Article Text

Abstract
Although syringomyelia has been associated with Horner's syndrome, it is typically associated with other neurological findings such as upper limb weakness or numbness. A patient is described who had an isolated Horner's syndrome as the only manifestation of syringomyelia. A 76 year old woman was discovered to have right upper lid ptosis and right pupillary miosis. Neurological examination was unremarkable, and pharmacological testing was consistent with localisation of the lesion to a first or second order sympathetic neuron. Neuroimaging disclosed a Chiari I malformation with a syrinx extending to the C2 to C4 level. An isolated Horner's syndrome may be the presenting manifestation of syringomyelia.
Statistics from Altmetric.com
Chiari I malformation is characterised by caudal descent of the cerebellar tonsils into the cervical spine and is associated with syringomyelia in 20% to 30% of cases.1 Horner's syndrome, in association with upper limb weakness or anaesthesia to pain and temperature, is a well recognised finding in patients with syringomyelia. Horner's syndrome has been reported in 4% to 6% of patients undergoing surgical decompression for Chiari I malformation.2-4However, an isolated Horner's syndrome as a presenting manifestation of a Chiari I malformation in association with syringomyelia seems uncommon. We report on a woman with an isolated unilateral Horner's syndrome who was found to have a Chiari I malformation and syringomyelia.
Case report
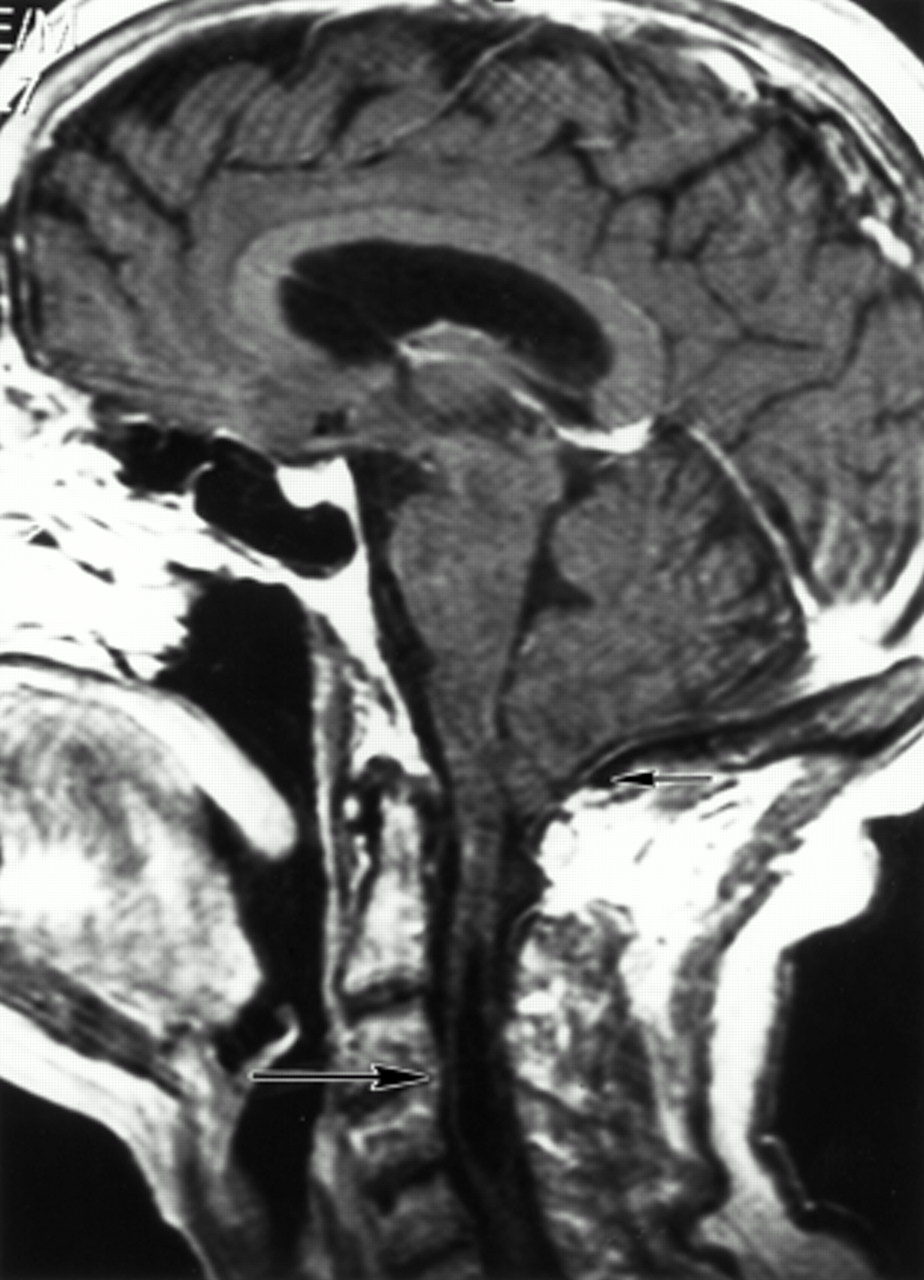
A 76 year old woman was noted by her ophthalmologist to have anisocoria and a droopy right eyelid. Over the previous 2 months, she had experienced intermittent occipital headaches in the morning, lasting 2 hours, and remitting spontaneously. She had 2 mm of ptosis in the right eye and 1 mm of anisocoria with the right pupil being smaller than the left. Her anisocoria increased in the dark, and she had pupillary dilation lag in the right eye. The remainder of her neuro-ophthalmological examination was unremarkable. Neurological examination was otherwise unremarkable with no upper limb weakness or numbness. After the instillation of 1% hydroxyamphetamine in both eyes, both pupils dilated, consistent with an intact third order sympathetic neuron. A chest radiograph with apical views disclosed no masses. Brain and upper cervical spinal cord MRI disclosed a Chiari I malformation with a syrinx extending to the C2 to C4 level (figure).
Discussion
Our patient had oculosympathetic dysfunction, localising pharmacologically to a first or second order sympathetic neuron, with no other neurological findings suggestive of a Chiari I malformation or syringomyelia. Unilateral Horner's syndrome, alternating Horner's syndrome, and alternating oculosympathetic spasm have all been seen in patients with syringomyelia, along with other typical findings of upper limb weakness and atrophy as well as anaesthesia to pinprick and temperature.5-7 In many of these cases, syrinx formation was a late sequelae of cervical cord trauma. Pupillomotor fibres coursing in the peripheral portion of the anterolateral cervical spinal cord are presumably interrupted by the syrinx, causing hypoactivity or hyperactivity of the second order neurons in the interomediolateral cell column at the C8 to T2 level.2 Stovneret al studied 15 patients with Chiari I malformations using pupillometry after sympathomimetic eyedrop stimulation.8 Although no patients had Horner's syndrome, two of four patients with an associated syrinx had a Horner-like pupillary reaction, characterised by greater dilation of the eye ipsilateral to hand wasting.
{kind=link}
Postgadolinium T1 weighted MRI of the brain and upper cervical cord showing extension of the cerebellar tonsils below the foramen magnum (small arrow) consistent with a Chiari I malformation. A syrinx is present in the upper cervical cord (large arrow).
In the past, suspicion of the presence of a syrinx based on neurological examination was confirmed by a myelogram or findings at the time of surgical decompression of a Chiari malformation. Before the development of MRI, the association of an isolated Horner's syndrome with syringomyelia would not have been recognised as such patients would not have undergone the invasive testing required to make the diagnosis. We recommend that all patients with isolated Horner's syndrome localising to a first or second order neuron lesion undergo MRI of the brain, brainstem, and cervical cord to screen for structural lesions such as Chiari I malformation with syringomyelia.
Acknowledgments
This work was supported by a grant from the Heed Foundation (JBK) and as part of an unrestricted grant to Emory Eye Center, Emory University School of Medicine, from Research to Prevent Blindness, New York, NY, USA, and National Institute of Health CORE grant No P30-EYO 6360.
Linked Articles
- Editorial commentary