Article Text

Abstract
OBJECTIVES To investigate the pathophysiology of selective absence of F waves and its relation with antiganglioside antibodies in Guillain-Barré syndrome (GBS). Some patients with GBS show the absence of F waves as an isolated conduction abnormality, which has been interpreted as demyelination in the proximal nerve segments.
METHODS In 62 consecutive patients with GBS, sequential nerve conduction and F wave studies were reviewed, and antibodies against ganglioside GM1, GM1b, GD1a, GalNAc-GD1a, GD1b, and GQ1b were measured by an enzyme linked immunosorbent assay.
RESULTS In the first electrophysiological studies, isolated absence of F waves was found in 12 (19%) patients. Sequential studies in 10 of these patients showed two electrophysiological sequel patterns; rapid restoration of F waves (six patients), and persistent absence of F waves with distal motor nerve degeneration (acute motor axonal neuropathy, four patients). None of the 10 patients showed evidence of demyelination in the proximal, intermediate, or distal nerve segments throughout the course. Of the 62 patients, IgG antibodies against GM1, GM1b, GalNAc-GD1a, or GD1b were significantly associated with the electrodiagnosis of acute motor axonal neuropathy, and patients with these antibodies more often had isolated absence of F waves than patients without them (11 of 36 (31%)v one of 26 (4%);p<0.01). Eleven of the 12 patients with isolated absence of F waves had positive serology for one or more antiganglioside antibodies.
CONCLUSIONS In GBS with antiganglioside antibodies, isolated absence of F waves is a frequent conduction abnormality especially in the early phase of the disease, and may be caused by axonal dysfunction, such as physiological conduction block or axonal degeneration at the nerve roots.
- Guillain-Barré syndrome
- F wave
- antiganglioside antibody
Statistics from Altmetric.com
In Guillain-Barré syndrome (GBS), electrophysiological evidence of nerve dysfunction may be more prominent in the proximal portions of the peripheral nerves.1-3 Peripheral nerve conduction studies are normal in 10% to 20% of patients,4-6 and the absence or slowing of F waves may be an isolated conduction abnormality, especially in the early stage of illness.3 7 8 The value of F wave studies in GBS therefore is well established.
The absence of F waves has been interpreted as demyelinative conduction block in the proximal nerve segments when distal compound muscle action potentials (CMAPs) are preserved.2 6 8 Other mechanisms, however, could contribute to the blocking of F wave generation in GBS: Firstly, axonal degeneration in the proximal portions results in the selective disappearance of F waves before distal nerve segments undergo wallerian degeneration. Secondly, physiological conduction failure at the nodes of Ranvier, proposed as a possible mechanism in the axonal subtype of GBS,9 may cause proximal conduction block. Thirdly, impaired excitability of the motor neuron or proximal axon has recently been proposed to be the major pathophysiology of F wave disappearance.10 Sequential F wave and nerve conduction studies are useful for clarifying the pathophysiology of absence of F waves because demyelinative or axonal conduction abnormalities may develop later in the distal or intermediate nerve segments, and resolution of demyelinative conduction block is associated with remyelinating slow components, as shown by prolonged minimum latencies or chronodispersion of F waves.
In the early 1990s, an axonal variant of GBS, named acute motor axonal neuropathy (AMAN), was recognised in northern China11 and is now known to occur in other countries.12 13 This subgroup of GBS is often associated with anti-GM1 antibody. The pathophysiological role of antiganglioside antibodies in GBS has not been established, but anti-GM1 antibody is reported to block nerve conduction14 and to affect nodal function in vitro.15 If humoral factors such as autoantibodies function in AMAN, the nerve roots, where the blood-nerve barrier is anatomically deficient,16 may be preferentially affected, as in classic demyelinating GBS.17 To investigate the pathophysiology of absence of F waves and its relation with antiganglioside antibodies in GBS, we reviewed sequential electrodiagnostic studies and measured antiganglioside antibodies.
Patients and methods
PATIENTS
Sixty two consecutive patients with GBS who were seen at Chiba University Hospital or its affiliated hospitals between January 1992 and April 1998, were studied. They fulfilled the clinical criteria for GBS,18 and the first electrophysiological studies were done within 16 days of onset of the neurological symptoms. Their mean age was 38 years (range 3 to 78 years).
ELECTROPHYSIOLOGY
Nerve conduction studies were done using conventional procedures and a Nicolet Viking IV EMG machine. Motor conduction studies were done in the median, ulnar, tibial, and peroneal nerves. In the median and ulnar nerve studies, the axilla was also stimulated. For the median and ulnar nerves, F waves were elicited after wrist stimulation, and for the tibial nerve after ankle stimulation after 32 consecutive supramaximal stimulations delivered at the rate of 1 Hz. Peroneal F waves were not analysed because there is relatively frequent absence of responses in normal subjects.19 During the F wave studies, patients lay on a bed and were asked not to fall asleep. Only deflections larger than 50 μV were accepted, to differentiate F waves from background noise.
Acute motor axonal neuropathy or acute inflammatory demyelinating polyneuropathy (AIDP) was diagnosed based on the electrodiagnostic criteria of Ho et al.20 When there was prolongation of motor distal latency (>10% of upper limit of normal) or slowed conduction velocity (<90% of lower limit of normal) in two or more nerves, patients were classified as having AIDP. When patients had a decrease in amplitude of distal compound muscle action potentials (<80% of lower limit of normal) and no evidence of demyelination as defined above, they were classified as having AMAN. When the AMAN pattern and amplitude reduction of the sensory nerve action potentials (<80% of the lower limits of normal) were present, patients were classified as having acute motor and sensory axonal neuropathy (AMSAN).21
ANTIGANGLIOSIDE ANTIBODY ASSAYS
Serum samples obtained from patients in the first 4 weeks of illness were stored at –80°C until used. IgG and IgM class antibodies to gangliosides GM1, GM1b, GM2, GD1a, GalNAc-GD1a, GD1b, GT1b, and GQ1b were measured by enzyme linked immunosorbent assay (ELISA) as described elsewhere,22 by one of the authors (MK) who was blind to the clinical and electrophysiological data. Antibody titre (1:x) was the highest serum dilution at which the optical density at 492 nm was 0.1 or more. Serum was considered positive when the titre was 1:500 or more.
Results
ELECTRODIAGNOSIS
The mean time from the onset of neurological symptoms to the first electrophysiological study was 8.4 days (range 2 to 16 days). By electrodiagnostic criteria, patients were classified as having AIDP (n =24), AMAN (n =18), or AMSAN (n=2) based on their peripheral conduction abnormalities. Of the remaining 18 patients, 12 showed the absence of, or markedly decreased (persistence<20%), F waves in two or more nerves with normal peripheral conduction, and six had only mild prolongation of distal motor latencies. Absence of F waves, therefore, was an isolated abnormality in 12 (19%) patients in the first nerve conduction studies.
ELECTROPHYSIOLOGICAL SEQUEL OF ISOLATED ABSENCE OF F WAVES
The 12 patients with isolated absence of F waves had the first electrophysiological study at a mean of 6.9 days (range 2 to 11 days) after the onset of neurological symptoms. Ten of them underwent three to six nerve conduction and F wave studies during the first 3 months. Sequential studies showed two electrophysiological sequel patterns (table 1). Six patients (1–6) had the rapid restoration of F waves 5 to 13 days after the first examination. When F waves appeared, there was no prolongation of F wave latency or F chronodispersion in any of them (fig 1). These six developed no conduction abnormalities in the intermediate and distal nerve segments throughout the course of the illness. Four patients (7–10) had the AMAN pattern in the second studies carried out 5 to 7 days later. Distal CMAPs were low but conduction velocities and distal latencies were normal. Amplitudes of CMAP were low for up to 3 months after onset. Sequential data of F wave persistence and distal CMAP amplitude are shown in fig 2.
Electrophysiological sequel and antiganglioside antibodies in GBS patients with isolated F wave absence

F waves in the median nerve studies of patient 2. F waves are markedly decreased in the first study (day 4), but seem normal in the second (day 14). 500 μV/division for F waves.
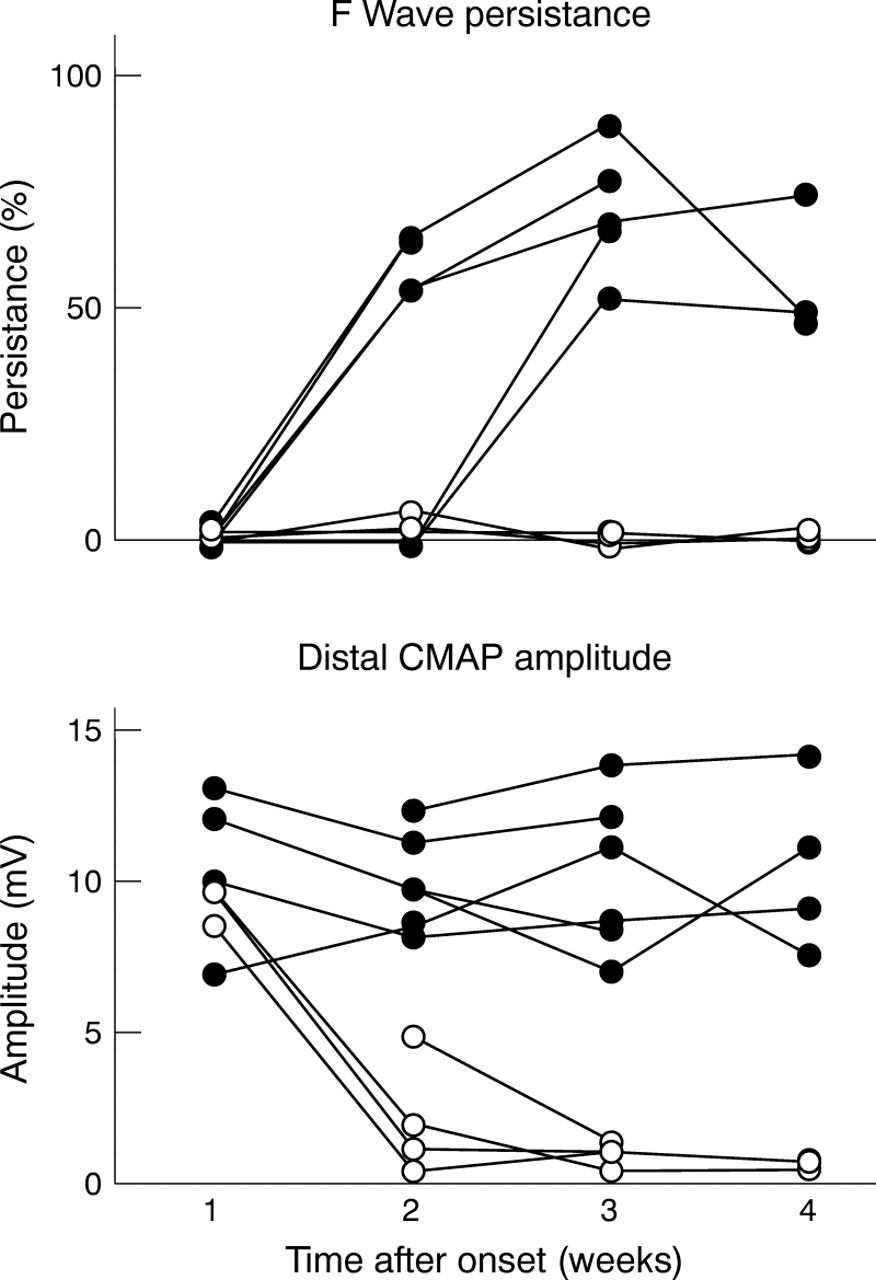
Sequential data of F wave persistence and amplitude of compound muscle action potential (CMAP) in the median nerves of patients who showed isolated absence of F waves in the first studies. In patients with rapid restoration of F waves (filled circles, patients 1–6 in table 1), distal CMAPs remained normal throughout the course. By contrast, the other patients (open circles, patients 7–10) had marked reduction of CMAPs suggesting an acute motor axonal neuropathy pattern.
EFFECTS OF VOLUNTARY CONTRACTION ON F WAVE PERSISTENCIES
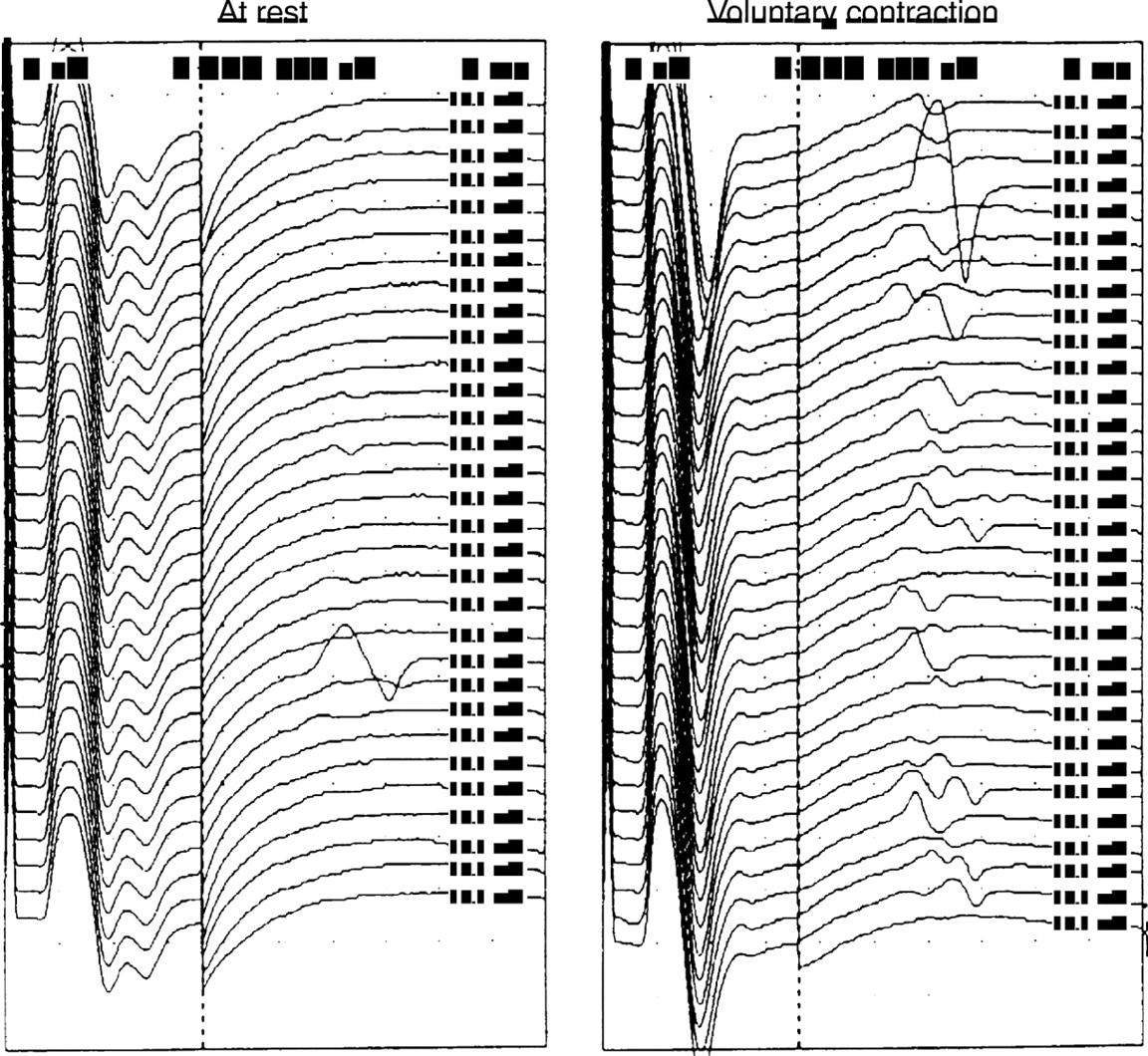
The F waves were also recorded in four patients with isolated absence of F waves during voluntary contraction in the first studies (table 2). Patients were asked to maintain thumb abduction in the median nerve studies. This manoeuvre increased F persistencies in two (fig 3) of the four patients.
The effect of voluntary contraction of F wave persistence (median nerve)
{kind=link}
{kind=link}
{kind=link}
Effect of voluntary contraction on median F wave persistence in patient 5. Voluntary contraction of the abductor pollicis brevis increased F wave persistence. Muscle strength is 3 on the MRC scale. 500 μV/division for F waves.
CLINICAL FEATURES OF PATIENTS WITH ISOLATED ABSENCE OF F WAVES
Ten of the 12 patients had preceding upper respiratory tract infection (table 3). Cranial nerve involvement was found for eight patients (ocular motor in four; facial in four). None of them had sensory loss, but 3 (4, 7, and 12) had mild paraesthesia in the distal limbs. In the four patients who had anti-GQ1b antibodies (4, 5, 6, and 10), ophthalmoplegia was the initial sign, descending paralysis developing later. Both the disabilities at the peak of the disease and the recoveries varied. Clinical recovery in the patients with rapid F wave restoration (1–6) was especially good, all being able to run 3 months after onset. Four patients with AMAN (7–10) had delayed recoveries and mild to moderate atrophy of the distal muscles.
Clinical features of patients with isolated F wave absence
ANTIGANGLIOSIDE ANTIBODIES
Positive IgG antibodies were found against gangliosides GM1 (n=26, 42%), GM1b (n=23, 37%), GD1a (n=20, 32%), GalNAc-GD1a (n=11, 18%), GD1b (n=13, 21%), and GQ1b (n=6, 10%), and IgM antibodies were found against GM1 (n=11, 18%), GM1b (n=6, 10%), GD1a (n=4, 6%), GalNAc-GD1a (n=10, 16%), GD1b (n=2, 3%), and GQ1b (n=3, 5%). Thirty six (58%) patients had one or more IgG antibodies. IgG antibodies against GM1 (p<0.01), anti-GM1b (p<0.01), anti-GalNAc-GD1a (p<0.05), and anti-GD1b (p<0.05) were significantly associated with the AMAN electrodiagnosis. The other antibodies tested had no correlation with electrodiagnosis. Table 1 shows results of antiganglioside assays in the 12 patients with isolated absence of F waves. Eleven of them had positive antiganglioside antibodies, although the remaining one was negative for all the antibodies. Of the 62 patients, isolated absence of F waves was more often found in patients with antibodies against GM1, GM1b, GalNAc-GD1a, or GD1b, which had association with AMAN (11 of 36, 31%), than in patients without these antibodies (one of 26, 4%) (p<0.01).
ABNORMALITIES IN F WAVES IN PATIENTS WITH AIDP OR AMAN/AMSAN
Sixteen of the 20 patients with AMAN/AMSAN and all 24 patients with AIDP showed the absence of or decreased F waves, or prolonged minimum latencies in two or more nerves, the F wave studies showing abnormalities in 52 of 62 (84%) patients in the first studies. In the recovery phase (weeks 5 to 7), 20 patients with AIDP had prolonged minimum latencies above 125% of the normal limits in two or more nerves, and 11 patients with AIDP had F chronodispersion (>6.6 ms for the median and ulnar nerves, and >9.6 ms for the tibial nerve23).
Discussion
Our findings show that 12 (19%) of 62 patients with GBS had an absence of F waves but normal peripheral nerve conduction in the first examination. The incidence is consistent with previous findings: Ropperet al 6 reported that of 113 consecutive patients with GBS, isolated absence of F waves or a decrease, which they termed “selective proximal block”, was present in 27% and was the most common early finding. Kiers et al 8 reported 10% of 241 GBS nerves as having an absence of F waves with preserved distal CMAPs.
None of our patients with selective absence of F waves showed evidence of peripheral nerve demyelination. This may be due in part to geographical differences among the countries in the ratios of GBS subgroups. The AMAN pattern is much more frequent in China11 20 than in western countries, where most GBS is AIDP. The incidences of anti-GM1 antibodies are reported to be 43% in China20 and 10%-25% in western countries.21 24-26 Our Japanese series showed an incidence of 34% for the AMAN/AMSAN pattern and 42% for the anti-GM1 positivity. Because the higher ratio of antiganglioside positive patients in our series may have affected the results, discussion is limited to the antiganglioside positive subgroup of GBS.
Our study showed two electrophysiological sequel patterns; rapid restoration of F waves (six patients) and persistent absence of F waves associated with axonal degeneration (four patients). As stated in the introduction, at least four mechanisms account for the selective blockage of F wave generation in GBS; demyelination, axonal degeneration, physiological conduction failure, and impaired excitability. Physiological conduction failure is proposed as the mechanism for AMAN.9 27 Rapid clinical recovery,10 quick resolution of distal conduction block,28 and minimal pathological changes despite the profound paralysis27 29 of some patients with AMAN suggest early reversible conduction failure at the nodes of Ranvier. This axonal dysfunction may produce proximal conduction block. Impaired excitability has recently been proposed as the mechanism of F wave disappearance by Yokota et al.10 They demonstrated that in some patients with GBS who lack F waves, magnetic brain stimulation elicited enough CMAPs to generate F waves, and concluded that the major pathophysiology of F wave disappearance is not conduction block, but decreased excitability of the motor neuron or proximal axon.
Our patients with isolated absence of F waves followed by rapid restoration were characterised by early reversible and selective involvement of the nerve roots. We speculate that this conduction abnormality results from physiological conduction block or decreased motor neuron excitability. Demyelination is unlikely because the restoration seemed too rapid for developing remyelination, and because remyelinating slowly conducting components were absent in the recovery phase, although the possibility of mild demyelination restricted to the paranode could not be excluded. Resolution of demyelinative conduction block usually begins with remyelinating slow components,30 31 as indicated by prolonged latencies or the chronodispersion of F waves, and our antiganglioside negative patients with AIDP actually showed this recovery pattern. Because voluntary contraction of the tested muscles increased F wave persistency, impaired motor neuron excitability probably contributed to the blocking of F wave generation in some cases. The apparent weakness of the tested small hand muscles (table 2), despite normal conduction in the nerves distal to the axilla, however, indicated the presence of conduction block between the axilla and spinal cord. We speculate that in this patient group, the F wave disappearance is caused by the cumulative effects of both phenomena—physiological conduction block and decreased motoneuron excitability.
In the patients who showed isolated absence of F waves and later developed AMAN, axonal damage at the level of the nerve roots may have been responsible for the disappearance of the F waves. Although newly developed lesions in the distal motor nerves or wallerian degeneration after radicular axonal damage could cause axonal loss, we consider the first more likely in some cases because distal axonal loss occurred too early to allow wallerian degeneration after root lesion (intervals between the first and second studies were 3 to 7 days, mean 4.3 days). In human wallerian degeneration, loss of CMAPs requires several days even in axonotomy, and longer distal stumps show a later loss of CMAP amplitude.32 The sequential findings may be explained by axonal degeneration that occurs initially in the nerve roots and somewhat later in the motor nerve terminals, both regions being preferentially affected in GBS. This is consistent with the null effect of voluntary contraction on F wave persistence in this group of patients (table 2).
Isolated absence of F waves during the early phase of GBS with antiganglioside antibodies suggests axonal conduction abnormalities such as early reversible physiological conduction block or axonal degeneration of the motor nerve roots. Motor neuron excitability may affect F wave persistencies in some cases. Patients with isolated absence of F waves often had IgG antibodies to GM1, GM1b, GalNAc-GD1a, or GD1b, which were correlated with the electrodiagnosis of AMAN. These antibodies may have a pathophysiological role in the blockage of F wave generation as well as axonal degeneration. In both physiological conduction failure and axonal degeneration, the axolemma of motor fibres is probably the target of immune attack in GBS with the anti-ganglioside antibodies.