Article Text

Abstract
Two siblings with myotonic dystrophy presented for treatment of faecal incontinence. The pathophysiology of this functional disorder is described with the results of anorectal manometry, EMG, and biopsy of smooth and striated muscle of the anorectal sphincters. Both medical and surgical management of the incontinence was unsatisfactory in the long term. Involvement of gastrointestinal musculature is a characteristic feature the disease.
- myotonic dystrophy
- gastrointestinal musculature
- faecal incontinence
Statistics from Altmetric.com
Myotonic dystrophy predominantly affects striated muscle, but multisystem involvement is well recognised.1 Abnormalities of smooth muscle lead to disordered oesophageal and gastrointestinal motility with megaoesophagus and megacolon and, rarely, incontinence.1-5 We describe the pathophysiology and management of major faecal incontinence in two siblings with severe myotonic dystrophy.
Anorectal physiology results
Clinical data
CASE 1
A 29 year old man developed increasingly severe faecal incontinence over the course of eight years. In the two years before investigation he had soiled his underclothes daily and had been unable to control either flatus or loose stool. In addition there was a long history of severe constipation. Incontinence of urine developed during coughing, and the urinary stream was poor.
Myotonic dystrophy was diagnosed at the age of 22 years. There was a myotonic grip, myopathic facies, frontal balding, wasting of the small hand muscles, and early cataracts. His father and three of five siblings were also affected. The diagnosis was confirmed by EMG and by genetic testing.
Digital and manometric anorectal examination showed poor resting tone and low squeeze pressures in the anal canal, without asymmetry. The rectosphincteric reflex was sluggish. Formal assessment of sensory thresholds to rectal filling and distension were within normal limits, although the rectal compliance was reduced (table). Defaecography showed faecal incontinence with an intrarectal intussusception. He declined urological investigation.
Electrophysiological studies showed normal pudendal nerve terminal motor latencies6 and a normal single fibre EMG fibre density in the external anal sphincter (table). No myotonic discharges were found in this muscle, but external urethral sphincter EMG showed profuse myotonic discharges, with reduced numbers of motor units. Motor units were recruited normally during coughing. There were no bizarre high frequency discharges.
For two years after a postanal sphincter repair faecal continence was restored. Postoperative anorectal and anal canal manometry showed an improved resting anal pressure compared with the preoperative study, but there was no change in the squeeze anal pressure, or in the anal canal length. Subsequently a minor degree of incontinence returned, which gradually increased during five years of follow up, leading again to socially distressing incontinence and a decision to treat with a permanent colostomy.
CASE 2
The 28 year old nulliparous sister of case 1 presented with a five year history of faecal incontinence and a minor degree of stress urinary incontinence. Examination disclosed the typical features of myotonic dystrophy.
The anus was patulous, with low resting tone. The external anal sphincter (table) was weak, with reduced resting and squeeze anal pressures. The internal anal sphincter relaxed normally on rectal distension, but cessation of this stimulus was followed by a rebound rise in anal canal pressure. Rectal sensation was normal. The pudendal nerve terminal motor latencies were normal. Anal EMG was refused.
During the first six months after postanal sphincter repair she experienced only one minor episode of faecal incontinence, but during the subsequent two years faecal incontinence recurred. Postoperatively the resting anal canal pressure was improved, but there was no change in squeeze anal canal pressure or in anal canal length. Urinary incontinence was not modified by anal surgery.
Histological findings
With preoperative consent of each patient, biopsies were taken from the external anal sphincter and puborectalis muscles during postanal repair. Frozen sections were prepared for light microscopy using standard enzyme histochemical methods. Material from these muscles was also studied by electron microscopy.
In case 1 the external anal sphincter biopsy (fig 1) consisted almost entirely of smooth muscle derived from the internal anal sphincter muscle. The external anal sphincter muscle was atrophic and difficult to identify. The tissue was abnormal, with pronounced fibrosis and abnormal variation in diameter of the remaining striated external anal sphincter muscle fibres. Zones of the tissue consisted only of fibrous scar tissue. The bundles of smooth muscle fibres were abnormally widely separated by this matrix of fibrous connective tissue. Some smooth muscle cells showed features consistent with dedifferentiation into myofibroblasts. No nerve fibres were seen. The anal sphincter of case 2 showed similar abnormalities, with few remaining striated muscle fibres.

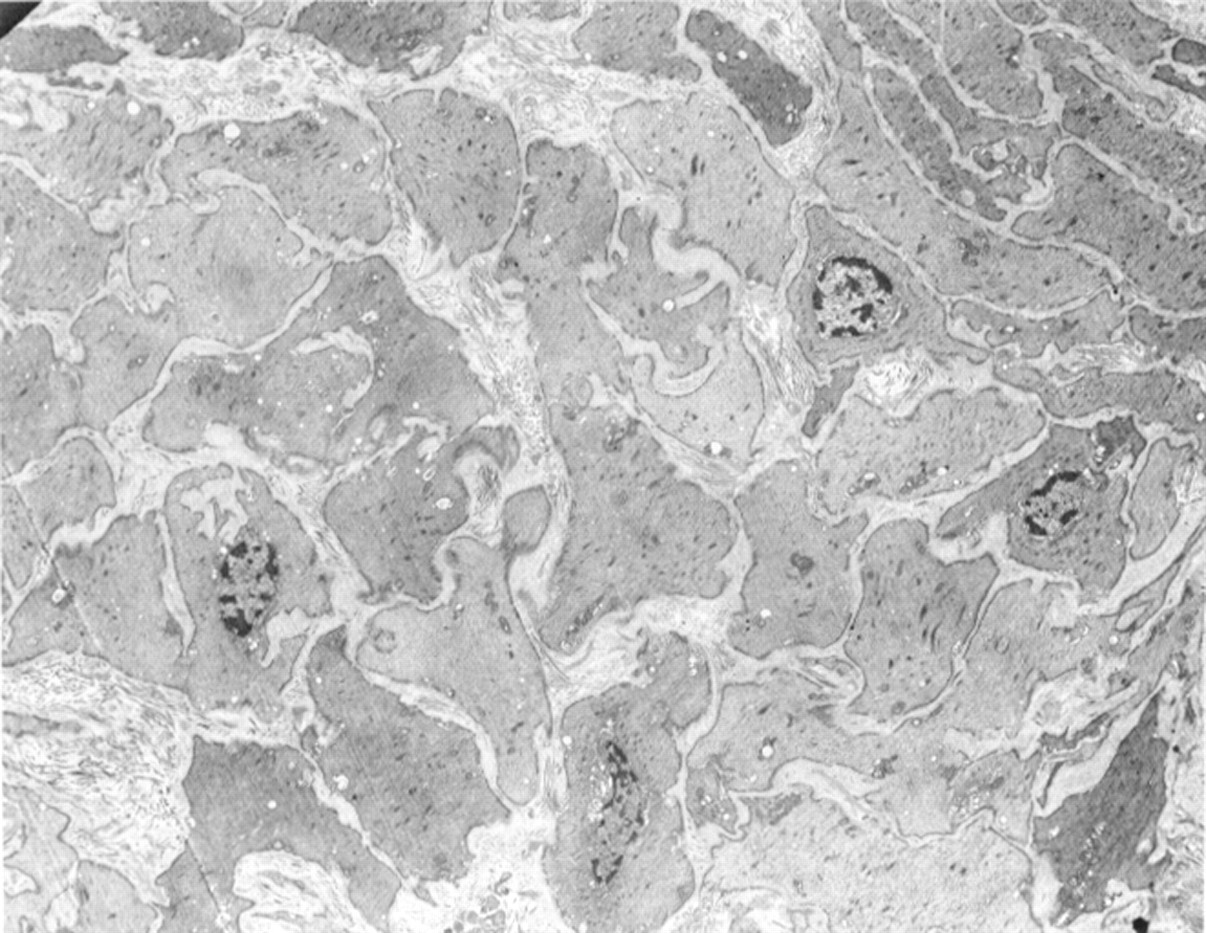
Electron microscopy ×3000. Myotonic dystrophy. The biopsy consisted almost entirely of internal anal sphincter. The smooth muscle cells are separated from each other by fibrous connective tissue, and vary in size and relative electron density. Stretched elastic tissue strands are seen between adjacent smooth muscle cells, indicating the disruption that has occurred in the tissue.
In both patients the puborectalis muscle biopsies showed some increased fibrosis and loss of striated muscle fibres. Many of the remaining muscle fibres were hypertrophic and there was increased central nucleation. Several fibres showed sarcoplasmic masses, but there were no necrotic or regenerating fibres. There was pronounced type 1 fibre predominance (99%). Type 1 fibres ranged from 28–120 μm in diameter (mean 64 (SD 22) μm). The normal puborectalis muscle (fig 2) shows 77% type 1 predominance, and the mean muscle fibre diameters are 26 (SD 11.2) μm in females and 34 (SD 14) μm in males.7
{kind=link}
{kind=link}
Electron microscopy×3500. Control specimen of internal anal sphincter from subject aged 30 years.8 The smooth muscle cells are arranged in close interdigitated juxtaposition, and there is little fibrous connective tissue in the biopsy.
Discussion
Widespread abnormalities of gastrointestinal motility have been described in myotonic dystrophy,1 8-11 involving the oesophagus and small and large intestine, but their pathogenesis is controversial. In one patient with megacolon associated with myotonic dystrophy Yoshida et al 9 described normal smooth muscle cells by light and electron microscopy, with loss of substance P and enkephalin containing colonic neurons. Conversely, Pruzanski and Huvos11 found histological evidence of degeneration and fatty infiltration of small intestinal smooth muscle in postmortem specimens from two patients. Our findings illustrate degeneration of smooth muscle cells and fibrosis in the internal anal sphincter, and loss of striated muscle fibres in the external anal sphincter and puborectalis muscles. The EMG confirms involvement of the striated external anal sphincter muscle with myotonia and myopathic features.
Anal sphincter function in myotonic dystrophy has been investigated only infrequently. Ekhardt and Nix4 found decreased resting and squeeze anal canal pressures in a group of 16 patients with myotonic dystrophy compared with a group of normal control subjects. The rectosphincteric reflex was abnormal in the patients with myotonic dystrophy; the normal response of internal anal sphincter relaxation to rectal distention was obscured by a prolonged myotonic contraction of the striated sphincter mechanism, as occurred in our case 2. Hamel-Royet al 5 found that the amplitude of this myotonic response to rectal relaxation was diminished by pudendal nerve blockade, suggesting that it was, at least in part, a neural reflex response. These manometric data suggest that both the striated external anal sphincter and the non-striated internal sphincter musculature are abnormal in myotonic dystrophy, and are consistent with our data (table). Eckhardt and Nix4 found myopathic potentials, with myotonia, as we did also, in EMG studies of the external anal sphincter. Pudendal nerve terminal motor latencies were normal in our patients, as was anorectal sensation, confirming the absence of a neurogenic lesion.6 The combination of smooth and striated muscle abnormality found in this disease by clinical examination, anorectal manometry, and histological studies is unique among the muscular dystrophies.
Postanal repair12 initially improved the functional disorder, but unfortunately this effect was not sustained. Our experience suggests that faecal incontinence in myotonic dystrophy is difficult to relieve by any currently available treatment other than colostomy.