Article Text

Abstract
A woman developed brain stem encephalopathy in association with serum anti-Ma2 antibodies and left upper lobe lung mass. T2 weighted MRI of the brain showed abnormalities involving the pons, left middle and superior cerebellar peduncles, and bilateral basal ganglia. Immunohistochemical analysis for serum antineuronal antibodies was confounded by the presence of a non-neuronal specific antinuclear antibody. Immunoblot studies showed the presence of anti-Ma2 antibodies. A premortem tissue diagnosis of the lung mass could not be established despite two CT guided needle biopsies, and the patient died as a result of rapid neurological deterioration. The necropsy showed that the lung lesion was an adenocarcinoma which expressed Ma2 immunoreactive protein. Neuropathological findings included prominent perivascular inflammatory infiltrates, glial nodules, and neuronophagia involving the brain stem, basal ganglia, hippocampus and the dentate nucleus of the cerebellum. Ma2 is an autoantigen previously identified in patients with germ cell tumours of the testis and paraneoplastic brain stem and limbic encephalitis. Our patient's clinical and immunopathological findings indicate that this disorder can affect women with lung adenocarcinoma, and that the encephalitic changes predominate in those regions of the brain known to express high concentrations of Ma proteins.
- paraneoplastic
- brainstem encephalitis
- lung adenocarcinoma
- anti-Ma2 antibody
Statistics from Altmetric.com
Antibodies to Ma2 were originally described in men with testicular cancer and paraneoplastic limbic-brain stem dysfunction.1 Tumour expression of immunoreactive Ma proteins in some of these patients suggests that these antigens, which are widely distributed in normal human brain, are targets of autoimmunity in paraneoplasia. We report on a female patient with brain stem encephalitis, serum anti-Ma2 antibodies, and adenocarcinoma of the lung, and describe the associated tumour and brain immunopathology.
Case history
A 77 year old woman with a 50 pack-year smoking history presented in February 1999 with a 2 month history of progressive unsteadiness of gait and slurring of speech. Left facial weakness and dysphagia had developed in the 3 weeks before admission.
Examination showed an alert and oriented patient with no cognitive dysfunction. A slurring dysarthria was evident. The eye movements were conjugate. There was gaze evoked right beating nystagmus and mild slowing of horizontal saccades. Vertical eye movements were intact. The vestibulo-ocular reflex (VOR) was preserved, but there was bilateral failure of suppression of the VOR. There was mild lower facial weakness on the left. There were no appendicular cerebellar signs but marked ataxia of gait rendered the patient unable to walk without assistance. Muscle bulk, tone, power, reflexes, plantar responses, and sensation were normal.
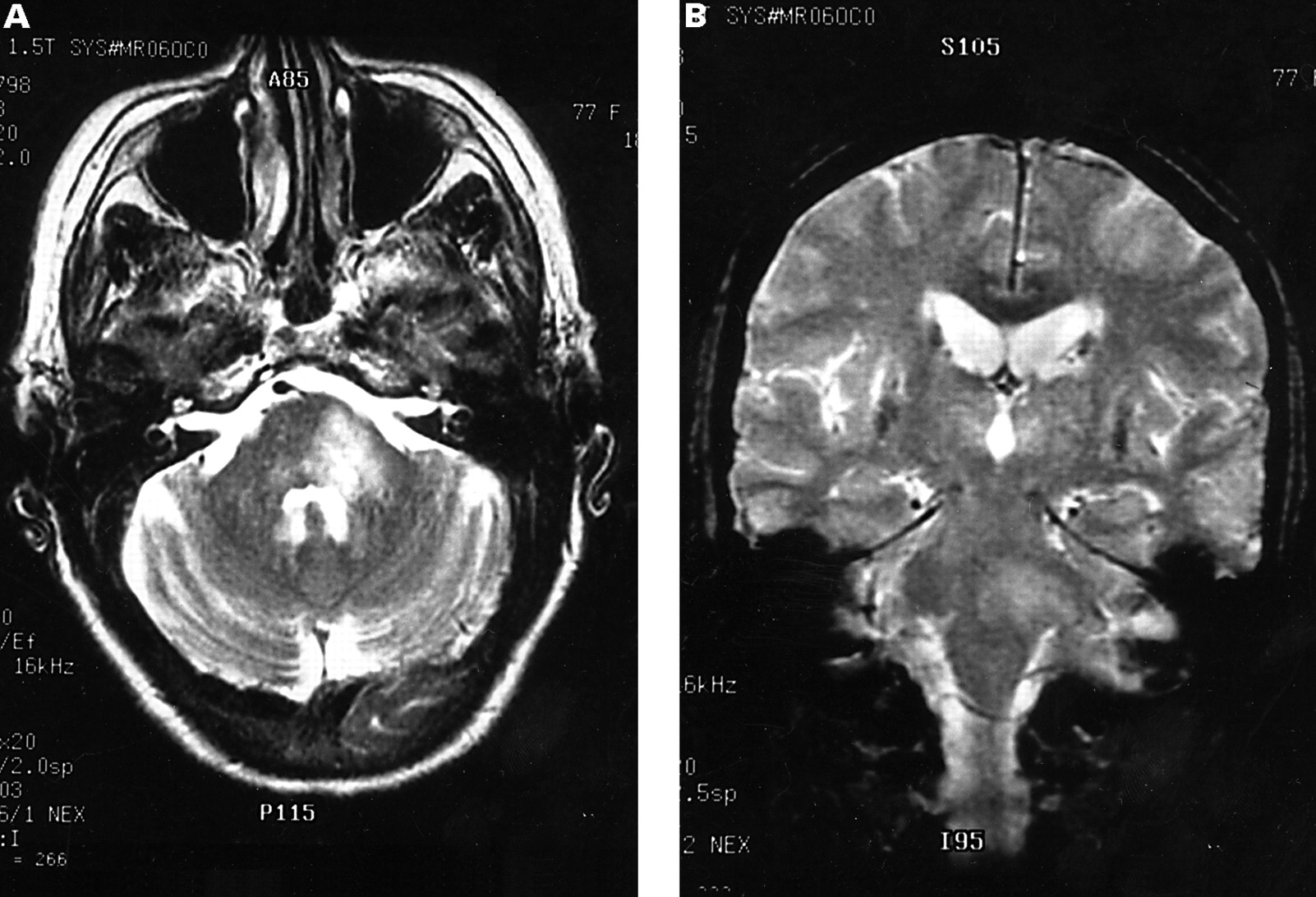
Investigations showed hyponatraemia (124 mmol/l) and a urine osmolality of 542 mmol/l, consistent with inappropriate antidiuretic hormone secretion. The serum contained an antinuclear antibody (ANA) with a titre>2560 and a speckled pattern on immunofluorescence. Anti-dsDNA was not detected by radioimmunoassay. A T2 weighted MR of the brain showed asymmetric scattered high signal intensity lesions in the pons, left middle and superior cerebellar peduncles, and the basal ganglia and internal capsule regions bilaterally (fig 1). A lumbar puncture yielded clear CSF under normal pressure containing 4×106/l lymphocytes, 0.83 g/l protein, and no detectable oligoclonal bands. No malignant cells were identified on CSF cytological examination. Chest radiography showed a small ill defined left upper lobe lesion and chest CT confirmed the presence of a 1.8 cm left upper lobe mass. A fine needle aspiration and core biopsy of the lesion yielded pulmonary alveolar tissue only, and no malignant cells. Investigation for the presence of antineuronal nuclear antibodies by immunofluorescence on monkey cerebellum was confounded by the presence of the high titre antinuclear antibody. A preliminary diagnosis of paraneoplastic brain stem encephalitis was made; however, specific therapy, in particular resection of the undiagnosed pulmonary lesion, was deferred after discussion with the family.

Axial (A) and coronal (B) T2 weighted MRI of the brain showing asymmetric high signal in the brain stem.
Over the next 5 months, progressive bulbar dysfunction, ataxia, and general debilitation ensued. Further examination showed complete external ophthalmoplegia with a left over right skew deviation of the eyes in primary gaze, a left Horner's syndrome, left upper limb ataxia, and a left extensor plantar response. The patient developed aspiration pneumonia and a tracheostomy was performed for airway protection, and percutaneous gastrostomy feeds were begun. Western blot against a panel of paraneoplastic antigens confirmed the presence of anti-Ma2 antibodies. A whole body FDG-PET showed a glucose avid focus in the left upper lobe of the lung consistent with a primary tumour. A repeat CT guided biopsy of the lung mass again yielded no malignant tissue. A course of plasmapheresis was attempted, but the patient was unable to tolerate more than a single 2 litre exchange. Seven months after presentation, a series of prolonged focal and secondarily generalised seizures occurred and the patient died 1 week later.
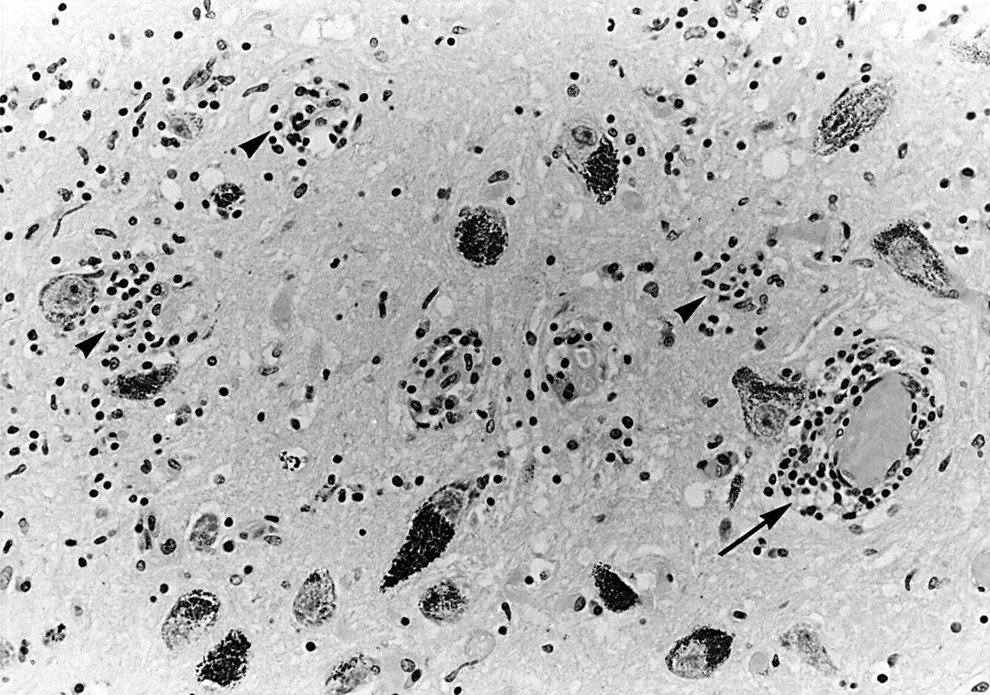
The brain was sectioned coronally and examined after fixation in formalin. Prominent perivascular cuffing with mononuclear inflammatory cells was present throughout the brainstem, basal ganglia, and cerebellar dentate nucleus. Associated neuronophagia and multiple glial nodules (fig 2) were seen in the areas of neuronal degeneration. There was less marked but obvious involvement of the hippocampus and temporal lobe cortex. In the cerebellum there was focal loss of Purkinje cells and an intense proliferation of Bergmann glia, with occasional mononuclear cells. The features were typical of a paraneoplastic encephalitic process. A small old lacunar infarct was noted in the right internal capsule adjacent to the basal ganglia.

Brain stem section showing inflammatory cell cuffing (arrow) and microglial nodules (arrowhead). Haematoxylin and eosin.
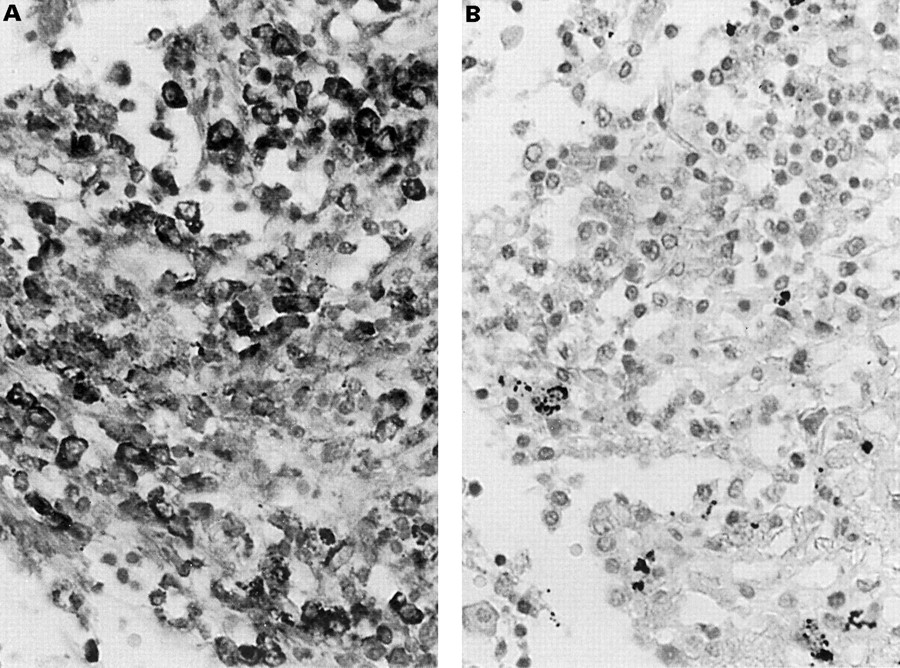
The cut surfaces of the lung showed a poorly defined firm 1.5 cm lesion in the parenchyma near the pleural surface of the left upper lobe. Microscopically, the lesion was composed of sheets of moderately pleomorphic cells which were seen to extend into the adjacent lung alveoli and alveolar ducts lining these structures. The tumour cells stained strongly positive with cytokeratin. The features were those of an adenocarcinoma. An extensive mononuclear inflammatory infiltrate surrounded the lesion. The tumour cells reacted strongly with biotinylated anti-Ma2 IgG, indicating expression of Ma2 protein (fig 3A). The tumour expression of this protein was confirmed with a competition assay between two anti-Ma2 serum samples, as reported.1 Using this technique, preincubation of the tumour section with one anti-Ma2 serum abrogated the reactivity of the biotinylated anti-Ma2 IgG of the other serum. There was no tumour immunoreactivity with normal biotinylated IgG (fig 3 B). The perivascular and parenchymal inflammatory infiltrate within the brain and lung consisted predominantly of CD8+ T cells.

{kind=link}
{kind=link}
{kind=link}
Sections of lung tumour tissue incubated with (A) biotinylated anti-Ma2 IgG demonstrating variable tumour expression of Ma2 protein and (B) biotinylated normal IgG. Counterstained with haematoxylin.
Discussion
Antibodies to Ma2 were originally reported in 10 male patients with testicular cancer and limbic/brain stem encephalitis.1 Recent studies have identified this type of onconeuronal immunity in women, but neuropathological studies were not obtained.2 We describe the clinical and immunopathological findings in a female patient with anti-Ma2 antibodies and paraneoplastic brain stem/limbic encephalitis associated with adenocarcinoma of the lung, and this broadens the range of tumour types shown to express the Ma2 antigen.3
Screening for paraneoplastic antineuronal antibodies by immunofluorescence in this patient was confounded by the presence of a high positive serum antinuclear antibody, and we were unable to establish a tissue diagnosis of lung cancer premortem. This delayed definitive diagnosis and institution of appropriate therapy, and thus illustrates the importance of western blot analysis in the diagnostic work up of such patients. When results of western blotting became available, resection of the undiagnosed pulmonary lesion was not feasible due to general debility.
The Ma2 gene has partial homology with Ma1, which codes for a 37 kDa protein associated with paraneoplastic brainstem or cerebellar dysfunction in patients with tumours of lung, breast, parotid gland, and colon.4 The precise function of the Ma antigens is unknown. However, cumulative experience with 25 patients indicates that Ma2 is a major autoantigen of a paraneoplastic disorder that targets temporal-mesolimbic, diencephalic, and brain stem regions.3 Interestingly, these areas and the dentate nucleus of the cerebellum are the regions that have higher expression of Ma proteins1 and that showed major pathological involvement in our patient.
Clinical stabilisation of neurological paraneoplastic syndromes after tumour resection has been reported,5 6 and previous studies1 suggested that in patients with anti-Ma2 antibodies this may occur more often than in other antibody associated paraneoplastic syndromes of the CNS. Failure to make a premortem tissue diagnosis is, however, not uncommon.7 This has been attributed to a possible antitumour effect of the paraneoplastic immune response, limiting tumour growth and metastasis, and hindering early tumour detection by conventional methods. Indeed, an extensive CD8+ T cell infiltrate was present in the tumour tissue in this case.
We conclude that adenocarcinoma of the lung may be associated with antibodies to Ma2, and that aberrant expression of the Ma2 antigen in lung tumour tissue is the probable stimulus for antibody production. The presence of anti-Ma2 antibodies in the appropriate clinical setting should prompt the clinician to expedite therapy, particularly resection of any demonstrable or suspected tumour tissue.