Article Text

Abstract
OBJECTIVES To determine the prognosis in patients with Lambert-Eaton myasthenic syndrome (LEMS) without small cell lung cancer (SCLC), and to analyse longitudinal clinical, electrophysiological, and immunological data on each patient to establish prognostic factors for long term outcome.
METHODS The retrospective and part prospective study of 47 patients with LEMS was undertaken from data recorded during visits to a specialist neuromuscular clinic. Serial measurements of muscle strength score in shoulder abduction, elbow extension and hip flexion, compound muscle action potential (CMAP) amplitude, and postcontraction increment in abductor digiti minimi (ADM), and anti-P/Q-type voltage gated calcium channel (VGCC) antibody titre were made at each visit.
RESULTS Muscle strength scores were improved in 88% of patients after a median duration of immunosuppressive treatment of 6 years (range 1.3 to 17 years); anti-VGCC antibody titres fell in 52% after treatment; and mean resting CMAP amplitude improved from 2.7 mV initially to 8.8 mV after 2 years of treatment p<0.001). Initial pretreatment anti-VGCC antibody titre did not correlate significantly with either CMAP amplitude, CMAP increment, or clinical score: from serial measurements made during follow up, significant correlation between antibody titre and CMAP amplitude was seen in only two patients. Sustained clinical remission was achieved by 20 (43%) of whom only four remained in remission without the need for immunosuppression. Using a Cox proportional hazards model, the only independent predictor of sustained clinical remission was initial pretreatment clinical score (p=0.03). Lymphoma presented in three patients during the study.
CONCLUSIONS The prognosis in patients with LEMS without SCLC is favourable, although patients often need significant doses of immunosuppressive treatment to remain clinically stable. Only initial clinical muscle strength measurements and not anti-VGCC antibody titres or electrophysiological recordings are predictive of long term outcome.
- Lambert-Eaton myasthenic syndrome
- prognosis
Statistics from Altmetric.com
Lambert-Eaton myasthenic syndrome (LEMS) is a presynaptic disorder of neuromuscular transmission characterised by impaired quantal release of acetylcholine that causes proximal weakness, depressed tendon reflexes, and post-tetanic potentiation; additionally, autonomic changes are present.1 2 About 60% of patients have a small cell lung cancer (SCLC).3 Evidence that it is an autoimmune disease mediated by antibodies to voltage gated calcium channels (VGCCs) at motor nerve terminals includes the clinical response to plasma exchange,4 the passive transfer of the pathophysiological and morphological changes to mice by injection of patients' immunoglobulins,4-7 and the detection by radioimmunoassay of serum antibodies in patients with LEMS to P/Q-type VGCCs.8 9 The antigenic stimulus for anti-VGCC autoantibody production in patients with SCLC-LEMS seems to be tumour VGCCs10; the trigger for the production of anti-VGCC antibodies in patients with LEMS with no detectable lung cancer (non-SCLC-LEMS) is unknown.
Prognosis in autoimmune diseases is variable. Most chronic autoimmune diseases are associated with reduced life expectancy.11 In myasthenia gravis, spontaneous long lasting remissions can occur in up to 20% of patients, and, after surgical and immunosuppressive treatment, at least 70% of patients are well or have only minimal restrictions 3 to 5 years after disease onset.12
There have been no long term follow up studies of patients with non-SCLC-LEMS although mortality statistics are available on patients with SCLC-LEMS.3 13 14 We therefore undertook a prospective study of patients with non-SCLC-LEMS seen from September 1996 to October 1998, and combined this with a retrospective study of similar patients seen before that date.
Methods
PATIENTS
We analysed the case records of 47 consecutive patients with LEMS without clinical or radiological evidence of SCLC seen in Oxford by one of us (JN-D) between December 1987 and October 1998. The diagnosis was based on typical clinical features and the presence of either characteristic EMG changes or raised VGCC titres. The EMG criteria comprised a reduced compound muscle action potential (CMAP) amplitude in abductor digiti minimi (ADM) (<8.5 mV)15 16; and a CMAP amplitude increment of more than 100% after 10 seconds maximal voluntary contraction. Serum VGCC antibody concentrations were significantly raised in 86%. A further 15 patients with LEMS with SCLC were also seen during the study period, but have been reported elsewhere14 and were excluded from the present study.
CLINICAL SCORES
Sequential muscle scores were calculated by summing the Medical Research Council (MRC) graded strength measurements in shoulder abduction, elbow extension, and hip flexion bilaterally made during clinic visits. An additional score of 0, 1, or 2 was added to this muscle score depending on whether the patient had swallowing problems with aspiration, swallowing problems without aspiration, or normal swallowing respectively to give a combined total clinical score of 32. Clinical remission was assigned to patients in whom, for at least 6 months, symptoms were either absent or sufficiently mild or infrequent as not to hinder normal physical activity, and whose clinical scores were greater than 30.
VOLTAGE GATED CALCIUM CHANNEL ANTIBODY ASSAYS
Patients' serum samples stored in our laboratory were assayed using 125I-ω-conotoxin MVIIC (ω-CmTx) to label P/Q-type VGCCs in extracts of human cerebellum as described previously.8 17 Assays on individual patients were performed in the same batch to allow titres to be compared. Each measurement was the mean of at least two estimations.
Final treatment details at death or final follow up
Longitudinal analysis of antibody titres was performed in nine patients in whom at least seven serum samples were obtained at the same time as measurements of CMAP amplitude and combined clinical score over a minimum period of 6 years. Serum samples were also assayed for anti-VGCC antibodies on samples taken before treatment and at final follow up in 23 patients. The minimum interval between samples was 2 years and the median interval was 6 years.
ELECTROPHYSIOLOGICAL MEASUREMENTS
These studies were performed in Oxford on all except eight patients, who had initial or follow up measurements made elsewhere. The peak to peak CMAP amplitude was recorded from the ADM using standard surface bipolar stimulating electrodes over the ulnar nerve at the wrist and Ag/AgCl recording electrodes on the belly and tendon of the muscle. All EMG measurements used to study correlation between clinical, electrophysiological, and immunological measurements were recorded within 24 hours of measuring clinical score and of obtaining serum samples for VGCC antibody assay.
STATISTICAL ANALYSIS
Student's t test was used to compare means of data sets that approximated to a gaussian distribution. Remission free survival rates were obtained using log rank tests from Kaplan-Meier survival curves. Between and within patient non-parametric (Spearman) correlation was made between clinical score, ADM amplitude, and increment, and VGCC antibody titre. Predictors of long term outcome from clinical and laboratory data were determined using Cox proportional hazards analysis.
Results
PATIENT CHARACTERISTICS
The median duration of follow up from disease onset was 10.5 years (mean 11.8 years, range 2.3 to 36 years). Mean age at onset was 47 years (median 54 years; range 11 to 74 years). The sex ratio was equal (M:F=24:23). Only 11% of the patients were regular smokers; 55% had never smoked.
TREATMENT
Forty four patients (94%) were first treated with prednisolone, which was combined with azathioprine in 37 cases (84%). Of the three patients who never took prednisolone or azathioprine, two were well on symptomatic treatment alone (3,4-diaminopyridine) and one died 28 months into his illness of an unrelated disease. The table outlines details of final treatment.
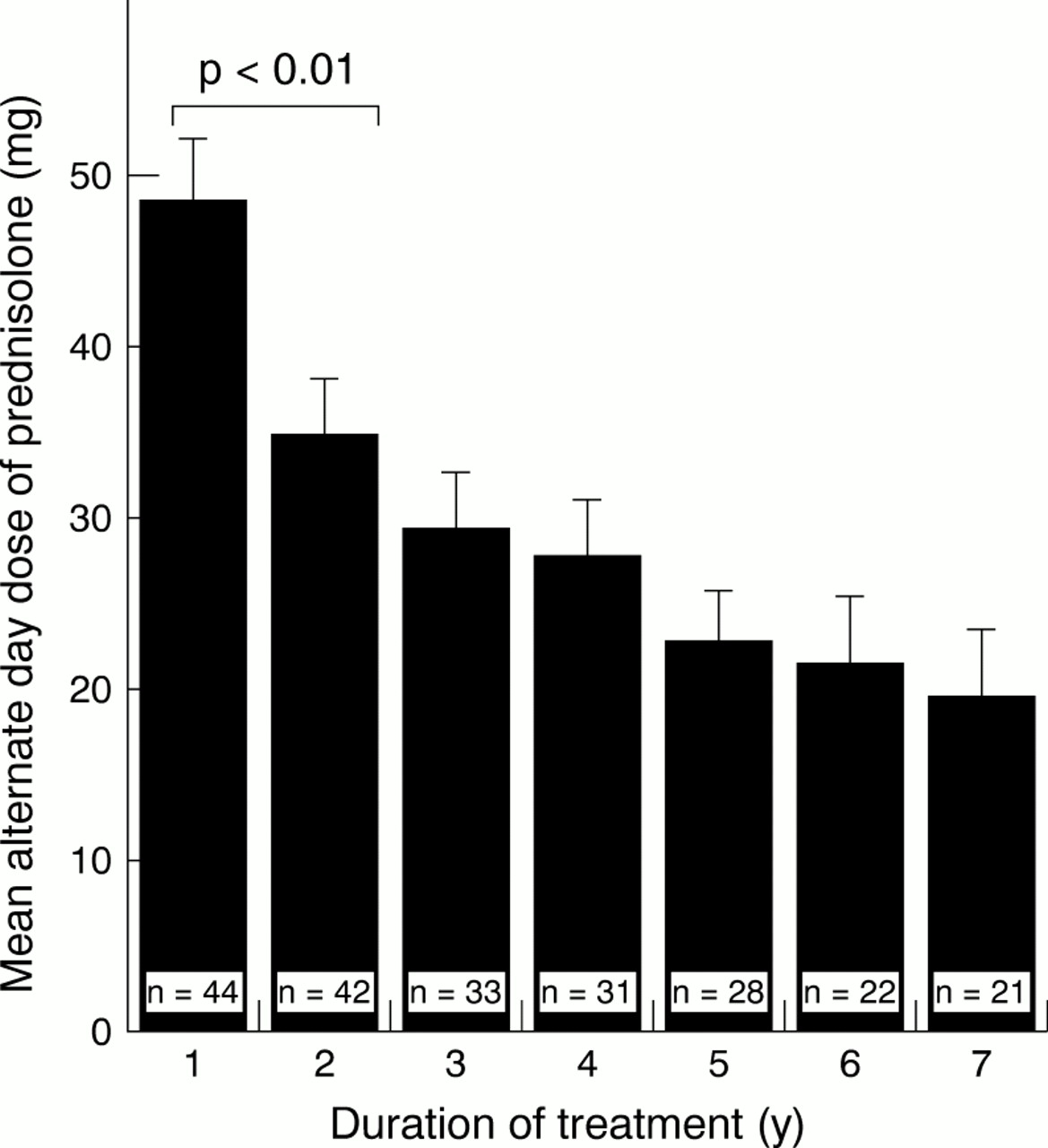
The duration of prednisolone treatment was more than 1 year at final follow up in 43/44 patients. Figure 1 shows the progressive decline in the mean prednisolone dosage for all patients treated. The dose reduction between the 1st and 2nd year of treatment was significant (p=0.005, Mann-Whitney U test). At final follow up, six of 43 (14%) were no longer receiving prednisolone. Reasons for steroid withdrawal were clinical remission (n=5), all attained in year 1, and severe disability despite prolonged immunosuppression (n=1).

Mean alternate day prednisolone dose in patients with LEMS with no detectable lung cancer during follow up. Error bars=1 SEM
Plasma exchange was used initially in moderate to severe cases in conjunction with starting immunosuppression in 26 of 44 patients to produce a response within 2–4 weeks; mean initial muscle scores were significantly lower in this subgroup than in the remainder (p=0.04, Mann-Whitney U test). Seven patients whose LEMS symptoms were only partially controlled using prednisolone and azathioprine had repeated courses of intravenous immunoglobulin therapy at 3 to 6 weekly intervals (dose range 0.8–2.0 mg/kg body weight), continued until the end of follow up in two.
CLINICAL SCORES
All but two patients (96%) had proximal leg weakness as a presenting feature and 44 of 47 (94%) also had proximal arm weakness. Dysphagia was present in 10 (22%) but persisted after treatment in only two (4%). Of the 43 patients who had been on immunosuppression for over a year, clinical scores at final follow up were improved in 38 (88%) after a median treatment duration of 5.9 years.
Voltage gated calcium channel titres
Anti-P/Q-type VGCC antibody titres were available on 44 patients (94%), with no available serum samples in three. Thirty eight (86%) had raised titres (>45 pM). The six patients who were antibody negative had multiple serum samples tested, including at least one obtained before immunosuppressive treatment.
In 23 patients, serum samples were available before starting immunosuppressive treatment. The titre declined in 12 of 23 (52%), but increased in six (26%) (fig 2), the median duration of treatment being 6 years. In three of 23 patients, antibody titres had fallen to control concentrations (<45 pM), each of whom had regained full muscle strength.

Change in antibody titre during long term follow up in 23 patients. Median duration of immunosuppressive treatment between first and last antibody titres=6 years. Horizontal bars represent group mean antibody titre. Overall mean antibody titre was not significantly different after treatment (497 pM pretreatment; 318 pM at final follow up; p=0.11, t test).
Electrophysiological data
Figure 3 shows the increase after treatment in the mean resting CMAP amplitude in the 43 patients on whom pretreatment values were available. Differences were highly significant over the 1st year (p<0.0001, Mann Whitney U test). There was also a significant decline (p<0.0001) in the mean postactivation increment in CMAP amplitudes (fig 4), which remained at less than 100% over the next 4 years.

Mean resting compound muscle action potential amplitude in the ADM in patients with LEMS during follow up. Dashed line=lower limit of normal in healthy controls. Error bars=1 SEM.

Median compound muscle action potential amplitude increment (%) in abductor digiti minimi after 10 seconds maximal voluntary contraction in patients with LEMS during follow up. Dashed line=diagnostic cut off for LEMS. Error bars=upper quartile range.
Paired CMAP amplitude and increment data were available in 31 patients before treatment and at final follow up. The CMAP amplitudes increased in 26 (84%) and postactivation declined in 28 (90%). At final follow up, 11 (35%) had normal resting CMAP amplitudes, 18 (58%) had increments within the normal range, and 10 (32%) had normal values for both.
Correlation between clinical score, electrophysiology, and antibody titres
Initial pretreatment clinical score and CMAP amplitude or increment did not correlate across patients. However, in 22 patients studied serially, significant within patient correlation was found between muscle score and CMAP amplitude in 10 (45%) and between muscle score and CMAP amplitude increment in 11 (50%) (p<0.05, Spearman rank correlation).
The pretreatment anti-VGCC antibody titre did not correlate across patients with either CMAP amplitude, CMAP increment, or clinical score. In nine patients followed up serially in whom anti-VGCC antibody titres were measured on the same day as the documented clinical score and CMAP recordings, significant correlation between antibody titre and CMAP amplitude was only seen in two patients (p<0.05, Spearman rank correlation). In none did antibody titre significantly correlate with clinical score.
Treatment response and clinical remission
At final follow up, 37 of 44 patients who had received immunosuppressive treatment were surviving, of whom 29 (78%) still required prednisolone (mean dose 22.2 mg on alternate days, range 5 mg to 55 mg alternate day dosage), combined with azathioprine in 20 (54%), cyclosporin in three, methotrexate in one, and monthly pooled intravenous immunoglobulin infusions in two. The median duration of immunosuppressive treatment in this group of patients was 6.4 years. Four of the eight surviving patients no longer taking prednisolone at final follow up were taking 3,4-diaminopyridine (3,4-DAP) alone, two were on a combination of azathioprine and 3,4-DAP and two were off all treatment.
Sustained clinical remission was achieved by 20 of 44 (45%) patients of whom all but four required continued immunosuppressive treatment. There was no significant difference in the mean duration of immunosuppressive treatment between patients who achieved remission and those who did not. Kaplan-Meier estimates of survival without remission showed that most patients achieving remission had done so within 3 years of starting treatment (fig 5). Remission was not interrupted by sustained relapses. Transient relapses were usually associated with reduction in immunosuppressive medication and were rapidly reversed by dose increases. In 14 of the 44 surviving patients not in clinical remission at final follow up, three required a wheelchair at all times and a further seven used a wheelchair outside the house.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier proportional estimate of the number of patients with LEMS surviving without remission on follow up. Censored cases are displayed as filled squares.
Of the initial pretreatment variables of clinical score, CMAP amplitude, CMAP increment, anti-VGCC antibody titre, and disease duration before commencement of treatment, the only independent predictor of attaining sustained clinical remission using a Cox proportional hazards model, was initial pretreatment clinical score (p=0.033). None of the other variables (CMAP amplitude, CMAP increment, anti-VGCC antibody titre, pretreatment disease duration) were predictive. Patients presenting initially with a clinical score of 25 were 2.6 times less likely to achieve sustained clinical remission than those with a score of 31.
Prognosis and survival
Ten patients died during follow up after a median duration of LEMS symptoms of 11.4 years. Causes of death were lymphoma (three patients), and single cases of pulmonary embolism, stroke, myocardial infarction, perforated gastric ulcer, bronchopneumonia, peripheral vascular disease, and congestive cardiac failure secondary to ischaemic heart disease. Mean age at death was 69.7 years.
Discussion
In this combined retrospective and prospective study of 47 patients with LEMS without SCLC, we found that proximal muscle strength, but neither electrophysiological measures nor anti-VGCC antibody titres predicted outcome after about 11 years of follow up.
It is unlikely that any of the patients had an undiagnosed SCLC. Only three patients had LEMS symptoms less than 5.5 years (the longest interval we have seen between the onset of neurological symptoms and the appearance of SCLC). Two of these patients died after 2 years, of unrelated causes, and the third is still alive with no detectable cancer 4.5 years after LEMS onset. All three patients were lifelong non-smokers.
The finding of lymphoma in three of our patients adds to the evidence that reticulendothelial tumours may, like SCLC, be implicated in the pathogenesis of paraneoplastic LEMS,18 19 and underscores the need for clinicians to be aware of this possibility. By contrast with the previously reported cases, our patients had been receiving azathioprine, which is known to increase the risk of lymphoma, often in conjunction with other immunosuppressive treatments.20These tumours are usually B cell in type,21 and only very rarely of T cell type.22 However, the tumours were of T cell type in two of our patients, and the duration of azathioprine treatment was relatively short (3 and 7 years). Lymphoma was only diagnosed at postmortem in these two patients (3 and 8 years after LEMS onset). Only in the patient who developed non-Hodgkin's lymphoma (undetermined cell type) after 17 years of treatment with azathioprine does it seem likely that this medication may have predisposed to lymphoma development.
We based the clinical score measures on previous experience, selecting muscle groups that are weakest in LEMS.3 The MRC scale is non-linear and therefore a change in the strength of one muscle from 5 to 4 represents more of a deterioration than a fall from 2 to 1. It is not surprising that initial pretreatment clinical score did not correlate with CMAP amplitude or increment and that in only about 50% of cases did clinical and electrophysiological measurements correlate over time because MRC grading correlates poorly with CMAP measurements in both the ADM and flexor carpi ulnaris in LEMS.23 In other neuromuscular disorders such as amyotrophic lateral sclerosis, CMAP amplitude is not linearly related to MRC score and reduced CMAP amplitudes may be recorded from muscles without detectable weakness.24 In LEMS, muscle strength is difficult to assess accurately, as patients exhibit post-tetanic potentiation, becoming stronger on prolonged voluntary contraction. Most strength measurements in this study were made by one of us (JN-D), thus limiting between rater variability. Our evaluation did not measure autonomic disturbances, but two patients with persistent autonomic symptoms (of erectile impotence and constipation) but who were otherwise well were excluded from the category of remission.
The lack of consistent correlation between clinical score and CMAP amplitude or increment, both within and across patients indicates that the ADM does not accurately reflect overall muscle weakness, even though it is the most sensitive muscle for detecting the electrophysiological changes of LEMS.16 No direct relation was seen across patients between anti-P/Q-type VGCC antibody titre and CMAP amplitude or clinically detectable weakness. Some patients with profound weakness and small CMAP amplitudes had low antibody titres whereas others in clinical remission had persistently high titres. The poor correlation between concentration of VGCC antibody and CMAP amplitude or clinical score suggests that some antibodies detected in the immunoprecipitation assay may not interfere with calcium channel function. In myasthenia gravis there is also no clear correlation between disease severity and antiacetylcholine receptor antibody titre across patients, thought to be due in part to antibody heterogeneity.25 In about one third of patients with LEMS without SCLC, antibodies can be detected to the intracellular β-subunit by radioimmunoassay,26 and presumably do not interfere with VGCC function. Conversely, there may be other undetected antibodies that reduce release of acetylcholine at the neuromuscular junction.
Broadly, mean antibody titres declined after prolonged immunosuppression and most patients improved clinically and electromyographically, suggesting that the antibody titre in part reflects disease severity in individual patients.
The level of immunosuppression required to control symptoms of LEMS in patients in this study, even after over 6 years of treatment, was notably higher than that recorded in a recent trial of prednisolone and azathioprine in myasthenia gravis.27 In that study, 67% of myasthenic patients no longer required prednisolone to remain in remission after 3 years, compared with only 14% of our patients with LEMS. In addition, most myasthenic patients had achieved remission within the 1st year, markedly quicker than remission attainment between 1 and 4 years in our patients with LEMS. This may have been due in part to referral bias, where mildly affected patients with LEMS may not be recognised and diagnosed, biasing towards more severely affected patients.
Survival in our patients with non-SCLC LEMS was favourable: of the 10 patients who died during follow up, the mean age at death was 70 years. Although most of the deaths were due to causes unrelated to LEMS, both the patient who died from bronchopneumonia and the patient who had a perforated gastric ulcer were taking steroids, raising the possibility that their treatment may have been partly responsible for their deaths. Long term disability was high in the remainder of patients where over 25% still required a wheelchair either at all times or for mobilising outside, at final follow up.
We conclude that the prognosis in LEMS without SCLC is variable. Although about half of the patients achieved sustained clinical remission, most of them required substantial and continuing doses of immunosuppressive medication. The only predictor of outcome (clinical remission or independent ambulation) was initial clinical score, comprising strength measurements in proximal limb muscles. Immunological and electrophysiological measurements were useful, however, for monitoring disease progression and response to treatment in individual patients.