Article Text

Abstract
OBJECTIVE To evaluate the cost-effectiveness of interferon beta-1b (IFβ-1b) for relapsing-remitting multiple sclerosis (RRMS).
METHODS Construction of a cost-effectiveness model using published data on IFβ-1b effectiveness and the natural history of RRMS, and new data on costs and quality of life (QoL) from a sample of 102 patients with RRMS and resident in northern England.
RESULTS Poorer QoL was found for patients with multiple sclerosis compared with the general population; those who had had a relapse; those with worse states identified by a clinical measure (expanded disability status scale (EDSS)). Relapses have effects over several months. Health state valuations were higher than in the general population. Costs were higher in relapse than remission and for worse EDSS states. IFβ-1b costs were larger than cost savings. The best cost-effectiveness estimate was £28 700 per relapse avoided, which is £809 900 per QALY gained; or £328 300 per QALY gained allowing for effects of progression over 5 years. Estimates were robust to changes in assumptions.
CONCLUSIONS The impact of multiple sclerosis on QoL is substantial. Future trials should base outcomes measurement on QoL and be better linked to natural history and cost data. IFβ-1b produces important occasional short term QoL gains, but small gains in QALYs overall and large additional costs.
- costs
- quality of life
- multiple sclerosis
- interferon β
Statistics from Altmetric.com
Until recently, no specific therapy was available for multiple sclerosis. After clinical trials which established that interferon β preparations reduce multiple sclerosis disease activity,1-4 three products have been licensed in the United Kingdom—interferon β 1-b (IFβ-1b) and two interferon β 1-a (IFβ-1a) compounds. IFβ-1b is now also licensed for secondary progressive disease.5
At present, their role in clinical practice remains uncertain. The trials are not easily extrapolated to general patient populations and provide no information about quality of life effects and cost-effectiveness. The National Health Service Executive's health technology assessment programme commissioned a 1 year project to assess the cost-effectiveness of IFβ-1b (which at the time was the only licensed product) in relapsing-remitting multiple sclerosis (RRMS).6 A cost-effectiveness model was constructed using published data on effectiveness and the natural history of multiple sclerosis and new data on costs and quality of life. There is a danger that cost-effectiveness summaries may suppress important detail; we therefore examined the quality of life of people with multiple sclerosis more closely than economic appraisal strictly requires.
Methods
The cost-effectiveness of IFβ-1b compared with standard management was measured by cost-effectiveness and cost-utility ratios, defined respectively as cost per relapse avoided and cost per quality adjusted life-year (QALY) gained. This was based on the IFβ-1b trials' reported clinical outcomes.1 2 However, resource use and quality of life and utilities (the QALY adjustment weights) were not reported, requiring collection of new data and a model to link data from different sources. The new data could not directly compare patients receiving and not receiving IFβ-1b, but provided a means to generate such comparisons.
DATA COLLECTION
Two samples of people with RRMS were chosen from the catchment area of the neurology service at Newcastle-Upon-Tyne: 40 patients who had experienced a relapse in the 6 months preceding a fixed date (the “recent relapse group”); and 62 who had not (the “remission group”). Subjects were chosen as they were identified from medical records by a research nurse.
Our study only identified relapses via medical records and therefore had less detailed information than the trial. Our definition of a relapse (a new symptom or worsening of an existing one) thus differed from the trial, which did not stipulate hospital management but required evidence of new neurological abnormality. Hence, patients in our study may on average have experienced more severe relapses. Because this may lead to an overestimate of the benefits of IFβ-1b, we tested the effect of this by sensitivity analysis.
Resource use data were collected by patient questionnaire and medical records, and converted to NHS unit costs using various sources (see costs section below). Quality of life data were collected by patient questionnaire, and converted to utilities using two sources. Firstly, the EuroQoL-5 Dimension instrument, EQ-5D7 was used in the patient questionnaires (see quality of life section below), giving population based values via the measuring and valuing health (MVH) tariff developed at the University of York, UK.8 Secondly, utilities were measured directly for 50 patients, 26 from the recent relapse group and 24 from the remission group.
Linkage between multiple sclerosis natural history data, trial outcomes, and cost and quality of life data was through the expanded disability status scale (EDSS).9 As this is not routinely collected, estimates were made for those patients managed by the consultant neurologist (DB).
QUALITY OF LIFE
We reviewed available patient based measures of QoL in multiple sclerosis, opting for the multiple sclerosis quality of life 54 item scale (MSQOL).10 This measure comprises a well validated generic health status instrument, the short form (SF)3611and additional multiple sclerosis specific items. It addresses 12 QoL domains: physical and social function, roles physical and emotional, pain, energy, mental and general health, health distress, sexual function, cognitive function, and overall QoL. Composite scores for physical and mental health can be calculated. As for the SF-36, scores on the MSQOL range from 0–100, with higher scores indicating better functioning (0=worst possible, 100=best possible). MSQOL has been shown in a United States sample to have good psychometric properties10 (high internal consistency, test-retest reliability and reproducibility; evidence of construct validity). As the time frame set by the funding body did not permit a pilot study to examine the acceptability to patients of four detailed sexual function items which might offend some and so reduce response rates, we omitted them and included only the single item concerning sexual satisfaction.
To support the use of this adapted version of MSQOL, psychometric analysis using the MAP-R multitrait scaling analysis package12 was performed. This showed that MSQOL performs similarly for United Kingdom as for United States patients; and its psychometric properties were generally acceptable. Compared with United States patients, there were marked ceiling effects for two scales, role emotional and bodily pain; and marked floor effects for two scales, role physical and role emotional. Floor effects were particularly problematic for the first, suggesting that MSQOL may underestimate marked differences in level of functioning in this domain between different patient subgroups. Full details of the psychometric analysis are reported elsewhere.6
We also collected the EQ-5D,7 a generic measure with five dimensions—mobility, self care, usual activities, pain/discomfort, and anxiety/depression. The EQ-5D notation represents a composite health state denoting the level of severity in each of the five health domains. For example, 11112 means no problems with walking, self care, usual activities and pain, moderate anxiety/depression; 22222 means moderate problems across all domains. A summary quality of life score (varying between 0 and 1) can then be assigned to each state using the MVH tariff. The tariff was derived from interviews with the United Kingdom general population, which involved asking them to assign values to different health states using the time-trade off method.13
The remission group judged quality of life in remission by recording health status over time. They kept a daily quality of life diary for 6 weeks, and at the start and end of this period recorded via a structured questionnaire current MSQOL and EQ-5D status. Because we could not identify patients at the start of a relapse and monitor them, relapses were assessed retrospectively. The recent relapse group recorded in a structured questionnaire how they were currently (MSQOL and EQ-5D) and how they were at the worst of their relapse (EQ-5D). Up to two 3 weekly reminders were sent to non-responders.
UTILITIES
In face to face interviews subjects valued multiple sclerosis specific health profiles, using the time trade-off method.13 These incorporated quality of life effects, described as EQ-5D states, number of relapses, and the probability of disease progression, taken from multiple sclerosis natural history data14-17 and the IFβ-1b trial. One scenario described multiple sclerosis with no drug therapy, matching the trial outcomes for the placebo group. Another described multiple sclerosis with (unnamed) drug therapy, matching the therapy group's outcomes. A third described more severe multiple sclerosis effects without drug therapy. Subjects also valued five EQ-5D profiles likely to be encountered by patients with RRMS, which could be directly compared with the MVH values.
COSTS
Service use data for 6 months were abstracted from hospital case notes, including inpatient stays (specialty, number of admissions, and duration of stay), day cases and outpatient visits (specialty and number of visits), drugs (name, dosage, and duration), procedures and tests (type and frequency), and appliances. The patient questionnaires included questions on primary and community services, recording number of visits by professional group.
The Chartered Institute of Public Finance and Accountancy (CIPFA) database18 provided inpatient and day case unit costs. Drug costs were from the British National Formulary19; IFβ-1b costs included administration and monitoring. Procedure and test costs were from the Trust providing the patients' specialist service. Costs for appliances and community services were taken from a previous report.20
COST-EFFECTIVENESS MODELS
The IFβ-1b trial reported reduced numbers of relapses but no statistically significant effect on disability. This requires a simple model which sums over time resultant cost savings and QALY gains to compare with treatment costs.
However, because other trials may find an impact on progression, a more complex model is required which incorporates this and the natural history of multiple sclerosis. It comprises a hypothetical cohort, within which each patient is at any time at a particular EDSS level, initially EDSS 3, the average trial baseline. Progression probabilities, taken from the natural history literature, determine the levels in subsequent years; a reduced risk rate, taken from trial estimates, applies to those having therapy. Each patient's illness career is summarised as a “transition state”— for example, EDSS 3→3 (no progression), EDSS 3→5 (initially EDSS 3, finally EDSS 5), which has a particular level of costs and utility, calculated as an average for each EDSS level weighted by the time spent in it. Full details of the model are reported elsewhere.6
Relapse costs and utility losses were the difference in average cost and EQ-5D scores between remission and relapse groups. The remission group provided EDSS level costs. A utility score was calculated for each EDSS level by assigning each patient's EQ-5D state in remission a score from the MVH tariff and averaging for those at that level.
STATISTICAL ANALYSIS
Analysis of health state differences between remission and relapse patients are reported as two tailed p values using Mann-Whitney tests. Analysis of EDSS scores are reported using Kruskal-Wallis one way analysis of variance (ANOVA). All statistical tests were performed using SPSS software.
Results
Table 1 summarises demographic and clinical characteristics. Most patients were women and the average age was 42 years. Half could not work because of long term illness or disability (55% of the recent relapse group, 47% of the remission group). Eighty nine were assigned EDSS scores; 37% scored 0–3, 36% scored 4–5, 27% scored 6 or more; the remaining 13 patients' notes could not be obtained in the time in which data were collected. Except for employment status, the utilities subsample had similar sociodemographic and clinical characteristics compared with the whole sample.
Demographic and clinical characteristics of participants in a survey of people with relapsing-remitting multiple sclerosis
QUALITY OF LIFE
Table 2 shows MSQOL scores for remission and relapse groups. Scores were significantly different (p<0.001) for physical function, role physical, and social function scales, the change in health item, and the physical health composite. As we do not reproduce MSQOL here, it may aid interpretation to know that for physical function, lower scores represent reduced ability to perform a range of gentle through to vigorous physical activities; for role physical, lower scores indicate problems in carrying out work and other regular daily activities; and for social function, lower scores indicate problems in carrying out normal social activities with family and friends. Scores for emotional problems, mental health, cognitive function, and general health perceptions showed least differences. Table 3 reports MSQOL scores for EDSS subgroups. There was a highly significant trend in physical function scores, from 54.2 with an EDSS score ⩽3 to 12.6 with a score ⩾6 (p<0.0001). There were also significant differences for social and sexual function (p<0.01) and role physical and health distress (p=0.01). There were small but significant differences for both composite scores.
MSQOL mean scores for patients in remission and recently relapsing in a survey of people with relapsing-remitting multiple sclerosis
MSQOL mean scores by expanded disability status scale (EDSS) scores in a survey of people with relapsing-remitting multiple sclerosis
Subjects had markedly lower SF-36 scores than a “normative” United Kingdom general population.21 For example, they scored 45 points lower on the physical function scale and 43 lower on the role physical scale than the general population with long standing illnesses; and 59 and 62 respectively lower than those without. Differences were smaller but none the less considerable for social function, energy, and general health.
Ninety six respondents completed all five EQ-5D statements. Only 5% were currently in state 11111, compared with 57% of a general population.22 Only 27 out of a possible 243 states were found; 31 patients reported problems with mobility and 32 problems with performing usual activities. The recent relapse group had worse mobility, self care, and pain than the remission group but similar anxiety and depression levels. The recent relapse group's profile was significantly poorer in all domains during relapse than currently.
HEALTH STATE UTILITIES AND PREFERENCES
Table 4 shows mean utility scores. The IFβ-1b and placebo scenario scores were very similar, but the severe scenario scored much lower. Compared with the MVH study, the EQ-5D scores were consistently higher, with greater differences among more severe states.
Utility values of disease specific scenarios and EQ-5D states from participants in a survey of people with relapsing-remitting multiple sclerosis
The results enabled conversion of EDSS scores into utilities. The MVH values were applied to each patient's EQ-5D state, from which the mean value for each studied EDSS level was calculated: 0.71 for EDSS 3, 0.66 for EDSS 4, 0.52 for EDSS 5, 0.49 for EDSS 6, and 0.35 for EDSS 7. Similarly, the utility loss from relapse was calculated by averaging over subjects the MVH values for each EQ-5D state in remission and relapse, and taking the difference: average remission value=0.604; average relapse value=0.136; a net loss of 0.468 per relapse.
COSTS
Average costs were £529 in the remission group and £2644 in the recent relapse group, giving relapse costs of £2115 per patient. The difference was mainly related to use of inpatient and day case and, to a lesser extent, community services, with no difference in outpatient visits, drugs, tests, and appliances. Higher resource use was associated with higher EDSS scores.
COST-EFFECTIVENESS AND COST-UTILITY ANALYSIS
Table 5 summarises results obtained from the models, showing costs, benefits, and cost-effectiveness and cost-utility ratios (rounded to the nearest £100). The results including only the effect of relapses are presented with and without discounting at the United Kingdom Government recommended rate of 6%, although discounting makes little difference. IFβ-1b reduced relapses by 1.52 per patient over 5 years, but had discounted net costs of £43 600, giving a cost-effectiveness ratio of £28 700 per relapse avoided. There was a gain of 0.054 discounted QALYs, giving a cost-utility ratio of £809 900 per QALY gained.
Cost, quality adjusted life-year, and cost effectiveness estimates from different models
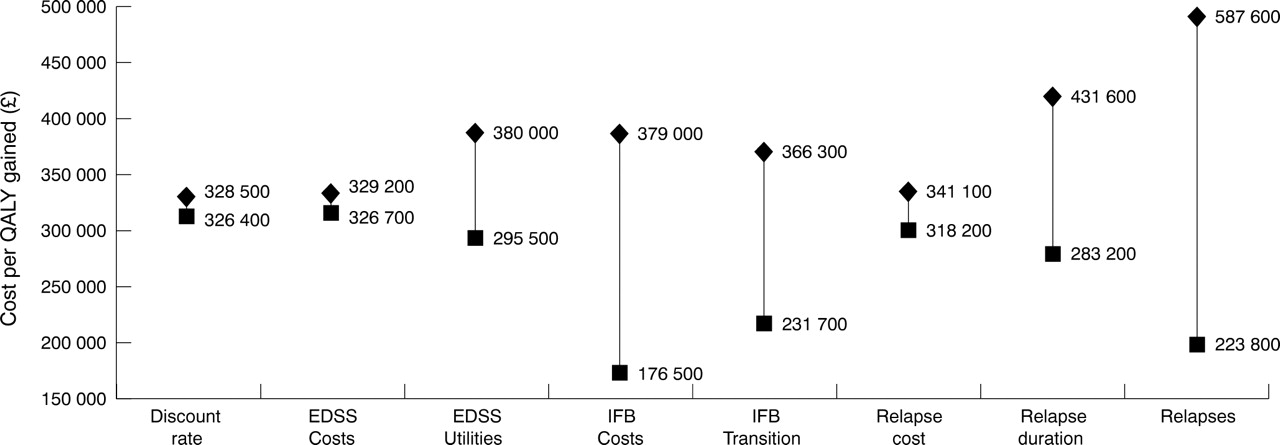
The more complex models, incorporating progression changes, are presented only in discounted form. For a five year model, 0.13 QALYs were gained at a cost of £43 400, giving £328 300 per QALY gained. The robustness of this was tested using one way sensitivity analyses. The figure shows that varying the assumptions for a range of variables produced no important changes in the cost-utility ratio. The largest change was related to the frequency of relapses.

{kind=link}
Sensitivity analysis of 5 year model. Base case and lower and upper estimates are: discount rate 6% (0–10); EDSS costs per year: EDSS 3 £740 (£370-£1480), EDSS 4 £850 (£425-£1700), EDSS 5 £1570 (£785-£3140), EDSS 6 £1590 (£795-£3180); EDSS utilities: EDSS 3 0.71 (0.65–0.79), EDSS 4 0.66 (0.59–0.74), EDSS 5 0.52 (0.41–0.67), EDSS 6 0.49 (0.38–0.63); IFb-1b costs per year £10 500 (£6000 - £12 000); IFb-1b transition probabilities: EDSS 3→4 0.12 (0.20–0.10), EDSS 3→5 0.06 (0.10–0.05), EDSS 3→6 0.22 (0.10–0.25); Relapse cost £2115 (£1000–£3000); Relapse duration in weeks 4 (2–6); utility loss per relapse 0.5 (0.25–0.75); Number of relapses with IFb-1b 3.71 (2.5–5).
A 10 year model, which uses more assumptions and has greater uncertainty, produced similar results using base case assumptions, and was examined further by altering the assumptions to favourable (“best case”) assumptions about progression and IFβ-1b effectiveness and unfavourable (“worst case”) assumptions, equivalent to “no impact on progression”. The best case gave £74 500 per QALY gained compared with base case and worst case values of £228 300 and £604 600 respectively (table 5).
Discussion and conclusions
IFβ-1b produces important occasional short term quality of life gains, but because they are infrequent they translate into small QALY gains. Even optimistic estimates of longer term gains from delayed progression produce small aggregate QALY gains because few benefit. With large net costs, IFβ-1b has a high cost per QALY gained.
It is difficult to compare these results with other studies as, to our knowledge, no previous economic evaluation of interferon β therapy has been undertaken using similar methods. A Canadian study calculated comparable cost per relapse avoided ratios of between Can$48 000-Can$67 000.23 However, no attempt was made to translate these effects into QALYs.
This study required many assumptions to construct an economic evaluation from clinical trials designed for a different purpose. Key instruments for data collection were developed rapidly, some data were collected retrospectively, and data collection was not planned to usual statistical specifications. However, the assumptions are evidence based, plausible, and robust to testing. The data instruments performed well and the results seem conclusive within a large margin of uncertainty.
Extensive sensitivity analysis was conducted to ensure that the results could be generalisable to a wide patient population. This was particularly important as our study sample exhibited some clinical differences from the drug trial population with respect to EDSS levels and the measurement of relapses. In addition, we made no attempt to value indirect costs, such as time lost from work and other activities for patients and carers. Although these are likely to have important implications for the level of costs associated with EDSS scores and relapses, we have shown that different values make little difference to the cost/QALY gain ratio (figure and table 5).
Summary effectiveness measures such as relapse rates or EDSS progression may mask important quantifiable effects of multiple sclerosis on quality of life. Measures of QoL are consistent with EDSS scores, which is important as they are widely used by clinicians, but provide important additional information. The outcome measure of choice in evaluations of therapies for multiple sclerosis should therefore be changes in QoL. Such studies must also link outcomes with direct and indirect costs, which has implications for trial design.
These results should help those making prescribing and policy decisions at different levels. Patients and clinicians might consider the extent of the quality of life gains produced by IFβ-1b compared with alternatives for improving health. Third party payers have also to consider potential health gains for people with other conditions which could result from alternative uses of IFβ-1b expenditure, bearing in mind both efficiency, as indicated by the cost-utility figures, and also equity.
Acknowledgments
This project was funded by the NHS Health Technology Assessment programme, project number 95/01/2. The views and opinions expressed do not necessarily reflect those of the Department of Health. The following were members of the team that carried out the study at the University of Newcastle Upon Tyne: Ms Julie Doughty, junior research associate, Centre for Health Services Research; Sister Joanna Forsyth, staff nurse, Department of Clinical Neurology; Mrs Sylvia Hudson, project secretary, Centre for Health Services Research. We are grateful to the people who gave their time to take part in our surveys, to Paul Dolan and Karen Gerard for help with the valuation exercise, to Pippa Anderson for access to psychometric analysis software, and to referees of our report to the HTA for their helpful comments.