Article Text

Abstract
OBJECTIVES To make a personal report of a hemianopia due to an occipital infarct, sustained by a professor of neurology.
METHODS Verbatim observation of neurological phenomena recorded during the acute illness.
RESULTS Hemianopia, visual hallucinations, and non-occipital deficits without extraoccipital lesions on MRI, are described and discussed.
CONCLUSIONS Hemianopia, due to an occipital infarct, without alexia, is not a disability which precludes a normal professional career. Neurorehabilitation has not been necessary.
- occipital
- hemianopia
- visual hallucinations.
Statistics from Altmetric.com
Personal reports of illness, disability, and the experience of being a patient, recorded by a trained observer, are of use to the medical profession. None of us plan to make such personal observations, but once the opportunity arises advantage should be taken of it.
I am a right handed neurologist who underwent an aortic valve replacement with a St Jude valve, as well as a double coronary artery bypass graft, on 2 January 1997 when aged 63. A self performed neurological examination in the recovery room disclosed a right hemianopia. Brain MRI and neurological examination (fig 1 and fig 2) demonstrated only a left occipital infarct on both banks of the calcarine fissure and the dense right hemianopia.

Brain MRI. (A) Sagittal view. Note infarct on both banks of the calcarine fissure. (B) Horizontal view.
{kind=link}
{kind=link}
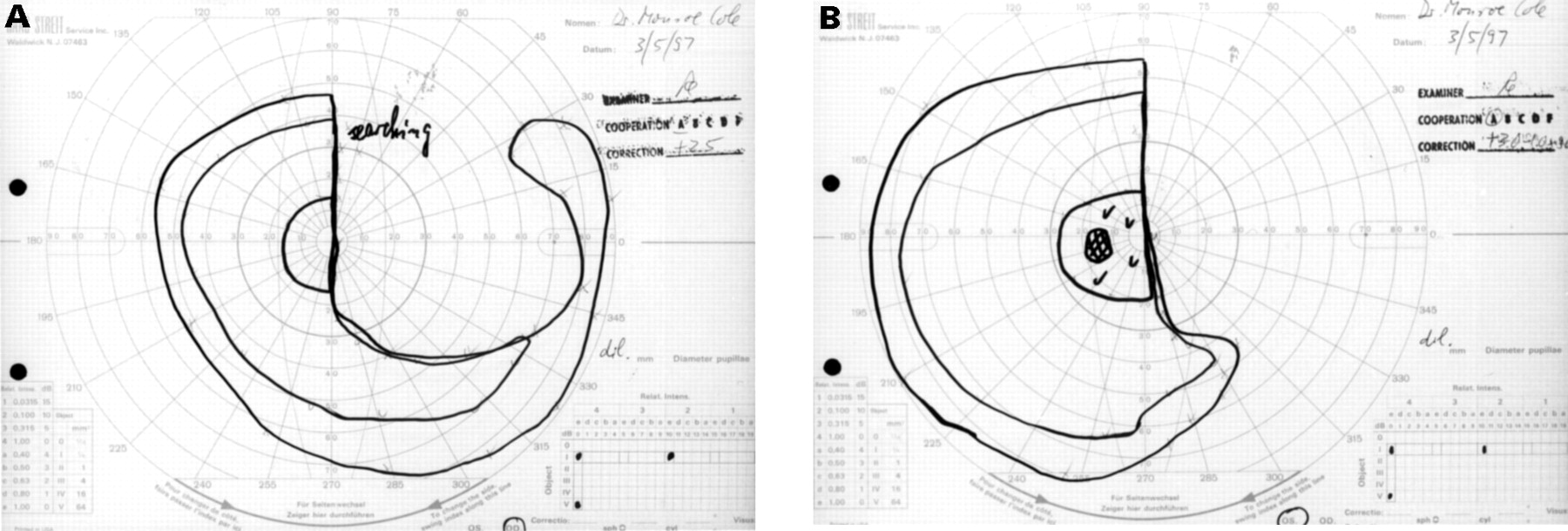
Visual fields by Goldmann perimetry. A. od 3 May 1997; B. os 3 May 1997.
On the second day I became aware of visual hallucinations. These were especially prominent between 3 January and 10 January. (They are, however, not entirely gone after 2 years and appear to be fixed.)
My wife suggested, and continually encouraged me, not to miss the opportunity to record my observations.
At first, virtually all of the hallucinations were in bright colours, but some days they were in muted grey, brown, or yellow. These duller colours would usually appear as swirling drapes, always in the right visual field, but tending to interfere with vision in general. Only twice did I see objects in black and white. Sometimes the colour was not quite appropriate. Often there was a pony with his head cradled in my right arm. I recognised the pony as the one owned by my granddaughter, but the colour was wrong.
Most of the hallucinatory material was recognisable but, as in the example above, the colours did not always fit the object. I saw many horses, dogs, and an even greater number of people, most of whom I could recognise. They moved, danced and swirled, but their purpose was unclear. The hallucinations were neither horrendous nor frightening. Many hallucinations were annoying even though I realised that they were unreal. One hallucination often recurred. There would be a hand thrust out towards me; it would get larger, become distorted, and then shake in a stereotyped manner either in the horizontal or sometimes in the vertical plane. Although the hallucinations interfered with vision, even at their worst I could continue to do some visual tasks such as shaving.
Hallucinations did not occur during sleep and could be differentiated from dreams. During dreams, visual images were bilateral—that is, not confined to the right visual field—and movements were not stereotyped.
In contradistinction to the hemianopic hallucinations described by Kölmel,1 my hallucinations were (1) not motionless; (2) not colourless; (3) not smaller than normal; (4) and not extinguished by eye movement. Finally, (5) my hallucinations were virtually continuous during the first few weeks.
On several occasions I saw what seemed to be a fortification outline. Unlike my migrainous fortification scotomata, however, this did not move across the visual field but stayed in one spot until it disappeared. Furthermore, the edges of the scotomata did not twirl or glisten, as my migrainous scotomata always do.
Certain factors made the hallucinations worse, such as tachycardia, increased heart failure, or an arrhythmia requiring electroconversion—which occurred five times post-operatively. During at least some of these episodes—for example, after cardioversion— I was seen to be mildly confused. The hallucinations were more prominent as the day went on and normally worse when I was taken to an unfamiliar environment.
On discharge, while being driven home, I was constantly surprised by tall, hallucinatory objects along the right side of the road. Sometimes they would be on the right side of a bend in the road, causing me to wonder if the road were blocked. The further the car went, however, the more certain I became that our progress would not be impeded. These hallucinations were stereotyped: large tan or cream coloured buildings reminding me of old public buildings or churches one would see driving in Italy. Such hallucinations persist, but only occasionally, and are very brief and evanescent.
A further peculiarity of these roadside hallucinations are that they have only occurred while I am heading east, as they did when I first was driven home from the hospital. I have never been aware of them while I am heading west—that is, away from home. Other hallucinatory phenomena persist, especially diagonal lines in the right visual field, noted mostly inferiorly. These are not annoying but occasionally distract me while I am reading.
Generally, I am unaware of my hemianopia unless I attend to it or strike things on my right side. I may start a line of writing on the wrong line above if the left side of the line is blank, since I may be unaware of writing on the right side of the line.
On a few occasions illusions were noted. At the end of my hospital bed there was a clamp which, when I first began looking at it, seemed to be a telescope on a military gunsight. After I saw what this actually was, I never had this problem again. Much more unusual were several episodes of false perception of colour. On one such occasion I painted an outdoor chair white. A few weeks later the house was professionally stained white, and a deck was stained battleship grey. I looked at the chair, which was some distance from the house, and wondered to myself why the painters had bothered to repaint my chair the same grey. I walked over to inspect it carefully and found that it was as white as the day I painted it.
I never read throughout my stay in hospital—the first time I ever remember passing time without reading. In fact, I noted, as did observant visitors, that I usually kept my eyes closed. I found vision bothersome although I never had diplopia. The exact quality which bothered me is difficult to analyse. I simply found it uncomfortable to see. After discharge I was constantly encouraged to read and was given a novel with large print. My enjoyment of reading was limited but rapidly improved, so that after the first book was completed I began to read for real pleasure. Medical literature came rapidly thereafter. I had difficulty reading in a moving car, mainly because I would lose the line in which I was reading, but after some weeks I could and would read constantly in a car.
Discussion
Hemianopic hallucinations occur in about an eighth of hemianopic patients.1
In some patients the hemianopic hallucinations occur at the onset of the ictus—for example, case 8 of Lance2—but usually there is a latent period before onset. Most hallucinations consist of familiar people, animals, or objects; some have no obvious familiarity. Lance2 states that hallucinations consist of people and things rather than landscapes and scenes.
WHERE IN THE BRAIN ARE HEMIANOPIC HALLUCINATIONS ORGANISED?
They obviously do not arise from destroyed visual cortex. I would predict that they arise from remaining visual cortex or, more likely, from extrastriate cortex.3 Manford and Andermann4 have recently reviewed various putative mechanisms of visual hallucinations. The physiological cause could be irritable cortex adjacent to the lesion, the original idea of Seguin5 in 1886. As Lance noted,2 “the concept of spontaneous discharge of neuronal circuits in ischemic cortex is attractive.” In one of his patients (case 9) in whom the clinical description does not suggest an epileptic disorder, hallucinations were reduced or abolished by anticonvulsant therapy. Weinberger and Grant6, however, concluded that visual hallucinations “are not due to cortical excitability but are psychological phenomena involving the total integrative activities of the mind.” Cogan7 concluded that episodic hallucinations represent irritative phenomena, while continuous non-stereotyped ones are better explained as a “release phenomenon” by loss of normal control by “higher centers”. Brust and Behrens8 and Fisher9 both support this interpretation. I am unaware of definite data to answer this question.
My original hallucinations were virtually, but not absolutely, continuous, and often recurred in a stereotyped manner. My present hallucinations, which are both simple (diagonal lines) and complex (roadside buildings), do not seem to represent seizures, as they last only seconds and have no other features of seizures, such as an aura, alteration of consciousness, or postictal confusion. Furthermore, the complex, or formed visions only occur under one condition—that is, riding in a car.
IS THE VISUAL FIELD, AS PLOTTED BY PERIMETRY OR CAMPIMETRY, AN ARTIFACT?
Most neurologists accept the fact of a precise retinotopic projection to certain parts of the visual cortex—namely V1, V2, and V3—which correspond to Brodmann’s areas 17,18, and the posterior part of 19.
The retinotopic map was originally deduced, mainly by Holmes and Lister10 and Holmes11-14 studying wounded soldiers. By carefully correlating the site of the entrance wound, sometimes supplemented by radiography, with perimetry Holmes, and Riddoch15 were able to describe the retinotopic organisation of the visual cortex. In these investigations they corroborated the work of Inouye in the Russo-Japanese war and also the papers of Marie and Chatelin,16 Axenfeld,17Dimmer,18 and Uthoff19 (see also Symonds20 and Spalding21). Holmes’ map was revised by Horton and Hoyt22.
In certain respects the visual field, as demonstrated by perimetry or campimetry, is an artifact of the method used: monocular or binocular, static or dynamic, fixation or gaze. Consider, for example, some of the research on macular sparing or splitting. Holmes11 14showed that the central 10° of the visual field is projected to the most posterior part of the striate cortex, including that part of the posterolateral occipital tip. Cogan7 indicated that macular sparing is more common with parietal or parieto-occipital lesions and less common with temporal or occipital lesions. He also states that macular sparing is absent with “paracentral scotomas from lesions in the occipital pole.” But cases 14, 15, and 19 of Holmes and Lister10 show just such sparing. Cogan,7however, seems to accept the idea that macular sparing or splitting may be an artifact of testing.
Williams23 showed that macular splitting demonstrated by fixation could be converted by having the subject gaze at a second stimulus about 5° from the fixation stimulus. He emphasised the factor of attention, or relative lack of it, to the fixation point as the primary artifact of macular sparing or splitting. Verhoeff24 also thought that macular sparing was only apparent and hypothesised that with occipital lesions it was due partly to instability of fixation and partly to the establishment of an eccentric fixation point—a so called pseudofovea (see also Grayet al 25).
I find that preservation of my temporal crescent is helpful20 when examining confrontational visual fields. As my stimulus enters my preserved temporal crescent, it provides better orientation to the stimulus position than simply “knowing” where the stimulus is by position perception.
FORMED VERSUS UNFORMED VISUAL HALLUCINATIONS
Probably most neurologists (see Kennedy’s discussion in Cushing26 and Weinberger and Grant6 for reviews) consider that complex visual hallucinations are more likely found with temporal lobe lesions, and that simple ones, such as photopsias, are of occipital origin. Horrax27 strongly supported this view, as did Cushing. Horrax and Putnam28state more strongly that “formed figure hallucinations are not produced by occipital tumors.” (Their material consisted entirely of tumours.)
A number of observers (for example, Weinberger and Grant6) have concluded that formed or unformed, simple or complex, visual hallucinations may arise anywhere from the retina to the visual cortex. It should be recalled that the first description of hemianopic hallucination by Seguin5 in 1886 described the hallucinations as “simple,” but they consisted of chairs and chickens. It behoves us to be more specific when discussing visual hallucination. The visual hallucinations of hemianopia, delerium, or seizure are likely to have different mechanisms.4 How they relate to one another is less certain.
EYE MOVEMENTS
I am possibly the only person who has ever been tested for eye movements, preoccipital and postoccipital lesion. Before the lesion, hypometric and hypermetric saccades were recorded, and were considered normal for age, when I was tested at the age of 62. Postlesion, the hypometric and hypermetric saccades were greater in degree, reaching a “staircase” pattern. Furthermore, when I searched for a stimulus in the blind hemifield, the strategy of an overshoot saccade, as described by Meienberg et al,29 was used, thus placing the stimulus in the seeing field.
“BLINDSIGHT” AND THE RIDDOCH SYNDROME
The perception of movement is thought to be organised in the middle temporal area comprising anterior area 19 and part of posterior area 37 (V5). (see Symonds,20 Douglaset al,30 and Barton and Sharpe31 for discussion of striate and extrastriate cortical organisation.) “Blindsight” is thought to occur if this area is intact. “Blindsight” is used by most authors to mean the ability to identify movement or orientation of stimuli without conscious awareness of having seen the stimulus.
“Blindsight” differs in certain respects from the so called Riddoch15 syndrome. Riddoch’s patients were consciously aware of movement in the blind hemifield, but not of shape or colour. His patients probably had sparing of V5.32
I have been tested by Drs Lea Averbuch-Heller and John Stahl, by the magnetic search coil technique, for both “blindsight” and the Riddoch phenomenon and demonstrate neither, suggesting that V5 is lesioned. However, Barton and Sharpe31 conclude that survival of V5 is not sufficient for “blindsight”. My MRI does not indicate a lesion in V5.
IMBALANCE
Riddoch15 also reported in his case that when there is any remaining vision in the blind hemifield, vision may actually increase the difficulty of ordinary life, as the disparity of the two half fields is “frequently sufficient to affect...equilibrium in walking.”
I too have inconstant imbalance. This was worse early in the course and soon after discharge from hospital. It was notably worse in unfamiliar environments and when vision was less clear. It still persists in unfamiliar environments, with decreased vision—for example, in reduced light, and also with fatigue. Usually it is not a problem, but in certain circumstances, such as going down stairs, I try to go more slowly and to hold onto the railing. The imbalance cannot in my case be ascribed to any type of “blindsight,” as noted above. Magnetic resonance imaging shows no lesion in the cerebellum, brainstem, or anywhere else to explain it. Examination of vestibular function demonstrated no abnormality.
This postural disturbance was well discussed by Rondotet al.33 They pointed out that imbalance, or as they suggested “visual ataxia”, which is to be differentiated from optic ataxia,34 occurs often in patients with homonymous hemianopia. The defect is not of labyrinthine origin, but may be a recentring of the centre of gravity in relation to the spared visual field. Brodal,35 in discussing certain otherwise unexplainable symptoms after his stroke, concluded “...destruction of even a localised part of the brain will cause consequences for several functions in addition to those which are more specifically dependent on the region damaged.” Further, “...in any brain damage one may expect to find disturbances in function which—according to current views—are not primarily served by the damaged part.”
VISION IPSILATERAL TO THE LESION
Rizzo and Robin36 have studied vision in the hemifield ipsilateral to a V1 lesion and concluded that it is impaired. The authors hypothesised that the deficit was either on the basis of diaschisis, or due to a lesion of V2, which has a strong transcallosal projection—at least in monkeys. The diaschisis impairs transcallosal connections to the opposite hemisphere from V2, V4, and V5. Furthermore, they hypothesised that visual attention or vigilance is impaired. Such an attention deficit is not measured by usual perimetry but a method thought to demonstrate its effect was devised by Williams.23
This deficit may best be described in the words of Rizzo and Robin36 as “complaints of tired eyes, things looking different, blurred or funny.” I do not find that I shun visual tasks such as reading, even under difficult conditions. I do need a great deal of light on any subject. For example, looking for something underneath a shelf or table is particularly difficult. Furthermore, I suspect that my visual attention is impaired as I often look for something, and fail to see it.
LIVING WITH A HEMIANOPIA
The prognosis for recovery of an occipital hemianopia depends entirely on the nature of the causative lesion. One might be hopeful of some recovery after closed head trauma, haemorrhage, infection, or inflammation. When the lesion is an infarct, (the most frequent cause of of an occipital hemianopia), there is probably little chance of recovery, depending on the extent of actual infarction with regard to the ischaemic penumbra.
Of more importance is the disability caused by such a hemianopia. Even intelligent patients often are surprised when a hemianopia is demonstrated, despite the fact that it has been so demonstrated on numerous examinations (see, for example, case 1 of Williams and Gassel37). Insight into the existence of a hemianopia generally relates to the ability to function in life situations.37 Compensation for the visual field defect probably is due to the deployment of “gaze vision”—that is, not attending to a fixation point; the use of searching saccades; and possibly to development and use of a pseudofovea. I personally am unaware of my hemianopia unless I take pains to fixate. I also find that unless specifically informed, my colleagues, patients, friends, and people I meet are unaware of my deficit.
I am more bothered by an intermittent hallucination of diagonally placed, thin blue lines at 30–40° below the horizontal meridian and 25–35° to the right of the vertical meridian. Even this is only annoying if I am reading, but does not hinder me in doing so. I have to be careful not to run into people on my right, or worse, to ignore them. I have already alluded to my generalised difficulty with vision and some imbalance.
Somewhat more vexing to me is the search for objects. I interpret this problem to be a deficit of visual attention rather than of vision. Refractive correction has made no difference and the searched for object is not necessarily in the hemianopic field.
My only real handicap is being unable to drive. I do not drive because I think it is too dangerous and also because it is illegal. Being unable to drive in the modern world is a mixed blessing. However, for the person who lives alone and is unable to arrange for a driver, the handicap could be severe.
Some programmes of visual rehabilitation, including the use of Fresnel prisms,38 have been tried to improve the function of the hemianopic patient. I have little use for this approach. Nor do I think that so called neurovisual rehabilitation (see Kerkhoffet al 39)—that is, saccadic training— is of much use as spontaneous adaptation occurs without “treatment”. A good, randomised control study would be necessary to change my opinion. What is more important is that the patient slows down to make certain that saccades are directed, actually overdirected, into the hemianopic field. I would say to a patient who has an occipital hemianopia without alexia, “count your blessings and reflect on how bad it might have been.”