Article Text

Abstract
OBJECTIVES To report on a 10 year follow up of patients with idiopathic Parkinson’s disease, particularly with respect to mortality and the effect of early treatment with bromocriptine.
METHODS The patients are from the 149 new patients recruited for a double blind, randomised study of low dose levodopa-carbidopa versus low dose bromocriptine. Patients were examined neurologically at least yearly. Neuropsychological examinations were performed at 0, 3, 5, and 10 years. Mortality and cause of death in these patients were compared with the Australian population using standardised mortality ratios (SMRs). Mortality and disease progression were compared by sex and treatment group. Predictors of death within 10 years, nursing home admission, and progression in Columbia score of ⩾20 points were examined by logistic regression analysis.
RESULTS Thirteen patients were excluded as having atypical Parkinsonism and six were lost to follow up. All available patients have been followed up for 10 years. Fifty patients (38%) were dead by 10 years and 63 by the last follow up. The SMR was 1.58 for all patients (p<0.001). There was no significant difference in SMRs between the sexes. The mean duration of disease until death was 9.1 years. Parkinson’s disease was thought to have contributed substantially to the death of 30 patients. The most common cause of death was pneumonia. Women progressed at a similar rate to men until 8 years, when the severity of their disease as measured by Hoehn and Yahr stage became greater (p<0.05). Older age of onset correlated with increased risk of death but the SMR was increased even in those aged <70 years (SMR 1.80, p=0.03). Early use of bromocriptine did not reduce mortality or slow progression of disease. One quarter of all patients had been admitted to nursing homes by 10 years. Only four patients were still employed.
CONCLUSIONS Mortality in Parkinson’s disease remains increased despite low dose levodopa-carbidopa therapy and no additional benefit was gained from early use of bromocriptine. Duration of disease was similar to that in the era before levodopa.
- Parkinson’s disease
- mortality
- bromocriptine
Statistics from Altmetric.com
The cohort of new patients recruited over 3 years into the Sydney Multicentre Study of Parkinson’s disease has now been followed up for a minimum of 10 years. It is timely to look at disease progression, mortality, and the influence of bromocriptine in this closely observed group of patients. Patients were randomised to receive either low dose levodopa-carbidopa (⩽600/150 mg/day) or low dose bromocriptine (⩽30g/day), although few patients remained on bromocriptine alone for more than 2 years.1 The influence of early use of bromocriptine on the appearance of dyskinesia and end of dose fluctuations has been reported previously.1
Despite levodopa, the mortality of people with Parkinson’s disease remains increased compared with the general age matched population,2-8 although survival may be increased with levodopa by about 5 years especially in younger patients.2 6 8-12 Initial reports when levodopa first became available suggested that life expectancy returned to near normal with this agent.13-15 This is now thought to have reflected the benefit of levodopa early in the course of the disease in drug responsive patients, who then “caught up” in the mortality stakes by the early 1980s.2 16
The aim of this report is to:
-
Compare mortality in our cohort of patients treated with low dose levodopa-carbidopa and/or bromocriptine with the age matched Australian population
-
Assess predictors of increased mortality in Parkinson’s disease
-
See if early use of bromocriptine lessens mortality
-
Compare causes of death with the age matched general Australian population
-
Provide data on disease progression and employment
-
Consider risk factors for nursing home placement.
Materials and methods
This report is based on data collected from the patients who participated in the Sydney Multicentre Study of Parkinson’s Disease. Between 1984 and 1987, 149 patients were recruited with Hoehn and Yahr stage 1 to 3 disease. They have been followed up for as long as 13 years. As all available patients have completed 10 years, this time is used for most analyses. However, deaths are included up to 13 years for comparison with the general Australian population.
Table 1 shows the various patient subgroups. At 10 years, 122 of 126 patients thought to have idiopathic Parkinson’s disease and completing more than 6 months of the study were accounted for. Four were lost to follow up. We originally had 70 men and 56 women. These 126 patients are used for analysis of disease progression during the 10 years. Of the 10 patients who did not complete the first 6 months of the study (phase 1), eight were accounted for at 10 years by telephone or personal examination. Two were lost to follow up. Most of those lost to follow up at 10 years had moved from the Sydney area and information regarding mortality was not available. These 130 patients (122 plus eight) are the basis for analysis of mortality. Two patients failed to complete the first 6 months due to death; to exclude patients who did not complete phase 1 from mortality analysis would have allowed a 6 month survival advantage to the other 126 patients. Of 13 patients recruited into the study but later found on clinical grounds not to have idiopathic Parkinson’s disease,1 nine are dead and four are still alive (one essential tremor, one post-traumatic lesion of the basal ganglia, one undetermined congenital abnormality, and one pinealoma). These 13 patients are not discussed further.
Mortality for 10 and up to 13 years of follow up. Patients who continued after the dose finding phase (phase 1) are considered as full trial patients. Those who did not complete this are listed as phase 1 incomplete. An additional 13 patients considered to have atypical Parkinsonism before 5 years are excluded
The diagnosis of Parkinson’s disease was based on the presence of two of the following: bradykinesia, resting tremor, and rigidity, in the absence of features suggestive of atypical Parkinsonism.1In the first 5 years, the emphasis of the study was a comparison between low dose levodopa-carbidopa (⩽600/150 mg/day) and low dose bromocriptine (⩽30 mg/day) therapies.1 Patients were seen at least twice yearly for 5 years then at least yearly thereafter. When possible, patients in nursing homes were visited yearly. All baseline and annual visits were performed by the one investigator (MAH). Fourteen patients have donated their brains for pathological studies.
Neurological assessments included a modified Columbia Score (maximum score 102),17 a modified North West University disability scale (NWUDS),18 Hoehn and Yahr stage,19 and standard questionnaires of symptoms and side effects. Patients were seen by a neuropsychologist (WG) at baseline, 3 years, 5 years, and 10 years and undertook a battery of neuropsychological tests. Definitions of dementia, late side effects, symmetry, progression rate, and balance disorder have been previously reported.1 20 21
Patients were examined before commencing medication at two separate visits but after this all examinations were done on medication, during the “on” phase once fluctuations were present. Hoehn and Yahr staging reflected the most appropriate global score for each patient. Hoehn and Yahr stage did not necessarily progress from one stage to the next, but often decreased on treatment and occasionally jumped more than one stage higher between visits. The first occurrence (if any) of stage 1−2 severity is used to calculate the initial date of that stage. The first occurrence of stage 3 after that date is used to calculate the time from stage 1–2 to stage 3. Similarly, the first occurrence of stage 4 or 5 illness after stage 3 is used to calculate the time to progress from stage 3 to stage 4 or 5.
Cause of death was notified by certifying doctors and family and in many cases the terminal illness was known to MAH. The main condition underlying the terminal event is considered as the cause of death. Comparison with the general Australian population was made with unpublished data provided by the Australian Institute of Health and Welfare. The International Classification of Diseases codes, ninth revision, was used.22
STATISTICS
The ratio of observed deaths to expected deaths compared with people of the same age in the same calender years in the general Australian population provided the standardised mortality ratio (SMR). Confidence intervals to the 95% level (95% CIs) were calculated to determine a range of valid values for the true SMR. Continuity corrected χ2 statistics were used to test whether the observed number of deaths differed significantly from the expected number. Relative death rates (RRs) were calculated to compare SMRs of women and men, with 95%CIs. To test if the RR differed significantly from 1, a χ2 test was used. Kaplan-Meier plots were also used to examine survival.
Possible predictor variables for death within 10 years of presentation, nursing home placement, and progression in Columbia score of ⩾20 points, were entered univariately into a logistic regression analysis. To test for differences in progression in the Columbia score and the Hoehn and Yahr stages by sex the Mann-Whitney test was used. For testing matched pairs data, such as change in score at 10 years for a patient, Wilcoxen tests were used.
This study was approved by the ethics committees of the participating Sydney hospitals. All patients gave informed consent.
Results
MORTALITY
Fifty patients (38%), consisting of 34 men and 16 women, of 130 patients available for follow up, died during the first 10 years. Sixty three patients (48%) had died by the last follow up (maximum 13 years). The SMR for the whole cohort was 1.58 (95% CI 1.21–2.02) indicating a higher rate of death than in the age matched Australian population (p<0.001). Death was more frequent in older patients, as expected. The SMR was also increased for younger onset patients compared with the age matched general population and there was no significant difference in the SMR between older and younger patients (table 2). From 1988 to 1997, observed death rates were in excess of expected death rates (SMR >1) despite low dose levodopa or bromocriptine therapy. The risk was higher in men (SMR=1.89, 95% CI 1.36–2.55) than in the Australian male population (p<0.001). The SMR for women was 1.19 (95% CI 0.76–1.82). This was not significantly different from the death rate in the general Australian female population. Comparison of SMR for male and female patients gave a relative rate of 0.63 (95% CI 0.35–1.09) and was also non-significant (p=0.11) as the confidence interval encompassed unity.
Mortality ratio of observed to expected deaths up to 13 years of follow up by age group at time of death and by sex
Predictors of mortality during the first 10 years of follow up are shown in table 3. Multivariate analysis showed that only older age of onset, randomisation to bromocriptine, and rapid prestudy disease progression were predictive of increased mortality. However, if patients were able to remain on bromocriptine for more than 1 year after randomisation to this drug (43 patients), no increased mortality was found.
Univariate and multivariate analysis for predictors of mortality during the first 10 years of the study, excluding those who die after their 10 year visit or who were lost to follow up at 10 years. Bromocriptine >1 year indicates those patients who were randomized to bromocriptine monotherapy and were able to continue bromocriptine monotherapy for at least 1 year
By 10 years, there were 29 deaths among the 63 patients randomised to bromocriptine and 33 at last follow up. Twenty two of these 33 had ceased bromocriptine well before death. Their mean time taking bromocriptine was 22.4 (SD 21.9) months. The mean time from ceasing bromociptine until death was 63.7 (SD 28.3) months. The reasons for stopping bromocriptine in these patients included confusion (11), postural hypotension (six), lack of efficacy (two), peripheral oedema, Raynaud’s phenomenon, and abnormal liver function (one each). Only two patients were on bromocriptine monotherapy when they died. The other patients were receiving levodopa-carbidopa alone or in combination with bromocriptine.
There were 21 deaths among the 67 randomised to levodopa and 30 at last follow up (six of those not completing the first 6 months did not commence randomised trial medication but took levodopa-carbidopa after leaving the trial).
CAUSE OF DEATH
The causes of death are shown in table 4. The distribution of causes of death was similar for both randomisation arms. Pneumonia was the most common cause of death (19/63, 30%) and all but four of these patients were severely physically disabled (Hoehn and Yahr stage 5) or demented. Four were moderately physically disabled (stage 4) and three of these had additional cerebrovascular disease. The comorbidity of other age related diseases including ischaemic heart disease, stroke, and carcinoma was prominent in the other causes of death. Parkinson’s disease was considered to have contributed to the deaths of 30 patients, based on the immediate cause of death and the degree of disability from Parkinson’s disease at the time of death: those with pneumonia, one who drowned, and some of those with stroke and cardiovascular disease who were already bed bound and often demented and thus not suitable for intensive therapeutic intervention or rehabilitation. The contribution of Parkinsonism to death was most apparent in those aged 50–69 years at entry (table5).
Cause of death for all patients dying before or after 10 year follow up. Other includes drowning (one), gastric haemorrage (one), herpes encephalitis (one), peritonitis and renal failure (one)
Proportion of patients in whom Parkinson’s disease (PD) makes a significant contribution to death according to age at presentation
SEX
Seventy men and 56 women completed the first 6 months. Baseline characteristics were similar for both sexes. Dyskinesia developed earlier in women20 but by 10 years there was no significant difference in its prevalence. Significantly more women than men experienced end of dose failure by 10 years. However, when dose of levodopa was controlled for in the regression analysis, female sex was not a significant factor in the appearance of end of dose failure although the levodopa dose for men and women was proportional to their weight. At 10 years men took a mean of 787 (SD 380) mg/day whereas women took a mean of 681 (SD 361) mg/day of levodopa.
{kind=link}
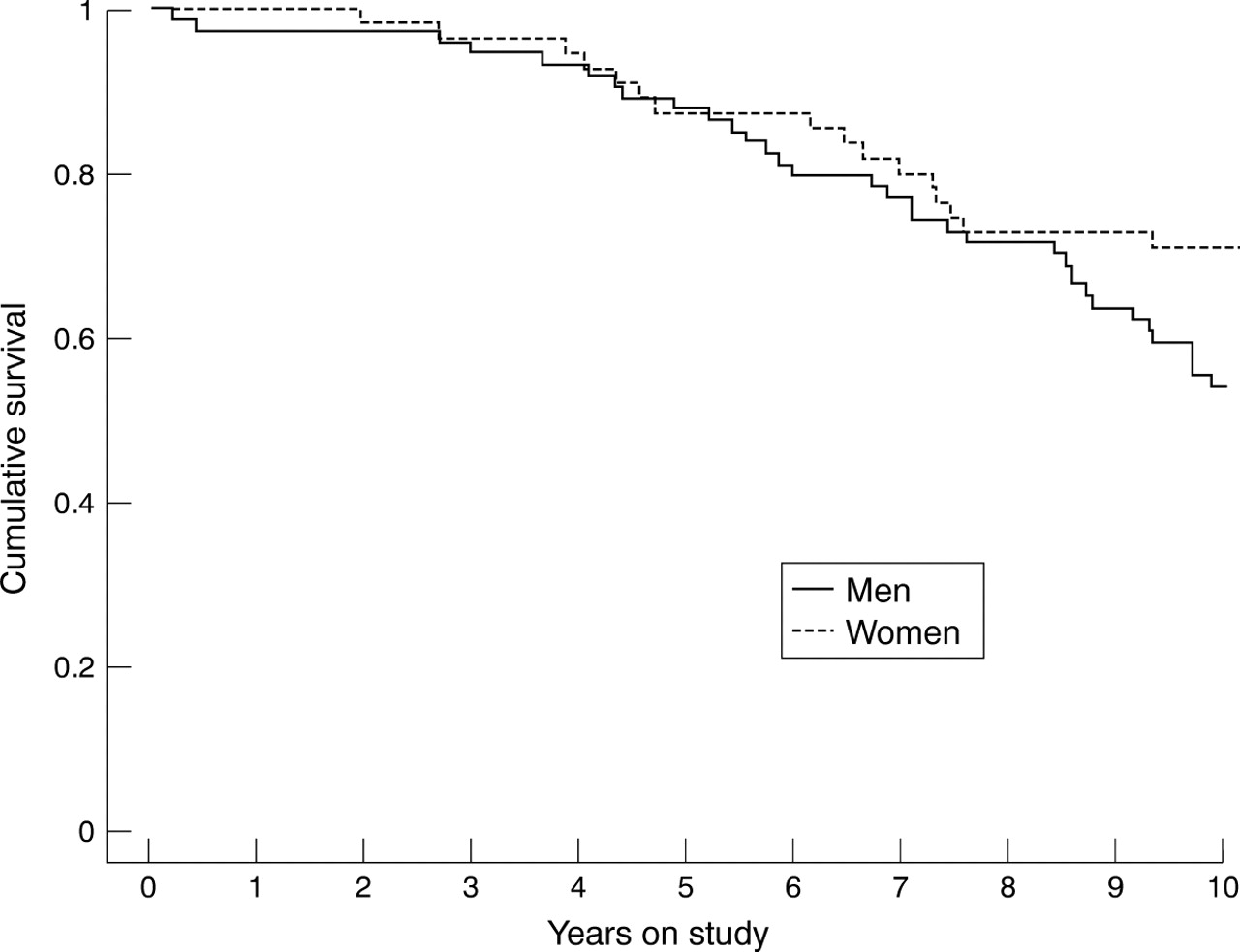
Cumulative survival of patients with Parkinson’s disease by sex up to the 10 year visit. Cox’s regression indicates no statistical difference in survival times by sex (p=0.09).
The rate of increase in modified Columbia and North West University disability scales was no different for men and women to 10 years. By 10 years there was a divergence in Hoehn and Yahr stage, with women having a higher score than men (mean for women=3.55, mean for men=3.11, Z=−1.9739, p=0.05).
The mean age of death for all patients was 74.5 (SD 8.2) years; 74.5 (SD 7.9 ) years for men and 74.3 (SD 8.9) years for women. The mean duration of disease from onset of symptoms to death for all patients was 9.1 (SD 3.6) years with a range of 2–15 years. The mean duration of disease from presentation until death for women was 7.6 (SD 3.3) years and for men it was 8.1 (SD 3.4) years. Although women who have died to date have done so unusually early, the overall percentage of women dying in the study was less than for men (36.2%v 53.8%). The difference was not statistically significant when the SMR was considered (see above mortality section) or when survival times by sex were analysed by Cox’s regression (p=0.09), figure.
PROGRESSION OF MODIFIED COLUMBIA SCORE
Logistic regression was performed for patients not on anticholinergic drugs at baseline to discover which baseline variables predicted an increase in Columbia score by 20 or more points in 10 years. Univariate analysis showed that increasing tremor score (p=0.01), female sex (p=0.02), and increasing age (p=0.006) were predictive. Multivariate analysis showed that only older age predicted deterioration by 20 or more points in the Columbia score (p=0.008, odds ratio 2.41 (95% CI 1.24–4.66)). Randomisation to bromocriptine (p=0.52) or continued use of bromocriptine for more than 1 year (p=0.68) did not influence deterioration in Columbia score by 10 or 20 points.
PROGRESSION OF HOEHN AND YAHR STAGE
At baseline eight of 126 patients were stage 1, and 75 of 126 patients were stage 2. By 10 years, 29 of 83 patients (34.9%) were dead. Sixty one who were stage 1 or 2 at baseline progressed to at least stage 3 within 10 years. The median was 3.5 years. Thirty four patients progressed further to stage 4. The median time was 7 years. Eleven patients progressed to stage 5 by 10 years in a median time of 6 years.
At entry, 43 of 126 patients were stage 3. Seven died still in this stage and 14 after reaching stage 4 or 5, a total of 21 deaths by 10 years (48.8%). Thirty two patients reached stage 4, taking a median of 4.5 years. Nine patients reached stage 5 taking a median of 6.5 years. Numbers of patients at each stage are shown in table 6. Patients who were dependent on others (stage 4 or 5) or dead, ranged from 8% at 2 years to 71% at 10 years. There was no significant difference between randomisation groups or use of bromocriptine for >1 year compared with patients on levodopa for progression through the Hoehn and Yahr stages.
Distribution of Hoehn and Yahr stages and number dead at each 2 year interval. Percentage calculations for stages are based on those patients examined at that visit. Percentage dead are based on all patients still followed up even if data for live patients are missing from that visit
BENIGN PROGRESSION
Although no patient stayed at stage 1 for 10 years, 13 patients completed 10 years and did not progress past stage 2. They had mild or no fluctuations. Dyskinesia, if present, was not troublesome. None of these patients had dementia or hallucinations and all were very responsive to drugs. There were 10 men and three women. Six had bradykinesia and rigidity only and seven had tremor, bradykinesia, and rigidity at presentation. Their age ranged from 40 to 63 years at entry with a mean of 50.3 (SD 8.3) years. Four of the men were still working and the three women were close to achieving full home duties. The mean levodopa dose was 604 (SD 314) mg/day. Eight patients were on bromocriptine (mean=18 mg/day) or pergolide (mean=3.7 mg/day) in addition to levodopa. One patient used selegiline and four used benztropine.
EMPLOYMENT
Employment was examined in those aged less than 60 years at entry to the study. These results are shown in table 7. The usual occupation for women was full time home duties rather than outside employment, particularly in those aged over 50. All nine patients who were aged less than 50 years at presentation who retired did so because of their Parkinson’s disease. Most patients aged 50–59 years at presentation (25 of 29) retired due to their Parkinson’s disease or dementia. Only one retired due to his age; three retired due to intercurrent disease.
Employment. Working includes those in their normal full time occupation and women who are running a home without need for help. Women who require help with home duties are grouped with those who have retired from full time work
NURSING HOMES
By 10 years, 29 of 126 (23%) patients had been admitted to a nursing home. The main reasons were confusion and increasing dementia (20 patients), often associated with increasing physical frailty and falls. Physical frailty and immobility without dementia were prominent reasons in nine patients. These nine patients all lived alone whereas 13 of 20 patients with dementia had a relatively healthy spouse at home. The age range of those admitted to nursing homes was 59–84 years at time of admission (median=77 years).
Baseline and within study variables that predicted nursing home admission are shown in table 8. Multivariate analysis showed that only increasing age and confusional states predicted nursing home admission within the first 10 years of diagnosis of Parkinson’s disease. By the end of 1997, 25 of 29 (86%) patients admitted to a nursing home were dead. The mean duration of survival in nursing homes was 34 (SD 20.5) months.
Univariate and multivariate predictors of admission to nursing homes by 10 years
Discussion
Patients in this prospective study were closely followed up by one group of neurologists from the time of initiation of therapy with either low dose levodopa or bromocriptine, for at least 10 years or until death. Close contact has been maintained and visits continued after nursing home entry and well after cessation of the drug trial, which officially ended after 5 years. We were often aware that death was imminent. Thus the cause of death and the contribution of Parkinson’s disease to death in these patients was better known than from just death certificate information, which has been found inaccurate.7 19 23 However, when sudden death occurred, death certificate information was taken.
We have tried to exclude atypical Parkinsonism. The group had mild to moderate Parkinson’s disease, Hoehn and Yahr stage 1–3, at presentation. Most had rest tremor and all showed a response to levodopa when they eventually received it.
PREVIOUS MORTALITY STUDIES
The main mortality study of the prelevodopa era is that of Hoehn and Yahr in 1967 based on patients seen between 1949 and 1964.19 They found that the mortality rate was 2.9 times that expected. The first reports after the introduction of levodopa suggested that mortality was reduced compared with that of the general population. (SMR 0.95–1.03).6 13-15 24 25 Later studies reported an increase in mortality in Parkinson’s disease despite more widespread use of levodopa (SMR 1.6–2.6).5 16 26-30 An explanation for the initial improvement of mortality in the first few years of the levodopa era was offered by Clark2 who argued that levodopa delayed death in a cohort of patients with Parkinson’s disease who were still in the levodopa responsive phase of their disease. This was supported by the studies of Uitti et al,8 and of Curtis et al 16 who noted an SMR of 1.45 after 6 years, but an SMR of 2.59 after 12 years. It suggests that the benefit of a good early response is lost as the disease progresses. The period of improved survival thus corresponds to the “honeymoon period” when patients are most responsive to levodopa. By contrast, the DATATOP study has found a mortality rate for all patient groups similar to that of the age matched American population after an average of 8.2 years of observation.31 This may be in part due to the inclusion of only patients with stage 1 and 2 disease and the exclusion from the DATATOP study of patients with pre-existing serious conditions other than Parkinson’s disease. In the general population no such exclusions were made.
CURRENT MORTALITY STUDY
Our study adds to the evidence for increased mortality in Parkinson’s disease despite using levodopa. Duration of disease and life expectancy cannot be reliably given as only some of the cohort have died. However, we have a duration of disease of 9.1 years with 46% of patients dead, whereas Hoehn and Yahr in the prelevodopa era19 found a disease duration of 9.4 years with 44% of their patients dead. Their mean age at death was 67 years whereas ours was 74.5 years. They noted that the mean age at presentation was rising between 1949 and 1964 from 54.3 to 61.9 years with an overall mean of 55.3 years despite excluding those thought to have secondary parkinsonism. The mean age at presentation in the Sydney study, 62 years, is similar to some contempory studies.4 23 31 32It is probable that with the increasing age of the general population, there is a rise in the mean age of presentation and subsequently of the mean age of death but the duration of disease may not be altered.
The Sydney Multicentre Study aimed at low dose medication for 5 years (mean levodopa dose 471 mg/day at 5 years for levodopa used alone,1 and 738 mg/day at 10 years). Perhaps our patients were inadequately treated. This, however, seems unlikely as patient satisfaction determined our dosage adjustments.20 All patients dying from the complications of Parkinson’s disease had reached stage 4 or 5 when non-levodopa responsive features such as gait and balance disorder, dysarthria, dysphagia, and the risk of aspiration pneumonia were prominent. In many of these, confusion and hallucinations limited the dose of levodopa.
Our mortality rates were not increased in the first 3 years of the study compared with the general population and deaths during these early years were due to non-parkinsonian causes. The proportion of deaths in which Parkinson’s disease made a major contribution was about equal to our excess in mortality throughout the 10 years subsequently.
CAUSES OF DEATH
As in previous studies pneumonia was the most often known cause of death in patients with Parkinson’s disease7 19 31 33 34 probably due to immobility and increased risk of aspiration. In the late stages of disease, when quality of life is profoundly poor, pneumonia is often best left untreated.
Death from carcinoma was not significantly different from that in the general Australian population. Some studies have shown reduced risk of death from cancer in parkinsonian patients19 34 35 but not others.7 36 Death from cerebrovascular disease was increased, as noted by Gorrell et al.34
PREDICTORS OF EARLY DEATH
As might be expected, the age at onset was the most significant predictor of death within 10 years. Parkinson’s disease did not contribute to the death of any patient younger than 50 years at presentation during this period of follow up. Parkinsonism and its complications contributed to nearly half of the deaths. An unexpected finding was that the highest proportion of deaths in which Parkinson’s disease contributed, occurred in patients aged 50–69, but further analysis of causes of death showed that ischaemic heart disease and cerebrovascular disease became much more prominent as causes of death in patients aged over 70. Some studies have shown that it is particularly the younger patients with Parkinson’s disease who have benefited from decreased mortality since the introduction of levodopa.10 11 30
More rapidly progressive disease at presentation also predicted death within the first 10 years. Higher Hoehn and Yahr scores have been found to increase risk of death in many studies.5 8 33 37 In this study proportionally more of the stage 3 patients were dead by 10 years. Dementia and imbalance were associated with older age and were only univariately predictive of death in 10 years if present at baseline.20 21 An increased death rate, if dementia occurs with Parkinson’s disease, has been noted previously.4 5 33 38
BROMOCRIPTINE
We were unable to show any protective effect from bromocriptine on longevity or disease progression in new patients with Parkinson’s disease. Olanow et al also detected no difference in the extent of change in disability in patients randomised to levodopa versus bromocriptine.39 Przunteket al reported that “the mortality risk associated with levodopa therapy was reduced by more than 50% by its combination with bromocriptine”.40 However, about half of the 587 patients had discontinued study medication by the time of analysis, and the life status was unknown in 48% of these.
The results of the United Kingdom study, in which bromocriptine monotherapy is compared with levodopa and levodopa-selegiline combination, are awaited.23 It is of interest that in this study randomisation to selegiline was associated with increased mortality. It was not explained by increased cardiovascular events, autonomic problems, or drug interactions. As in the United Kingdom selegiline-levodopa combination group,23 we noted increased problems with dementia and imbalance in the bromocriptine group, even at baseline, although the differences were not statistically significant (19% v 11% for dementia and 18% v 8% for imbalance).1 Due to these problems, bromocriptine was replaced early with levodopa-carbidopa and death did not occur for many months or years after the cessation of bromocriptine. We thus suspect that the poor results in our bromocriptine group were artificial, resulting from a chance selection of more severely affected patients in the randomisation process. In support of this, ability to remain on bromocriptine for more than 1 year neither increased nor decreased mortality. We are reluctant to conclude that bromocriptine increased the mortality in patients randomised to that drug, despite our multivariate analysis showing that randomisation to bromocriptine was associated with increased deaths within 10 years of presentation.
NURSING HOMES
Confusion and hallucinations often precipitated admission to nursing homes. Physical frailty alone was often insufficient to cause nursing home entry unless the patient lived alone. About half of the patients had died within 3 years of entry to nursing homes. Increasing age was an expected predictor of nursing home admission. Severity of Columbia score, activity of daily living score, or Hoehn and Yahr stage did not predict admission to a nursing home. Goetz and Stebbins found that hallucinations were a significant factor in nursing home placement but not necessarily severity of cognitive decline.41
Ebmeier et al reported that in his community study of Parkinson’s disease, nearly 24% lived in a hospital setting or specialised residence for elderly people.5 A quarter of our patients required nursing home admission by 10 years. Given the costs of nursing home care, better treatment for confusional states and hallucinations is warranted.
EMPLOYMENT
Employment is rarely reported in studies of the progression of Parkinson’s disease. However, our results give cause for optimism, at least for the first 5 years in patients with younger onset. Information was collected prospectively and certificates to enable retirement on medical grounds were often supplied. In most cases the reason for retirement was Parkinson’s disease rather than age or intercurrent illness in these younger patients. A previous report of an older group of patients who were retrospectively questioned found that Parkinson’s disease was responsible for about 40% of patients retiring from employment early.42
HOEHN AND YAHR PROGRESSION
Similar to the experience of Hoehn and Yahr,19 the rate of progression varied greatly and about 10% of patients followed a benign course. A comparison of our results for severely disabled patients (stage 4 or 5) and dead patients with Hoehn and Yahr’s prelevodopa results19 shows considerable similarity with 22% of our patients disabled or dead by 4 years compared with their 28% of patients with up to 5 years of follow up. At 10 years 71% of our patients were disabled or dead compared with 61% of Hoehn and Yahr’s patients who were followed up for 5–9 years and 83% who were followed up for 10–15 years.
COLUMBIA SCORE PROGRESSION
Age was a major determinant of increasing the Columbia score over 10 years. This may be due to the presence of more levodopa unresponsive features in elderly people, including imbalance and dysarthria43 and to a lesser reserve of dopaminergic neurons.44 More rapid progression of disease in elderly people has been noted by many others.45-49
SEX
In most parkinsonian studies men outnumber women by 1.4–3 :11 6 10 13 16 19 26 32 33 35 yet since the 1967 report of Hoehn and Yahr19 there have been repeated reports of increased mortality in women compared with men with Parkinson’s disease.13 16 32 50 Some find no difference or find a lower mortality in women.8 25 33 51 We did not find a significant difference between men and women for mortality when SMRs were compared and our increased female mortality did not reach statistical significance when compared with the general Australian female population, by contrast with the male comparison. However, within our group, the women who died did so unusually early, and at a similar age to the men. The current life expectancy of the Australian population is 75 years for men and is 81 years for women but includes all ages over 1 year.52
Conclusions
The considerable symptomatic benefit of levodopa therapy in Parkinson’s disease was not accompanied by a reduced mortality after the first few years of treatment. This applied to patients with onset in middle age as well as to elderly people. Bromocriptine did not reduce mortality when used early in the disease nor did it improve the progression of the disease when compared with levodopa therapy. Women did not have a higher mortality than men. One quarter of patients required nursing home placement, where they survived for a mean of nearly 3 years. Confusional states and hallucinations were prominent causes of placement. About 10% of patients had a benign form of Parkinson’s disease. A similar percentage of younger patients were able to work full time at 10 years. We suggest that the disease progresses at a similar rate now as it did before levodopa, with regard to the emergence of relatively non-levodopa responsive features such as imbalance, falling, dysphagia, dysarthria and dementia. Once these appear, mortality rises.
Acknowledgments
The initial drug study was funded by Sandoz Australia (now Novartis). Continued follow up of patients was funded by donations from the Hennessey Bequest, administered by the Australian Brain Foundation, and from the estate of the late Sarah Peters, administered by the Royal North Shore Hospital.
References
Linked Articles
- Editorial commentary