Article Text

Abstract
OBJECTIVE To quantitatively assess control of balance under static and dynamic conditions in patients with tonic and phasic cervical dystonia.
METHODS Ten patients with purely tonic cervical dystonia with fixed postural deviation and 20 patients with cervical dystonia with phasic head movements were investigated at least 3 months after botulinum toxin injections. Seventeen age matched volunteers served as controls. Static posturography was performed on a force platform; dynamic equilibrium was studied on a stabilometer, which requires the subject to continuously adapt upright posture to an unstable tilting surface. Measurements of maximum amplitude and linear displacement of the pivot were taken with open and closed eyes.
RESULTS Sway path values in static posturography were not significantly different between patients with cervical dystonia and controls. On dynamic posturography, patients with phasic cervical dystonia showed significantly higher platform measures (maximum amplitude and linear displacement of the pivot) with eyes open and closed By contrast, none of the dynamic platform measures differed significantly between patients with tonic cervical dystonia and controls.
CONCLUSIONS Normal measures of dynamic equilibrium in tonic cervical dystonia argue against a primary abnormality of balance control in cervical dystonia. Impaired dynamic equilibrium in phasic cervical dystonia is likely to reflect a disruption of vestibular input due to repetitive, involuntary head oscillations.
- cervical dystonia
- posturography
- balance control
Statistics from Altmetric.com
In cervical dystonia some previous studies have described changes in vestibular function and perception of body orientation, such as asymmetries of the vestibulo-ocular reflex,1 2 vestibular hyperreactivity,3 subtle difficulties in recognising the postural and visual vertical,4 5 and abnormal postural responses to vibration of neck muscles.6 The clinical importance of these findings is still unclear. Dizziness or vertigo have not been reported in patients with cervical dystonia7and postural sway during quiet stance does not seem to be significantly impaired.6 Because sway tends to be small when subjects stand on a stable platform,8 these reports raise the question of how patients with cervical dystonia perform on a more sensitive dynamic device where vestibular inputs seem to play a major part in compensation for angular tilting pertubations of the support surface.9 In addition, previous reports have shown dynamic posturography to be influenced by vestibular, somatosensory, or visual input.8 10 Such findings raise the possibility that the type of abnormal movement in cervical dystonia (tonicv phasic) might influence postural control differentially by the different degree of vestibular stimulation in both diseases. To further consider these issues, we have quantitatively assessed postural sway under static and dynamic conditions in patients with tonic and phasic cervical dystonia. Dynamic equilibrium was studied on a stabilometer, which requires the subject to continuously adapt upright posture to an unstable tilting surface.
Patients and methods
Thirty patients with cervical dystonia (15 women, mean age 53.2 (SD 11.0 years) (range 28–70), mean disease duration 10.3 (SD 5.7 years) (range 2–26), mean height 168.6 (SD 9.7) cm (range 153–190)) were investigated in the order of admission to the Innsbruck outpatient movement disorder clinic. Twenty seven patients (90%) had isolated cervical dystonia, three had craniocervical dystonia (cervical dystonia plus Meige syndrome (n=2), cervical dystonia plus spasmodic dysphonia (n=1)). Except for dystonia these patients were neurologically normal. Seventeen healthy age matched volunteers (mean age 52.3 (SD 14.0 years) (range 28–74), mean height 170.1 (SD 9.7 cm) (range 154–189)) served as controls.
A thorough clinical examination was performed to exclude peripheral or additional disturbances of the CNS. Patients or controls with a history of vertigo or falls, current neuroleptic or sedative medication, hip or knee problems, diabetes, or severely impaired vision were excluded. Four patients (13%) were on low dose anticholinergic treatment (2.5–10 mg/day Artane®). All 30 patients were on botulinum toxin A treatment and investigated at least 3 months after previous injections.
Before posturography the severity of cervical dystonia was rated according to the Tsui scale11 with a median value of 9.8.5-17 Ten patients (33%) had purely tonic cervical dystonia with fixed postural deviation and no clinical evident head tremor or jerks. Twenty patients (67%) had unsustained (phasic) head movements which were either purely horizontal (n=12), or of a mixed type with horizontal (n=7) or vertical (n=1) preponderance.
STATIC POSTUROGRAPHY
Static posturography was performed on a force platform (Dynatronic Instruments, France). Measurements of displacement of the centre of foot pressure (sway path) were taken for 51 seconds with feet placed at an angle of 30 degrees, heels 2 cm apart in a standardised visual environment. Measurements were first taken with eyes closed and then with eyes open.
DYNAMIC POSTUROGRAPHY
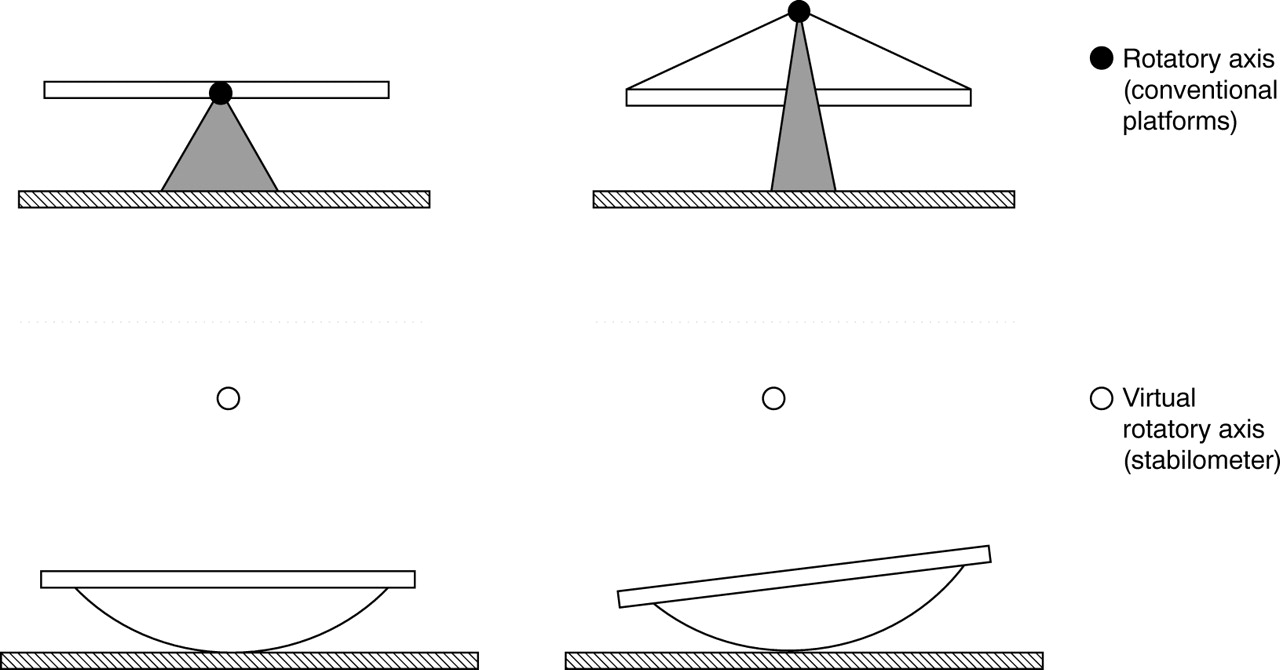
Dynamic posturography was studied with the subject standing on a stabilometer.12 The stabilometer is a seesaw consisting of a platform with a cylindrical curved base (radius 55 cm, height when level 6 cm). It comes into contact with the smooth surface of the ground along a generatrix of the cylinder (pivot). By contrast with other dynamic posturographic techniques, based on rotations around the axis formed by the subject's ankles (figure), the virtual axis of the stabilometer is located outside the support surface and continuously changes with platform movements. The design of the stabilometer makes the subject unable to stand still, needing to continuously adapt posture to keep balance. Tilts of the platform are continuously monitored by means of two potentiometers. Dynamic balance performance was assessed in patients and controls by (1) the linear displacement of the pivot (pivot length)—that is, the sum in mm of the absolute values of each elementary linear displacement of the pivot during the test—and (2) the maximum amplitude of pivot displacement in degrees. In the first trial subjects were required to stand (a) in the frontal position with eyes open, then (b) with eyes closed to measure anterior-posterior (a-p) displacement. In a second trial subjects were placed (c) in the lateral position with eyes open and (d) with eyes closed to assess lateral displacement. These four tests lasted 30 seconds each and were performed in the same order and with the same foot position (centred, 10 cm heel to heel distance, 30 degree foot a-p angle) in all subjects.
{kind=link}
The stabilometer consists of a platform with a cylindrical curved base. By contrast with other dynamic posturographic techniques, based on rotations around the axis formed by the subject‘s ankles, the virtual axis of the stabilometer is located outside the support surface and continuously changes with platform movements. The design of the stabilometer makes the subject unable to stand still, needing to continuously adapt posture to keep balance.
STATISTICAL ANALYSIS
In all tests, the null hypothesis was rejected at a significance level of p<0.05. Parametric data are expressed as mean (SD). Platform parameters are expressed as median values throughout the text and were analysed among groups (controls, tonic cervical dystonia, and phasic cervical dystonia) by Kruskal-Wallis analysis of variance (ANOVA) on ranks, and between groups by Mann-Whitney rank sumU test.
Results
STATIC POSTUROGRAPHY
Median sway path values with eyes open showed no significant differences among patients with tonic (248 mm) or phasic (334 mm) cervical dystonia and healthy controls (301 mm). With eyes closed the median sway path increased in all groups without signficant among group differences (506 mm, 612 mm, and 603 mm, respectively).
DYNAMIC POSTUROGRAPHY
Comparisons among controls, patients with tonic cervical dystonia, and those with phasic cervical dystonia showed significant differences for all lateral test positions—that is, for maximum amplitude (p=0.01) and linear displacement (p=0.005) of the pivot in the lateral test position with eyes open, and for maximum amplitude (p=0.02) and linear displacement (p=0.03) of the pivot in the lateral test position with eyes closed. Anterior-posterior parameters were less affected; significant among group differences were only found for a-p pivot displacement with eyes closed (p=0.03).
Median values of dynamic posturography in normal subjects and patients with tonic and phasic cervical dystomia (CD)
Tonic cervical dystonia (n=10)
Post hoc testing showed no significant differences between controls and patients with tonic cervical dystonia for any of the stabilometric recordings.
Phasic cervical dystonia (n=20)
Post hoc testing between controls (n=17) and patients with phasic cervical dystonia (n=20) showed significantly higher measures for all lateral test positions (table)—that is, for maximum amplitude with eyes open and closed (p=0.003 and p=0.008, respectively)—and for linear displacement of the pivot with eyes open and closed (p=0.002 and p=0.008, respectively). Patients with phasic cervical dystonia also showed significantly higher a-p pivot displacement with eyes closed compared with controls (p=0.02).
Patients with phasic cervical dystonia showed significantly higher measures compared with patients with tonic cervical dystonia in four of these five platform parameters: (1) lateral pivot displacement with eyes open (p=0.03), (2) lateral maximum amplitude (p=0.03), and (3) lateral pivot displacement (p=0.007) with eyes closed, and (4) a-p pivot displacement with eyes closed (p=0.04).
A further subgroup analysis between purely horizontal (n=12) and mixed phasic head movements (n=8) showed significantly higher values in the last group for the maximum amplitude in the lateral test position with eyes open and closed (p=0.04 and p=0.008, respectively) and for the maximum a-p amplitude with eyes open and closed (p=0.01 and p=0.004, respectively).
Discussion
Similar to previous investigations this study failed to show abnormalities of static posturography in cervical dystonia compared with healthy controls.6 However, dynamic balance was significantly impaired in patients with phasic cervical dystonia whereas patients with tonic cervical dystonia performed similarly to age matched healthy controls. With respect to these findings it is important to emphasise the differences between static and dynamic posturography. Under static test conditions supporting reactions are sufficient to maintain an upright position.13 By contrast, dynamic posturography requires further mechanisms (for example, anticipatory postural reactions and reactive postural responses13) to resist external disturbances. Particularly, the platform used here makes the subject unable to stand still and requires the continuous adaptation of posture to keep balance. Maintenance of balance when standing is a complex process that involves multiple peripheral sensory inputs, central integrating pathways, and efferent outputs.14 15 Postural sway presumably reflects noise and regulatory activity within these afferent-efferent control loops and seems to increase in a non-specific fashion with impaired vestibular, somatosensory, or visual input.8 Vestibular inputs subserve an important role in generating balance corrections to body instability induced by movements of a support surface.16 17 For pertubations in which the support surface is rotated toes upward the compensatory response in the tibialis anterior muscle used to restore balance was shown to be activated by the visual and vestibular systems, and with eyes closed primarily (80%) by the semicircular canals.9 Therefore the significant increase of predominantly lateral dynamic sway parameters in phasic cervical dystonia might reflect a disruption of vestibular input due to repetitive involuntary and mainly horizontal head oscillations. The further increase of maximum sway amplitude in the a-p and lateral test position in the subgroup of patients with mixed involuntary head movements corroborates this notion. In addition, the normal measures in patients with tonic cervical dystonia (table) argue against a primary abnormality of balance control in cervical dystonia which might be suspected from findings of vestibulo-ocular reflex asymmetries1 2 in cervical dystonia and postural instability after unilateral lesions of the basal ganglia or thalamus.18 Increased dynamic platform amplitude and pivot length under visual control in phasic cervical dystonia might indicate that visual input only partially compensates for the disruption of vestibular input.
This investigation for the first time assessed posture in cervical dystonia taking into consideration the different types of dystonic movement (tonic v phasic). Recently in a smaller group of patients similar abnormalities of dynamic balance function to our phasic cervical dystonia collective were reported.19 However, these authors did not try to distinguish between tonic and phasic cervical dystonia. Differences in patient collectives concerning the type of dystonic movement might thus in part be responsible for contradictory findings and reports on directional preponderance of optokinetic nystagmus,1 3vestibular hyperreactivity,3 20 and the subjective visual vertical5 in patients with cervical dystonia.
The clinical implication of impaired dynamic equilibrium with regard to particular leisure or occupational activities in phasic cervical dystonia patients is still unclear and the effect of botulinum toxin treatment deserves further study.
Acknowledgments
We thank K Jeller for her excellent technical assistance.