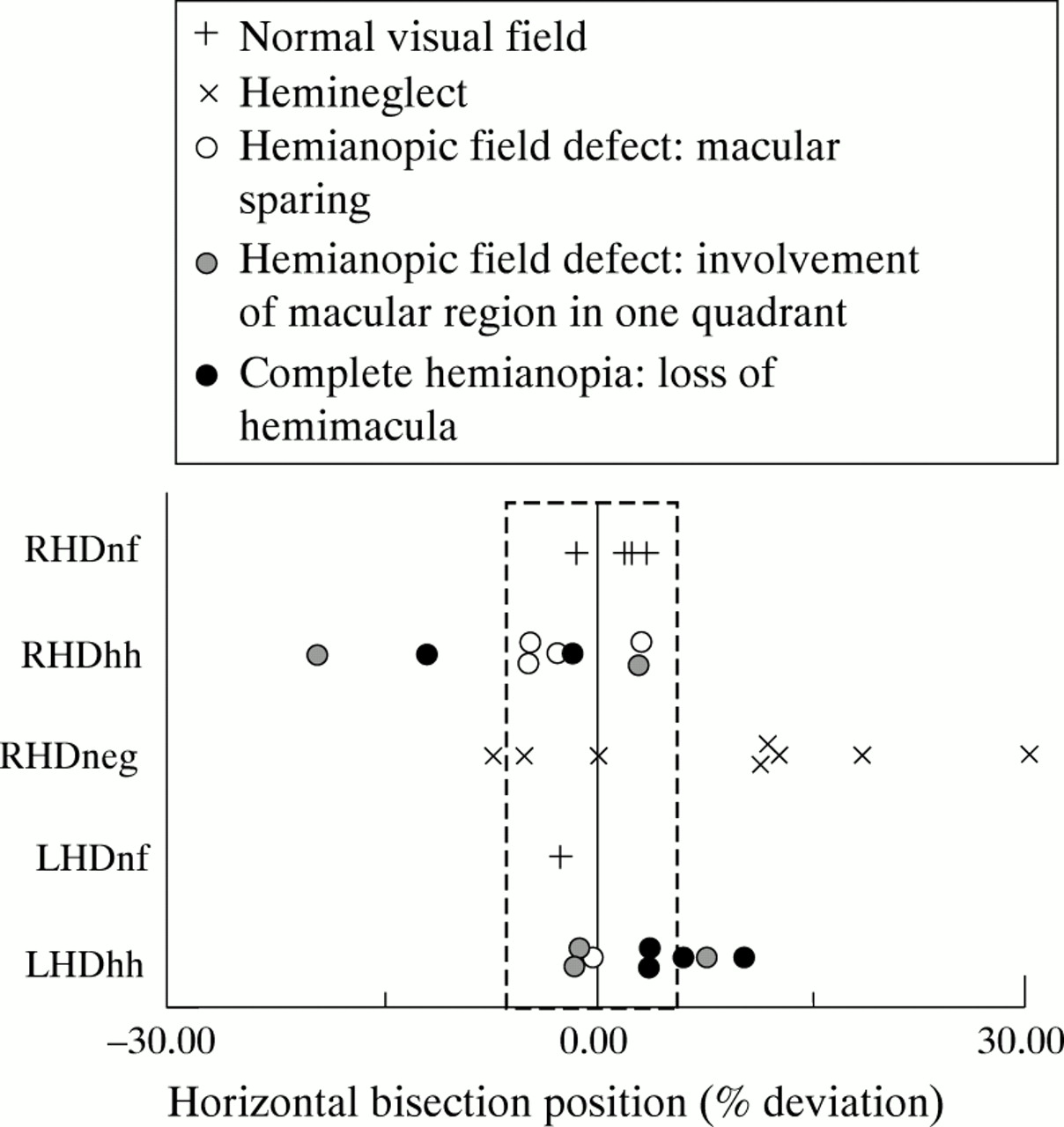
Line bisection by individual patients. Bisection is measured as % of total line length, rather than cm. Each result is the average of four bisections. The vertical dotted lines mark the borders of the 95% prediction interval derived from normal subjects; individual results to the left or right of this area are considered abnormal. Upright crosses represent those with normal visual fields, diagonal crosses those with hemineglect. Round symbols represent those with hemianopic field defects: clear circles are those with macular sparing, grey discs are those with involvement of the macular region in one quadrant, and black discs are those with complete hemianopia and loss of the hemimacula.
Results
Controls bisected lines very accurately (table). As expected, the hemineglect group deviated bisection rightwards, although a few patients showed normal or even slight leftward bias, confirming previous observations that bisection does not correlate perfectly with other hemineglect tests (figure).2 ANOVA showed a significant difference between non-neglect patients and controls (F(3,85)=7.85, p<0.0001). Pairwise comparisons showed that both groups of patients with hemifield defects were different from controls (p<0.004 for both hemianopic groups), with both deviating contralaterally. Five of the 16 patients with hemifield defects fell beyond the normal range contralaterally, none ipsilaterally. As a whole, this contralateral deviation was much less than the ipsilateral bias of hemineglect.
By contrast, there was no difference between controls and patients with normal visual fields. No patient with normal visual fields fell outside the normal range.
Contralateral bisection deviation tended to be larger in patients with larger visual field defects (figure). In particular, the six patients with complete macular splitting hemianopia had mean contralateral bisection errors of 6.15% (SD 4.07), whereas the six with sparing of both upper and lower macular regions had mean errors of 1.90% (SD 3.47) (p<0.05). However, these sample numbers and differences are too small to permit conclusions about the quantitative relation of the visual defect to bisection bias.
Discussion
Our prior report10 indicated that hemianopic patients had a contralateral bias to line bisection and the central peak of eye fixation in the ocular scanning preceding bisection. This was found with head fixed conditions, large displays subtending 37° and 45° at a distance of 1.14 m, and the use of a pointer, in seven hemianopic patients. However, that study did not examine patients with lesions and normal visual fields, so the bias may have been a non-specific effect of lateralised brain damage.
This study confirms contralateral bisection bias in a larger sample of 16 hemianopic patients. The bias also occurs under the more “natural” conditions used in neglect studies, with head movements permitted and the use of a pen at a writing table, and for lines subtending smaller visual angles. Also, the effect is not found in patients with hemispheric lesions and normal visual fields. Thus it is a consequence of hemianopia rather than cerebral damage. A possible correlation of contralateral bias with the severity of hemianopia and macular involvement would further support the hypothesis that the visual defect is causative. As most patients with hemineglect have hemianopia, this makes their ipsilateral biases all the more abnormal.
A contralateral hemianopic bias conflicts with predictions from Reuter-Lorenz et al.8 In that study normal subjects shown lines in one hemifield estimated midpoint to be more lateral than its true position. As patients with complete left hemianopia can only view the lines in their right hemifield, this would predict a rightward bisection bias, whereas in fact they biased bisection leftward (contralateral to their lesion). This discrepancy may originate from technical differences between the two studies. They used tachistoscopic presentations of under one second, whereas our patients had unlimited viewing time. They required subjects to judge the position of a mark on the line, whereas our patients made the mark. Perhaps most importantly, they used 2 cm lines, whereas our two studies employed lines an order of magnitude longer. Because the size and even direction of bisection bias in hemineglect depends on line length,3 4 17 biases in other subjects may also vary with this index. Finally, results from normal hemifields may not extrapolate to the intact hemifields of hemianopic patients, as there is accumulating evidence of various alterations in the remaining hemifield in hemianopia.18-21
Why might such a contralateral bisection bias arise in hemianopia? Any visual percept represents not only the physical properties of the stimulus but also the influence of numerous internal factors, including prior visual experience, expectation, and attention, among others. One internal factor that could generate an abnormal bias is a change in attentional distribution. During scanning of a letter array, normal subjects distribute fixations evenly across the display, suggesting a flat distribution of attention in this task.9 Hemianopic patients show a gradient of fixations with increased search in the contralateral hemisphere.9 A similar gradient of eye fixations is seen with line bisection, where hemianopic patients tend to search for the end of the line in their blind hemispace.10 22 23 We hypothesise that, because these patients are aware of their deficit, space on their blind side acquires greater salience, leading to an attentional gradient that is strategically adaptive for their disability. Whether the altered gradient is pathological (in neglect) or adaptive (in hemianopia), the result may be a bias in perceptual judgment in the direction of the gradient, causing ipsilateral bisection bias in hemineglect and contralateral bisection bias in hemianopia.
An alternative explanation is that the hemifield representation of space is not veridical. There is little data and the study of Reuter-Lorenz et al 8 did not examine the peripheral regions where our lines lay. Bowers and Heilman24 found that tactile bisection in one hemispace is biased contralaterally. Whereas this accords with our results, it is not known whether similar bisection errors occur visually. Also, our results are not explained by tangent artifact, as the lines were centred in front of the subjects, and hence the tangent points coincided with the midposition of the lines. Further studies are required to determine whether this contralateral bias is a manifestation of non-veridical spatial representation in hemifields or of an adaptive attentional gradient consequent to hemianopia.
Acknowledgments
We thank M Behrmann and C Szekely for assistance with data collection. JB was supported by MRC 9004FER-1222–21813 and NINDS NS01920–01A1.