Article Text

Abstract
OBJECTIVES Urinary dysfunction is a prominent autonomic feature in Parkinson's disease (PD) and multiple system atrophy (MSA), which is not only troublesome but also a cause of morbidity in these disorders. Recent advances in investigative uroneurology offer a better insight into the underlying pathophysiology and appropriate management for urinary dysfunction.
METHODS twenty one patients with PD (15 men, six women, mean age 64 (49–76), mean disease duration 4 years (1–8 years), median Hoehn and Yahr grade 3 (1–4), all taking 300 mg/day of levodopa (100–500 mg)) and 15 with MSA (eight men, seven women, mean age 59 (48–72), mean disease duration 3 years (0.5–6 years)) were recruited. Videourodynamic and sphincter motor unit potential analyses in the patients with PD and MSA were carried out, looking for distinguishing hallmarks that might be useful in the differential diagnosis of these two diseases.
RESULTS Urinary symptoms were found in 72% of patients with PD and in 100% with MSA. Filling phase abnormalities in the videourodynamic study included detrusor hyperreflexia in 81% of patients with PD and 56% with MSA, and uninhibited external sphincter relaxation in 33% of patients with PD and 33% of those with MSA. However, open bladder neck at the start of filling was not seen in patients with PD but was present in 53% of those with MSA, suggestive of internal sphincter denervation. Sphincter motor unit potential analysis showed neurogenic motor unit potentials in 5% of patients with PD and in 93% of those with MSA, suggestive of external sphincter denervation. On voiding, detrusor-external sphincter dyssynergia was not seen in patients with PD but was present in 47% of those with MSA. Pressure-flow analysis showed that the Abrams-Griffiths number, a grading of urethral obstruction (outflow obstruction >40), in PD (40 in women and 43 in men) was larger than that in MSA (12 in women and 28 in men). Weak detrusor in PD (66% of women and 40% of men) was less common than that in MSA (71% of women and 63% of men). Postmicturition residuals >100 ml were absent in patients with PD but were present in 47% of patients with MSA.
CONCLUSION Patients with PD had less severe urinary dysfunction with little evidence of internal or external sphincter denervation, by contrast with the common findings in MSA. The findings of postmicturition residuals >100 ml, detrusor-external sphincter dyssynergia, open bladder neck at the start of bladder filling, and neurogenic sphincter motor unit potentials are highly suggestive of MSA.
- urinary dysfunction
- Parkinson's disease
- multiple system atrophy
- videourodynamic study
Statistics from Altmetric.com
The clinical differential diagnosis of patients with parkinsonism is still a challenge to neurologists. One of the most important differential diagnoses of Parkinson's disease (PD) is multiple system atrophy (MSA) of the striatonigral degeneration type.1 2 Neuronal degeneration in MSA is not restricted to the basal ganglia, but also involves other neuronal systems such as the central autonomic nervous system including the intermediolateral cell column and Onuf's nucleus.3 4 Distinct distribution of the lesions in PD and MSA underlies certain clinical manifestations including urinary dysfunction, which is a prominent autonomic feature both in PD (58%-71%)2 4-12 and MSA (78–96%).2 9-16 The urinary dysfunction can be attributed to dysfunction of two lower urinary tract components; the urethral sphincter and the detrusor. Videourodynamic study is an established method of evaluating these functions.17-20 It is a combination of visualising the lower urinary tract simultaneously with EMG-cystometry, which has been performed mainly in patients with prostate hypertrophy and in those with traumatic spinal cord injury.17-20 However, little is known about dynamic sphincter behaviour in patients with parkinsonism, although the importance of sphincter motor unit potential analysis has been well documented.21-24 In this paper we present data on videourodynamic and sphincter motor unit potential analyses in PD and MSA, looking for distinguishing hallmarks that might be useful in the differential diagnosis in these two disorders.
Materials and methods
We recruited 21 patients with PD and 15 patients with MSA who met the clinical diagnostic criteria.1 2 The patients with PD comprised 15 men and six women with mean age 64 years, ranging from 49 to 76 years. The average duration of the disease was 4 years, ranging from 1 to 8 years, and the median Hoehn and Yahr grade was 3, ranging from 1 to 4. All patients with PD responded well to levodopa treatment. At the time of the study their daily levodopa (with a combination of carbidopa) requirement was 300 mg, ranging from 100 to 500 mg. The patients with MSA comprised eight men and seven women with a mean age of 59 years, ranging from 48 to 72 years. The average duration of disease was of 3 years, ranging from 0.5 to 6 years. None had abnormalities of blood chemistry (including blood sugar) or urinalysis. None had abnormal findings on digital examination or ultrasound echography of the pelvic organs. A detailed urinary questionnaire was given to all patients, which included sensation of urgency; nocturnal (more than twice) and diurnal (more than eight times) urinary frequency and urinary incontinence (filling symptoms); retardation in initiating urination, prolongation, intermittency, straining; and sensation of residual urine (voiding symptoms). Urinary incontinence was further subdivided into urgency type, stress type, and unwitting type (without urgency sensation or physical stress).
The videourodynamic set up is illustrated in figure 1. After voluntary voiding transurethral catheterisation was performed to measure postmicturition residual urine. A triple lumen 7F catheter (for use of contrast medium infusion and use of intravesical and urethral pressures) was inserted into the urethra to perform static urethral pressure profilometry, measuring a urethral pressure by pulling the catheter from inside the bladder (2 cm/min.) throughout the urethra, with infusing sterile water at a rate of 0.33 ml/min. The urethral pressure (pura) showed a maximum value at the external sphincter where the radio opaque marker attached to the urethral luminal orifice was fixed—that is, 2.0 to 2.5 cm below the bladder neck under thex ray fluoroscope. We performed a medium fill (50 ml/min) videourodynamic study on all patients, using a urodynamic computer (Lifetech; Urovision) and an electromyographic computer (Nihon Kohden; Neuropack Σ), simultaneously monitoring and recording the detrusor pressure (pdet), which is the difference of intravesical and intra-abdominal (rectal) pressures, pura, external sphincter EMG activity via a concentric needle electrode, urinary flow via a uroflowmeter, and fluoroscopic images of the bladder and the urethra. We used 20% amidotrizoic acid as a contrast medium infusant for the study. The filling phase abnormalities include detrusor hyperreflexia, which is an involuntary phasic detrusor contraction, and low compliance bladder which is defined as maximum bladder capacity divided by pdet greater than 20 ml/cmH2O.25Open bladder neck is defined as radiographical opening of the bladder neck, which is normally closed during filling.26 27Uninhibited external sphincter relaxation is defined as an involuntary decrement of the external sphincter EMG activity and of pura greater than 25 cm H2O during filling.28 29 The voiding phase abnormalities include detrusor-external sphincter dyssynergia, which is a detrusor contraction concurrent with an involuntary urethral contraction as detected by an increase of the external sphincter EMG activity and of pura, which normally decreases more than 25 cm H2O, with radiographical closure of the external urethral sphincter during voiding.19 20

Videourodynamic set up.
Pressure-flow analysis was performed in all patients, monitoring detrusor pressure and urinary flow. We obtained a relation curve between these two and detrusor pressure (pdet) at the point of maximum urinary flow rate (Qmax)—that is, PdetQmax—which was plotted in the Abrams-Griffiths nomogram30-32 and the Schäfer's nomogram33 by the urodynamic computer. In the Abrams-Griffiths nomogram we obtained the Abrams-Griffiths (AG) number (pdet Qmax−2 Qmax), an estimate of pdet at the point of minimum urinary flow. The AG number represents a numerical grade of obstruction, and an AG number greater than 40 means outflow obstruction in men.30 31 In the Schäfer's nomogram the point of PdetQmax falls into one of four categories of detrusor contractility; strong, normal, weak and very weak, and the last two were designated as weak detrusor in the present study.
Analysis of sphincter motor unit potentials was performed in all patients. According to the criteria proposed by Palaceet al,21 neurogenic sphincter EMG was diagnosed when at least one of the following abnormalities was seen; the average duration of motor unit potentials greater than 10 ms, and the percentage of motor unit potentials with duration greater than 10 ms more than 20%. In addition, we analyzed the number of phases and the amplitude of each motor unit potential. The methods and definitions used for the urodynamic studies conformed to the standards proposed by the International Continence Society34 35 and have been described previously.15 32 All patients gave informed consent before the studies. Statistical analysis was made by Student'st test for AG number and residual urinary volume, and χ2 test for the other variables.
Results
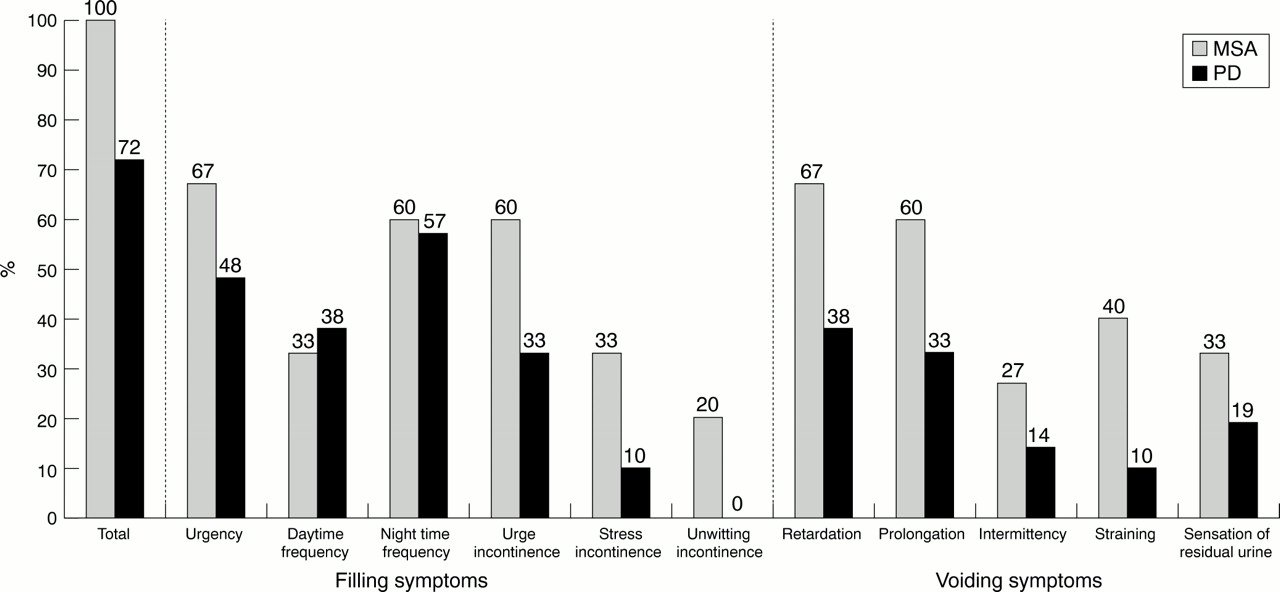
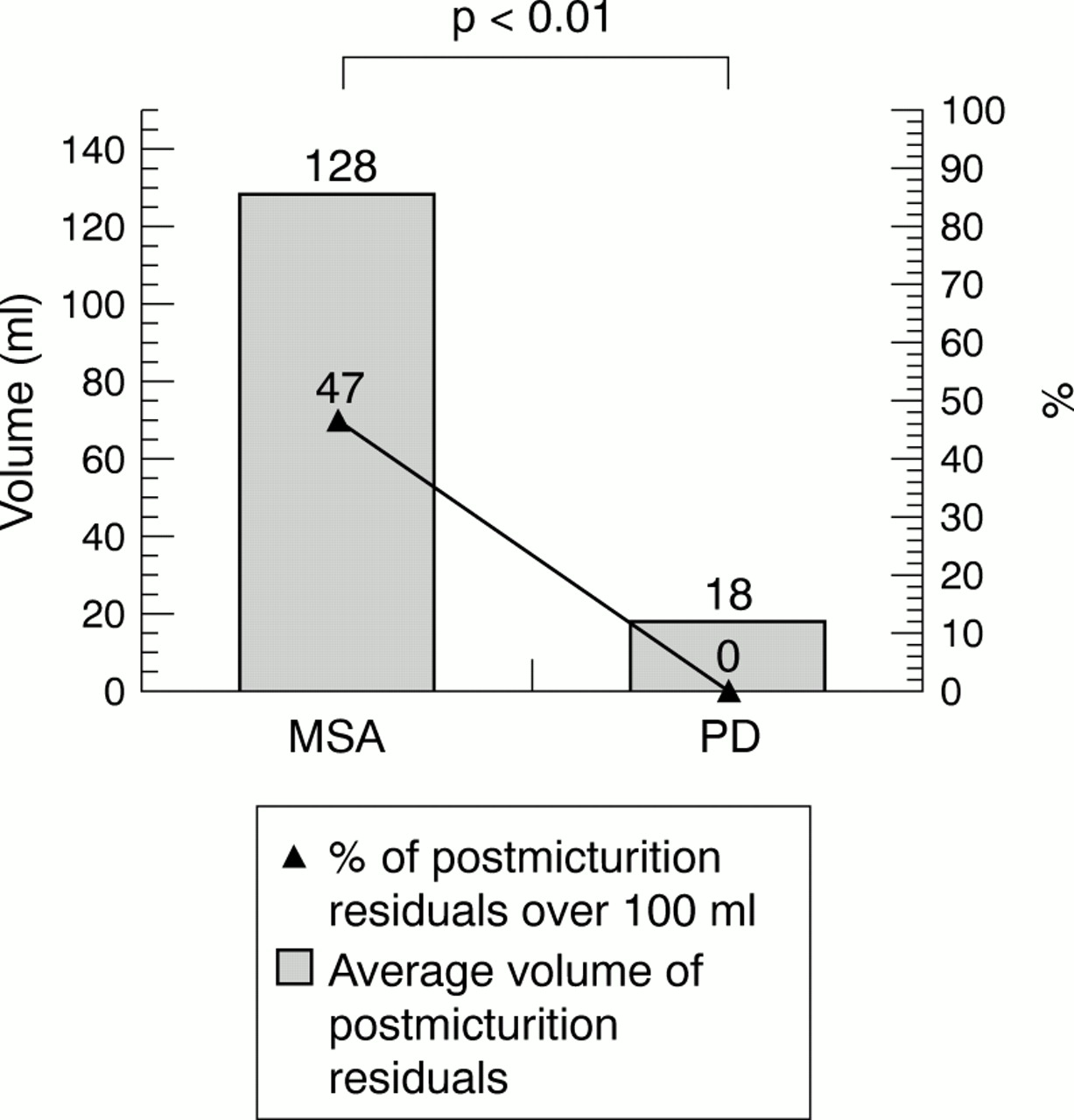
The urinary questionnaire showed urinary symptoms in 72% of patients with PD and in 100% with MSA (fig 2). The most common symptoms were night time urinary frequency (57%) in PD, and both urinary urgency (67%) and retardation in initiating urination (67%) in MSA. Urinary urge incontinence was noted in 33% of patients with PD and 60% of those with MSA. Measurement of residual urine showed that the average volume of postmicturition residuals was smaller in PD (18 ml) than that in MSA (128 ml) (p<0.01), and postmicturition residuals greater than 100 ml were less common in PD (0%) than in MSA (47%, p<0.01, fig 3).
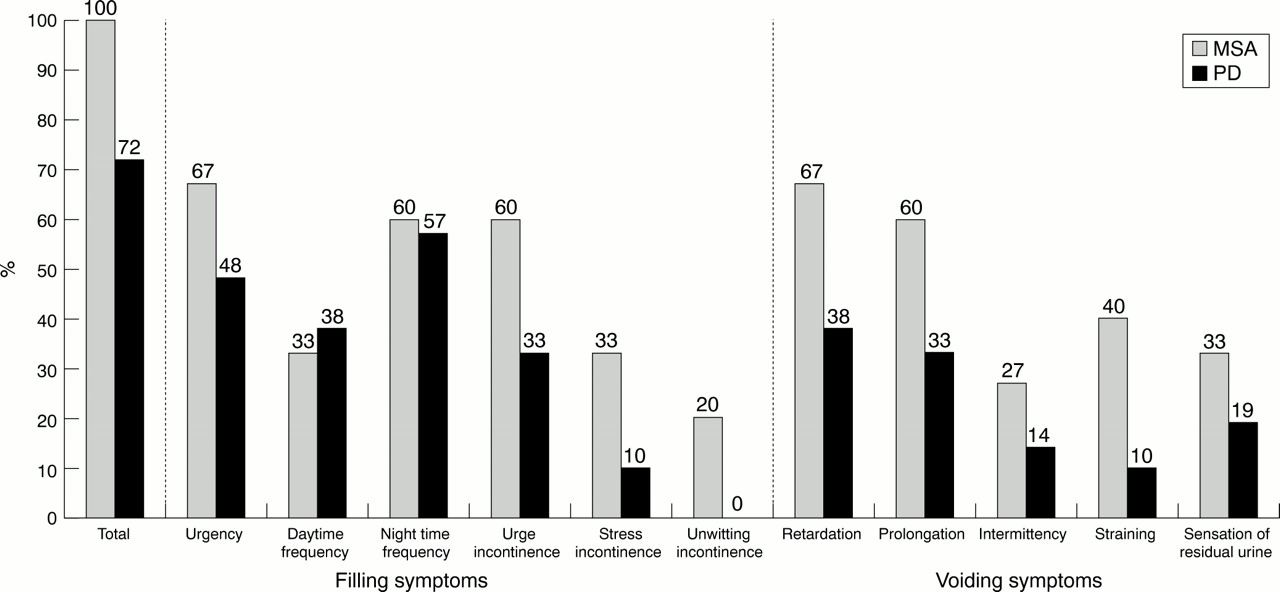
Results of urinary questionnaire. The urinary symptoms in patients with PD were less common than those in multiple system atrophy, although the differences were not significant.

Results of measurement of postmicturition residuals. The average volume of postmicturition residuals in PD (18 ml) is smaller than that in MSA (128 ml) (p<0.01). Postmicturition residuals >100 ml were less common in PD (0%) than in MSA (47%) (p<0.01).
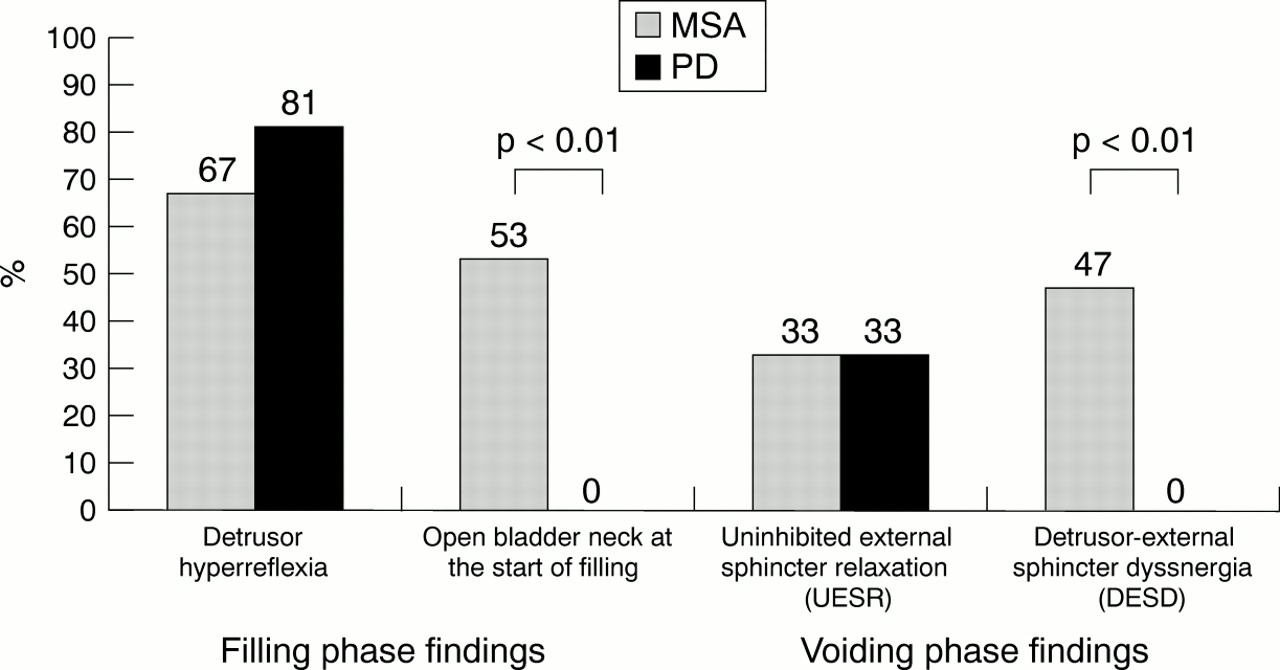
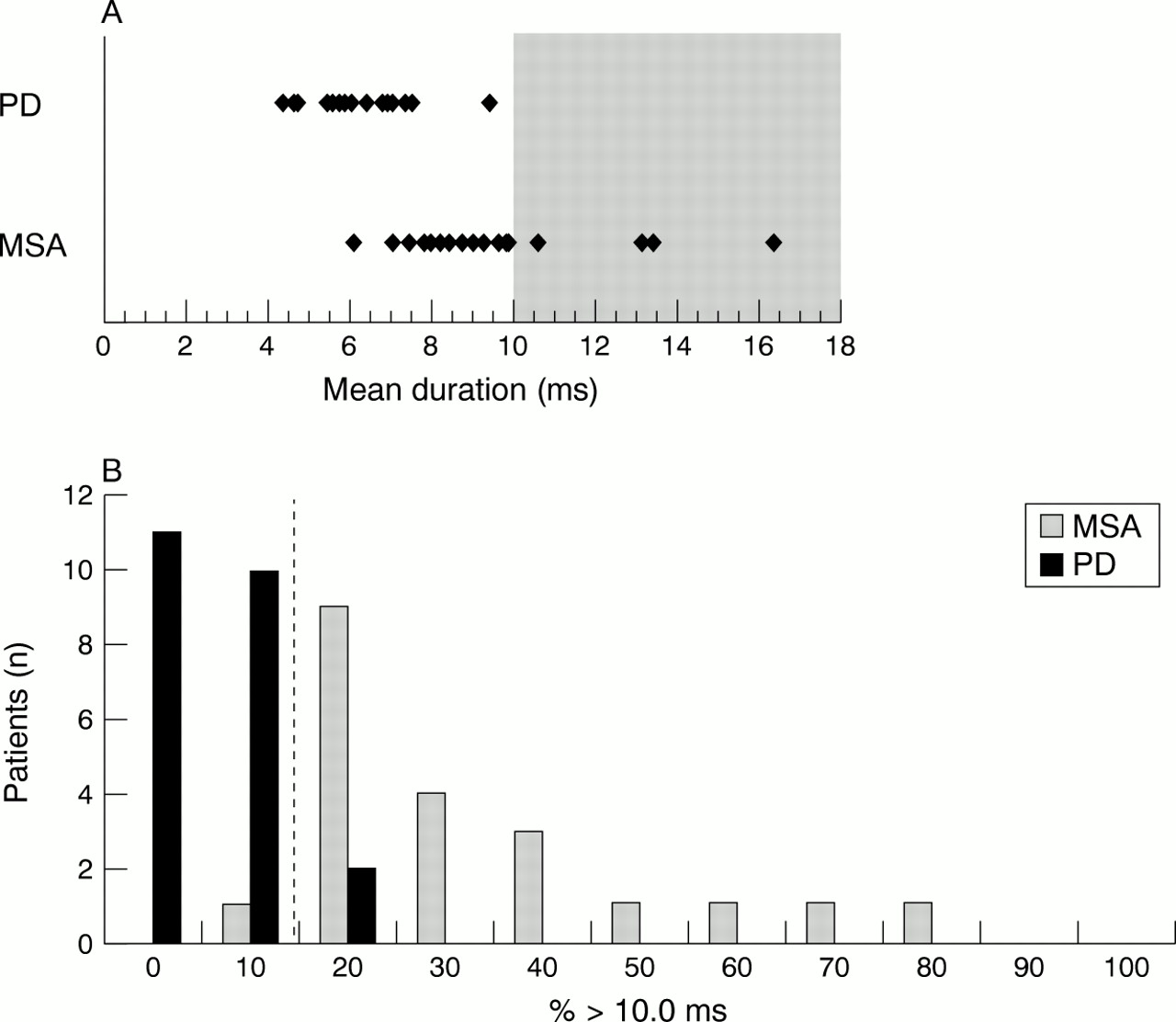
In the filling phase, a videourodynamic study showed detrusor hyperreflexia in 81% of patients with PD and 56% of those with MSA, and uninhibited external sphincter relaxation in 33% of patients with PD and 33% of those with MSA (fig 4). Open bladder neck, which appeared and gradually became manifest during bladder filling, was noted in 31% of patients with PD but in 87% of those with MSA. However, open bladder neck at the start of bladder filling was noted only in patients with MSA (53%; p<0.01; fig 5). Analysis of sphincter motor unit potentials showed motor unit potentials with average duration of over 10 ms only in patients with MSA, and more than 20% of motor unit potentials with duration over 10 ms in 5% of patients with PD but in 93% of those with MSA (p<0.01) (fig 6). The figures were more sensitive with polyphases over five or high amplitude over 800 μV for differentiating these two disorders.

Results of videourodynamic study. Open bladder neck at the start of bladder filling is less common in PD (0%) than in MSA (53%, p<0.01). DESD is less common in PD (0%) than in MSA (47%).
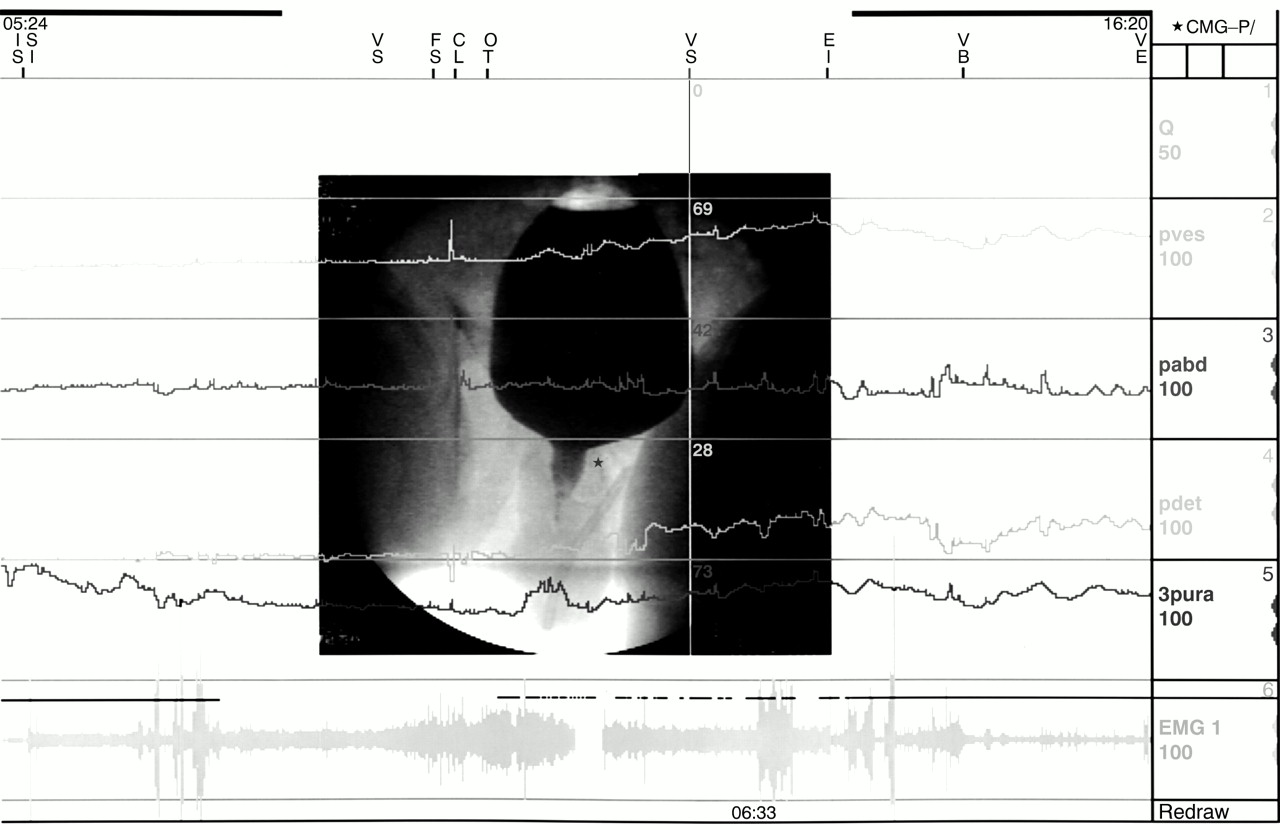
Open bladder neck during filling. A fluoroscopic image showed that the patient (a 56 year old man with MSA) had an open bladder neck (*) during bladder filling (at the point of vertical line). However, EMG activity and the urethral pressure (pura (cm H2O)) did not decrease without evidence of uninhibited external sphincter relaxation. pves=intravesical pressure (cm H2O); pabd=abdominal pressure (cm H2O); pdet=detrusor pressure (pves−pabd (cm H2O)); EMG=external sphincter EMG; Q=urinary flow rate (ml/s).

Results of external sphincter motor unit potential analysis. (A) Motor unit potentials (MUPs) with average duration over 10 ms are seen only in patients with MSA. (B) More than 20% of MUPs with duration >10 ms are noted in 5% of patients with PD but in 93% of patients with MSA (p<0.01).
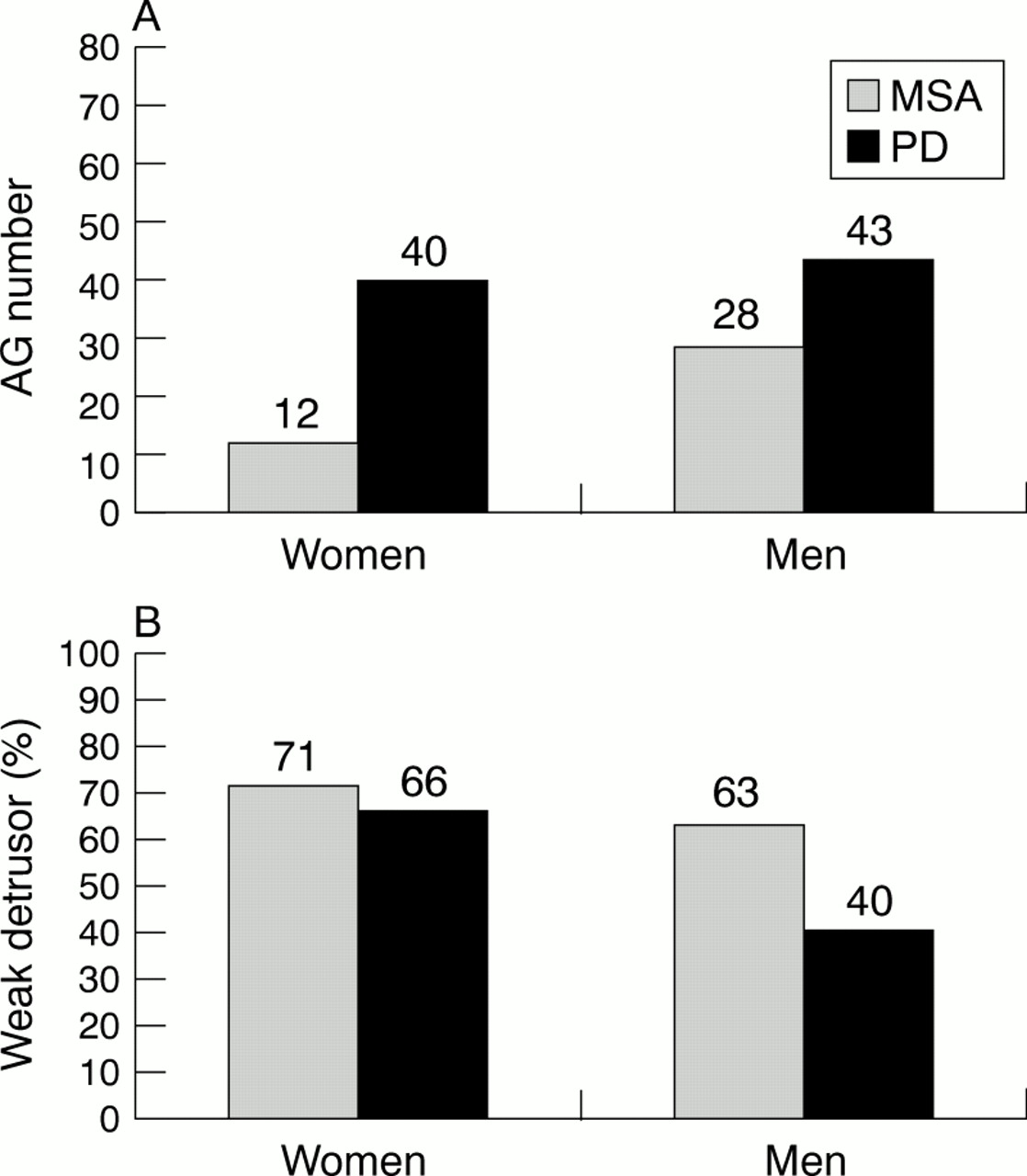
In the voiding phase, detrusor-external sphincter dyssynergia occurred less commonly in PD (0%) than in MSA (47%) (p<0.01). Pressure-flow analysis showed that the AG number in PD (40 in women and 43 in men) was larger than that in MSA (12 in women and 28 in men, respectively), although the differences were not significant (fig 7). Weak detrusor in PD (66% of women and 40% of men) was less common than that in MSA (71% of women and 63% of men), although the difference was not significant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of pressure-flow study. The Abrams-Griffiths (AG) number (a grade of urethral obstruction) in PD was larger than that in MSA. Weak detrusor in PD was less common than that in MSA, although the difference was not significant.
Discussion
The present study aimed at investigating urinary dysfunction in PD and MSA by videourodynamic and sphincter motor unit potential analyses, looking for distinguishing hallmarks that might be useful in the differential diagnosis in these two parkinsonian disorders. The videourodynamic study refers to the simultaneous measurement and display of urodynamic variables with visualisation of the lower urinary tract during bladder filling and voiding. When coupled with a micturition history, this is the most precise diagnostic tool available for evaluating voiding difficulty and incontinence.17-20In the videourodynamic study we used radiographic contrast as the infusant for cystometry, and other urodynamic variables such as detrusor pressure, uroflow, and sphincter EMG are recorded as well. In addition, urethral pressure at the external urethral sphincter can be obtained with visual guidance of radio opaque marker. By simultaneously measuring multiple urodynamic variables, we can better appreciate dynamic behaviour of the internal as well as external sphincters. Because it is difficult for patients with PD to stop taking levodopa, we assessed these patients under medication in the present study, although levodopa is reported to have both inhibitory and facilitatory effects on lower urinary tract function.4-6
As described in previous reports on PD4-12 and MSA,9-16 our patients with PD had less common urinary dysfunction than those with MSA (72% in PD and 100% in MSA). By contrast with MSA, patients with PD had less severe urinary dysfunction. In the filling phase urinary urge incontinence was noted in 33% of patients with PD and in 60% of those with MSA, and in the voiding phase postmicturition residuals greater than 100 ml were absent in patients with PD but present in 47% of those with MSA (p<0.01). The abnormalities of filling phase included detrusor hyperreflexia in 81% of patients with PD and 56% of patients with MSA and uninhibited external sphincter relaxation in 33% of patients with PD and 33% of those with MSA. The figures are almost in accord with those of previous reports,4-16 representing a suprasacral type of parasympathetic and somatic dysfunction.25 It is likely that these videourodynamic abnormalities are relevant to the pathological lesions in PD and MSA,2 3 which include neuronal loss of cells containing neuromelanin in the locus ceruleus (pontine micturition centre)36 37 and in the nigrostriatal dopaminergic system38 39 in PD and MSA and, making a lesser contribution, the frontal cortex36 40 41in MSA. Low compliance detrusor was not seen in the present study, similar to our previous study on PDPD,8 but we found it to occur in 31% of patients with MSA16, most probably reflecting neuronal loss of preganglionic neurons in the parasympathetic intermediolateral nuclei and their fibres (pelvic nerve).3 42
The present study disclosed open bladder neck in 31% of patients with PD but in 87% of those with MSA. The bladder neck, also known as the internal (smooth) sphincter, is a component in the maintenance of continence and has an abundance of α1-adrenergic receptors.43 Because open bladder neck is common in patients with myelodysplasia26 or lower thoracic cord lesion at T12-L244 (where sympathetic intermediolateral nuclei are located) and is reproduced by systemic or intraurethral application of α1-adrenergic blockers,43 it is likely that the open bladder neck reflects sympathetic (hypogastric nerve) denervation.45 Previous videourodynamic studies or fluoroscopic studies alone showed open bladder neck in 23% of patients with PD26 and in 46%-100% of patients withMSA,13 26 44 suggesting the finding as a cause of urinary urgency, although open bladder neck alone was not associated with urinary urgency in our patients. Open bladder neck at the start of bladder filling, even without accompaniment of detrusor hyperreflexia, was not found in PD but occurred in 53% of patients with MSA (p<0.01), evidence of internal sphincter denervation. Therefore, open bladder neck at the start of bladder filling is a feature suggestive of MSA.
The external (striated) sphincter is an another component in the maintenance of continence. External sphincter EMG is an established method to detect neurogenic change of motor unit potentials,22-24 which reflects denervation and re-innervation of the sphincter muscle by lesions in the sacral Onuf's nucleus or its fibres (pudendal nerve).2 46 Previous reports showed neurogenic motor unit potentials in 0%-17% of patients with PD10 12 but in 75%-100%10 12-16 22-24 of patients with MSA. In MSA denervation occurs much earlier in the sphincter muscle than in the other skeletal muscles.22 As an index of neurogenic motor unit potentials, Fowler et al proposed that the average duration of motor unit potentials greater than 10 ms, or the percentage of motor unit potentials with duration greater than 10 ms more than 20% are most sensitive for diagnosing chronic denervation in the differential diagnosis of parkinsonism.21 The results of the present study are in accordance with previous reports, that motor unit potentials with average duration of more than 10 ms. were recorded only in patients with MSA, and more than 20% of motor unit potentials with duration greater than 10 ms. were recorded in 5% of patients with PD but in 93% of those with MSA (p<0.01), evidence of external sphincter denervation. Therefore, neurogenic motor unit potentials are also a feature suggestive of MSA when comparing these two disorders.
We performed pressure-flow analysis along with the videourodynamic study during voiding, which refers to the simultaneous monitoring of detrusor pressure and urinary flow, and drawing the relation curve between these two. Although it was originally developed as a diagnostic tool for outlet obstruction due to prostate hypertrophy,30 31 33 pressure-flow analysis is useful for evaluating neurogenic voiding difficulty and providing objective indices of outflow obstruction and detrusor contractility.30-33 The pressure-flow analysis in the present study showed that the AG number in PD was larger than that in MSA. The AG number represents a numerical grade of urethral obstruction, and a value greater than 40 means outflow obstruction in men.30 31 Therefore, it seems likely that the urethral resistance in PD is larger than that in MSA. Previously we showed that detrusor-external sphincter dyssynergia is a factor contributing to neurogenic urethral relaxation failure, which is often seen in suprasacral pudendal nerve lesion.32 However, none of the patients with PD and 47% of those with MSA in the present study had detrusor-external sphincter dyssynergia. Although high urethral resistance is found in patients with detrusor instability,47 48 the exact reason for an obstructive pattern in PD is uncertain. Patients with PD are reported to have high resting urethral pressure, probably due to medication—that is, levodopa and its metabolites such as noradrenaline (norepinephrine)—which may contract the bladder neck via α1-adrenergic receptors.49 We did not measure urethral pressure at the bladder neck during voiding, and there is no report of the incidence of detrusor-bladder neck dyssynergia50 in PD or MSA. By contrast, our previous report showed that up to 40% of patients with MSA had low resting urethral pressure, most probably due to sphincter denervation.16 Pressure-flow analysis showed that weak detrusor during voiding in PD (66% of women and 40% of men) was less common than that in MSA (71% of women and 63% of men), indicative of parasympathetic dysfunction innervating the bladder.
In conclusion, our findings suggest that the videourodynamic and sphincter motor unit potential analyses are useful in distinguishing PD from MSA. Patients with PD had less severe urinary dysfunction without evidence of internal or external sphincter denervation. By contrast, the findings of post-micturition residuals greater than 100 ml, detrusor-external sphincter dyssynergia, open bladder neck at the start of bladder filling, and neurogenic sphincter motor unit potentials are highly suggestive of MSA.
Acknowledgments
We appreciate the assistance given by Ms Katayama and Ms Matsudo. The patients were cared for by staff in Neurology Ward East 11 of the Chiba University Hospital. This study was supported in part by grants from the Research Committee on Ataxic Diseases, the Ministry of Health and Welfare in Japan.