Article Text

Abstract
Objectives: To evaluate the safety and efficacy of a new dual channel stimulator (Kinetra) in patients with severe Parkinson's disease (PD) or essential tremor (ET).
Methods: 111 patients with PD and 18 with ET were studied. Leads were implanted into the subthalamic nucleus (STN) or internal globus pallidus of patients with the akinetic/rigid type of PD. Leads were implanted into the ventral intermediate nucleus (VIM) of the thalamus or the STN in patients with the tremor dominant type of PD and in those with ET. Technical data on the device and adverse events occurring during the study were documented. Patients were assessed with established and validated clinical scales before surgery and at three and six months' follow up.
Results: No device failure or unexpected adverse events occurred during the study. The dual channel stimulator used in stimulation of the STN, internal globus pallidus, and VIM in PD and ET was as safe and effective as the single channel stimulators in use. Mortality, morbidity, and infections were documented in the 129 treated patients. The parameter settings were similar to those usually programmed with single channel stimulators. Time spent in the operating room to implant the Kinetra system was systematically documented. In the PD group, improvement in the unified Parkinson's disease rating scale motor score, decrease in medication OFF periods, and reduced levodopa induced dyskinesia by bilateral STN stimulation were similar to those previously reported with bilaterally applied single channel stimulators. In the ET group upper and lower limb tremor scores were reduced by VIM stimulation. Activities of daily living improved in both disease groups.
Conclusion: The Kinetra facilitated bilateral deep brain stimulation implantation surgery and is easy to use. It offers more advantages for the patient than the single channel stimulators; consequently, this new device may be recommended to treat patients with severe PD and ET.
- essential tremor
- Parkinson's disease
- deep brain stimulation
- multicentre trial
- dual channel device
- DBS, deep brain stimulation
- ET, essential tremor
- ETRS, essential tremor rating scale
- GPi, internal globus pallidus
- PD, Parkinson's disease
- STN, subthalamic nucleus
- UPDRS, unified Parkinson's disease rating scale
- VIM, ventral intermediate nucleus
Statistics from Altmetric.com
- DBS, deep brain stimulation
- ET, essential tremor
- ETRS, essential tremor rating scale
- GPi, internal globus pallidus
- PD, Parkinson's disease
- STN, subthalamic nucleus
- UPDRS, unified Parkinson's disease rating scale
- VIM, ventral intermediate nucleus
High frequency deep brain stimulation (DBS) has become a widely used procedure for the management of severe movement disorders when symptoms can no longer be improved by adjustment of medical treatment. It is a safe, bilateral, and reversible treatment performed by bilateral implantation of leads into the target areas.1–3 The mechanism of action of DBS seems to be complex, involving both depolarisation block and release of neurotransmitters.4
In the past, ablative surgery such as thalamotomy or pallidotomy was performed to treat severe tremor and dyskinesias in patients with Parkinson's disease (PD). Ablative surgery is non-reversible and usually performed unilaterally. If performed bilaterally there is a high risk of severe side effects in the form of dysarthria and cognitive deficits,5–7 while bilateral DBS rarely affects cognitive functions.5–8 Because of the significant symptomatic effect and advantages of DBS, ablative surgery is now rarely recommended.7–16 DBS can also be applied in patients who already have received ablative surgery.14–17
DBS was first done in 1987 in the ventral intermediate nucleus of the thalamus (VIM) to treat essential (ET) and parkinsonian tremor.17 DBS has since been extended to the subthalamic nucleus (STN) and the internal part of the globus pallidus (GPi) to treat patients with advanced PD and motor complications in the form of the ON-OFF phenomenon and dyskinesias. Considerable and significant improvement in motor function and significant reduction in duration of OFF periods and dyskinesia have been shown in several studies.2–21
Until now bilateral DBS has required two separate procedures for the implantation of the two extensions, the leads, and the two single channel stimulators (Itrel II, Medtronic Inc, Minneapolis, Minnesota, USA). This involves repositioning and redraping during the second step of DBS surgery. To facilitate the procedure for bilateral stimulation and to improve the comfort of the patient, a one sided dual channel system was developed to provide stimulation through two DBS leads.
The present study aimed at evaluating the use of this dual channel stimulator (Kinetra, Medtronic Inc) for the treatment of severe PD with motor fluctuations and dyskinesia and for the treatment of ET in a prospective multicentre, open label clinical trial, which focused on surgical safety and technical performance of the device.
MATERIAL AND METHODS
Study design
This prospective multicentre, open label clinical study was designed and conducted according to the rules and regulations of the European directive on clinical studies with medical devices, EN 540, and the Declaration of Helsinki. Ethical committee approval was obtained from each participating centre before patient enrolment and informed consent was obtained for each patient.
Seventeen investigators with 18 centres in 12 countries participated in the study: 1 centre in Australia, 1 centre in Canada, and 16 centres in Europe. The study evaluated the Kinetra from implantation to a follow up visit at six months.
The primary focus was evaluating the performance and the safety of the system in a clinical setting during implantation and at three and six months' follow up. Secondary objectives were to monitor the DBS lead and Kinetra implantation technique and device use in daily practice. Furthermore, adverse events, parameter settings, and the use of the patient therapy controller (Access Therapy Controller, Medtronic Inc) were documented.
To evaluate the efficacy of the Kinetra, patients with PD were evaluated using the unified Parkinson's disease rating scale (UPDRS) and patients with ET by means of the essential tremor rating scale (ETRS).22–23 The scores were collected at baseline and at three and six months' follow up in medication OFF with stimulation ON or OFF. Lastly, the time required for the Kinetra implantation surgery was documented. Data concerning levodopa induced motor complications were collected in the medication ON condition.
Patient selection
Patients were enrolled if they had severe idiopathic PD with motor fluctuations or dyskinesias or ET and further improvement by medical adjustment was not possible. Patients 18 years or older who gave informed consent were considered for study enrolment. Patients were excluded if they had dementia or psychiatric disease, were pregnant or planning to be during the study, and were unable or unwilling to adhere to the study.
A total of 129 patients were enrolled in the study. Data for 111 patients with PD and 18 patients with ET were analysed for safety, demographics, stimulation parameter settings, system tests, and efficacy.
Device description
The Kinetra allows bilateral DBS through two leads programmed independently with one pulse generator. The special programming features in the Kinetra system are two different methods to set parameter limits (custom limits or autotracking), a day cycler (a method of synchronising the patient's therapy schedule to the 24 hour clock), cycling (in cycling mode, cycle time ON is the length of time that stimulation is delivered and cycle time OFF is the length of time between stimulation periods), and SoftStart/Stop (this causes the amplitude to increase from zero to the selected output amplitude and to decrease from the selected output amplitude to zero). The neurostimulator battery can be checked by different tests such as status (OK, low, or end of life), capacity (in volts), use (full or percentage used), and battery current (in microamps). The patients were able to use either a therapy controller (Access Therapy Controller) or a magnet to control the Kinetra. The Access Therapy Controller is a hand held battery powered device that allows the patient to turn the neurostimulator on and off and to check the neurostimulator battery status. In addition, the therapy controller can adjust stimulation amplitude, pulse width, and rate within a physician prescribed range of settings. The amplitude (0 to 10.5 V) and pulse width (60 to 450 μs) can be separately programmed for each channel. The stimulation frequency (2 to 250 Hz) is the same for both channels.
Three lengths of extension cable were available, depending on whether the stimulator was in a subclavicular (51 or 66 cm) or abdominal location (95 cm). Quadripolar leads, and in one patient a unipolar lead (already implanted before the start of the study), were used in the study. The Kinetra weighs 80.5 g and measures 60 × 77 × 13 mm. It consists of a titanium case enclosing a silver vanadium oxide battery and the electronic circuit of the stimulator.
Surgical technique
DBS was performed after stereotactic implantation of the DBS leads according to the procedure of each centre, which varied greatly (computed tomography, magnetic resonance imaging, ventriculography). A total of 260 DBS leads were implanted under local anaesthesia, while the Kinetra was implanted under general anaesthesia. The leads were fixed with a burr hole cap, with bone cement and anchoring sutures, or with microplates. In total 251 leads and extensions were connected at the scalp level and 4 leads were connected to the extension in the neck. For three leads this information is missing (only 258 extension connections were needed for 260 leads). The extensions were tunnelled subcutaneously, in a variety of ways depending on the preference of the surgeon, to a subclavicular pocket in 111 patients and to an abdominal pocket in 18 patients.
Statistical evaluation
The statistical analysis program SAS release 6.12 was used for data analysis. Descriptive statistics are given parametrically as mean (SD) and non-parametrically as median (quartiles). Comparative statistical tests were done on differences of individual items and sum scores of combinations of items of UPDRS and ETRS, respectively. As there was no clear evidence that data could be assumed to be distributed normally, we used the non-parametric Wilcoxon signed rank test to calculate the significance of the stimulation effect (stimulation ON versus stimulation OFF at the same follow up) and of the procedure effect (stimulation ON versus before surgery) at three and six months' follow up. The global maximal level of significance was set at 5%. All p values are given for two tailed tests.
RESULTS
All Kinetra neurostimulators were implanted between July 1998 and October 1999. Implantation of the Kinetra was an ongoing process over the study period. This means that not all patients had completed the three and six months' follow up by the end of the study. Table 1 gives an overview of the available data from baseline to study closure.
Maximum available data during follow up in patients with Parkinson's disease (PD) and essential tremor (ET) (all patients received bilateral lead implant)
Baseline characteristics
Table 2 summarises patients' characteristics. Of the 111 patients with PD, 15 had had an earlier neurosurgical procedure: two patients had a thalamotomy, one had a pallidotomy, one had both a thalamotomy and DBS, and the remaining 11 had DBS in different targets. Two ET patients had had an earlier DBS treatment. None of the patients had an implant in a previously lesioned target.
Patients' characteristics at baseline
Device performance
No device failure was reported during the study. The stimulation parameter settings amplitude, pulse width, and frequency did not change significantly during the study. At the six month visit, data for 98 leads were available. Few patients with PD had leads implanted in the GPi or the VIM and only adverse events, and no clinical results, of these patients are reported. In the PD group the median amplitude was 2.7 V (range 1.6–3.6, 10–90 quartiles), the median pulse width was 60 μs (range 60–90, 10–90 quartiles), and the median frequency was 163 Hz (range 130–235, 10–90 quartiles). For patients with ET the median amplitude was 2.1 V (range 1.9–3.5, 10–90 quartiles), the median pulse width was 120 μs (range 90–210, 10–90 quartiles), and the median frequency was 160 Hz (range 120–185, 10–90 quartiles).
Two modes of stimulation were available. In the unipolar mode the case of the stimulator was selected as the anode (positive pole) and at least one electrode as the cathode (negative pole). This mode was used in 82 leads (75 in PD and 7 in ET patients) at study closure. The bipolar mode was defined by at least one electrode selected as the cathode and at least one as the anode. Bipolar mode was used at study closure in 13 leads (7 in PD and 6 in ET patients). For the remaining three leads this information was missing.
A tendency was observed towards a more frequent use of patient therapy controller at the six months' follow up. At implantation 36 (29%) of 124 patients and at six months 22 (47%) of 47 patients were using the patient therapy controller. The cycling mode was transiently used by two patients with PD, and two patients with ET regularly used the day cycler. The battery status was reported as OK for all patients during the study.
Seven patients in three centres underwent magnetic resonance imaging after implantation of the Kinetra with no complication.24
Surgical experience
In the patients with PD, 209 leads were implanted in the STN, 10 in the VIM, and 4 in the GPi. In the patients with ET, 37 leads were implanted in the VIM. In total 129 Kinetra neurostimulators were implanted.
The operating room time for implantation of the Kinetra neurostimulator and the extension cables was defined as the time that elapsed between skin incision and skin closure. The median operating room time for the Kinetra was 55 minutes (45 minutes to 1 hour 19 minutes, 25–75 quartiles) and the median total (bilateral leads plus extensions plus neurostimulator) operating room time was 4 hours 55 minutes (3 hours 5 minutes to 7½12 hours, 25–75 quartiles).
Neurological outcome
Parkinson's disease (n = 111)
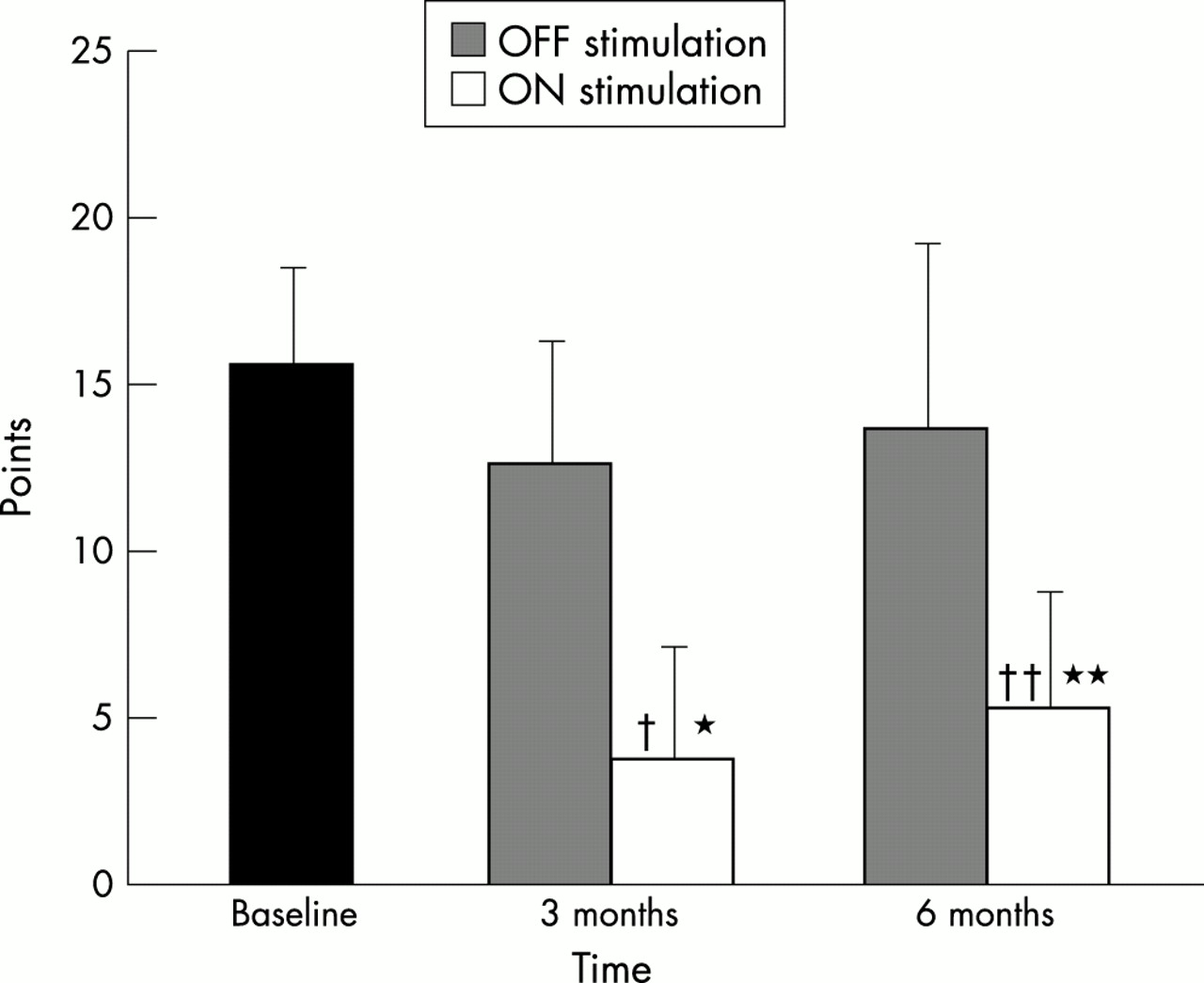
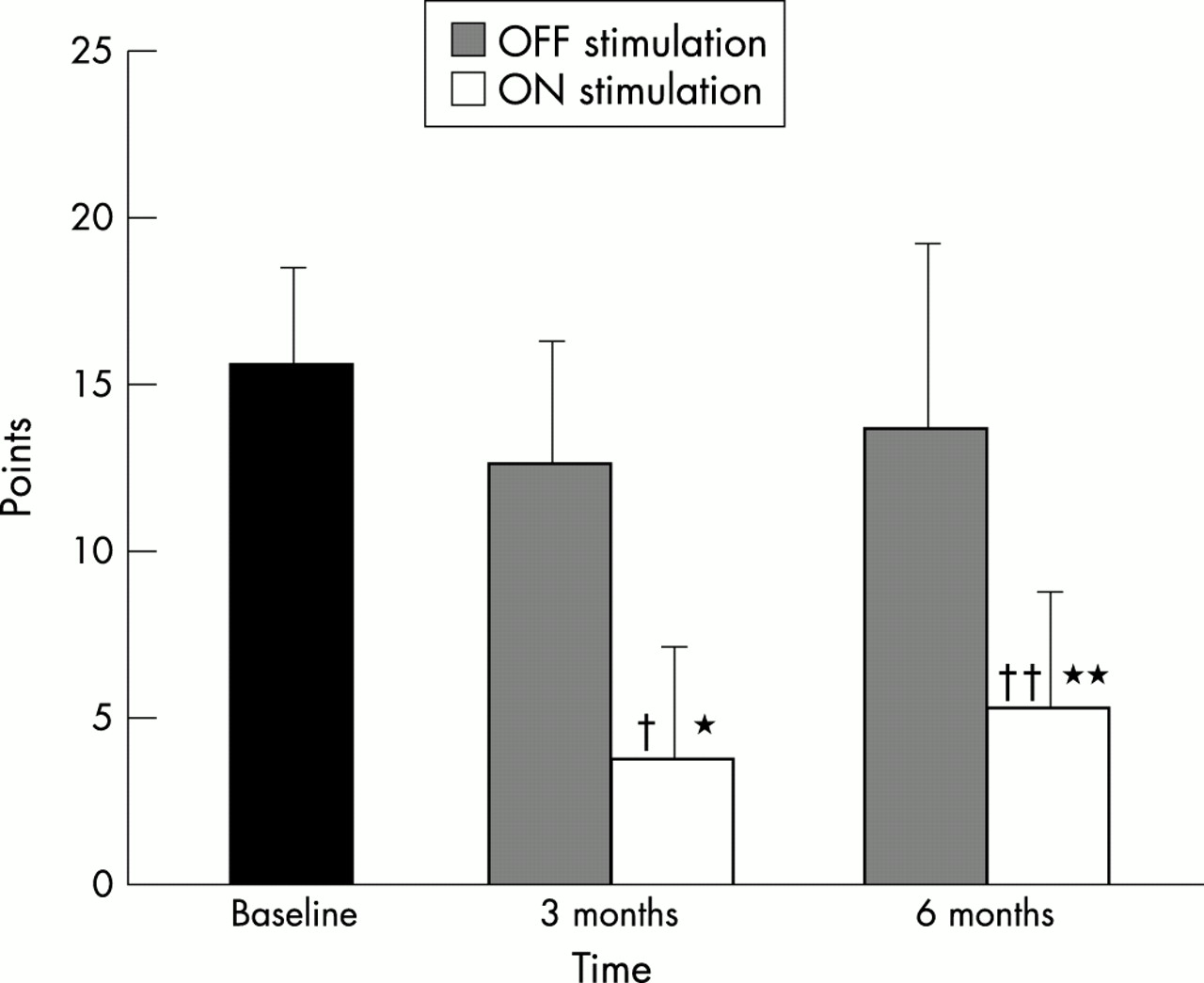
The effects of stimulation (ON versus OFF stimulation) and procedure (before surgery versus ON stimulation) on motor score (UPDRS part III), activities of daily living (UPDRS part II), dyskinesia duration and severity (UPDRS part IV, items 32 and 33), and the medication OFF periods (UPDRS part IV, item 39) were analysed for the total population of 104 patients with PD treated with bilateral STN stimulation. Patients with PD in whom leads were implanted in the VIM (n = 5) or the GPi (n = 2) were excluded from the efficacy analysis because of their small number. At three and six months' follow up, both activities of daily living and total motor scores were significantly improved by stimulation and procedure (p < 0.00001; fig 1). Duration and severity of levodopa induced dyskinesia and OFF periods evaluated in the medication ON-stimulation ON condition were significantly reduced at three and six months' follow up (fig 2). Activities of daily living improved significantly in the medication ON-stimulation ON condition (p < 0.00001) according to the UPDRS part II, from 27.1 (7.8) (baseline) to 12.9 (8.1) and 12.1 (7.7) at three and six months' follow up, respectively. The OFF stimulation condition (medication ON-stimulation OFF) was significantly improved at three months (27.1 (7.8) to 22.7 (10.9), p = 0.0001) and at six months' follow up (27.1 (7.8) to 23.6 (8.9), p = 0.02).

Effect of subthalamic nucleus stimulation (OFF or ON) on total motor score (unified Parkinson's disease rating scale (UPDRS) III) in Parkinson's disease (mean (SD)). Stimulation effect, *p < 0.00001; procedure effect, †p < 0.00001.

Effect of subthalamic nucleus stimulation on duration and severity of dyskinesia (items 32, 33, and UPDRS IV) and on the OFF period proportion (item 39, UPDRS IV) in the ON medication condition in Parkinson's disease (mean (SD)). *p < 0.00001.
Essential tremor (n = 18)
In the final statistical analysis, only patients with either an upper or lower limb score ≥ 2 at baseline (≥ 2 in item 5, 6, 8, 9) according to the ETRS were included. The effects of stimulation (ON versus OFF stimulation) and procedure (before surgery versus ON stimulation) on upper limb tremor scores (items 5 and 6) and lower limb tremor scores (items 8 and 9) of the ETRS were evaluated at the three and six months' follow up. Both stimulation and procedure significantly reduced upper limb tremor at three and six months (fig 3). Stimulation significantly reduced lower limb tremor at three months (p = 0.0078) but, most likely because of the small number of patients (n = 9), not at six months (p = 0.06). The procedure significantly reduced lower limb tremor at three months (p = 0.01) and at six months (p = 0.03).
{kind=link}
{kind=link}
{kind=link}
Effect of ventral intermediate nucleus stimulation on upper limb tremor scores (items 5 and 6) (mean (SD)). Stimulation effect, *p = 0.0001, **p = 0.0039; procedure effect, †p = 0.0001; ††p = 0.0039.
Adverse events
Adverse events were reported by 129 patients with an implanted Kinetra system. No unexpected device related adverse events were reported during the study. We defined four groups of adverse events: (a) procedure related neurological adverse events; (b) device related technical adverse events; (c) surgery related adverse events, subdivided into lead implantation related adverse events, extension and Kinetra implantation related adverse events, and infections; and (d) other adverse events.
There were 119 adverse events in 65 patients (98 adverse events in 55 PD patients, 21 adverse events in 10 ET patients) during the follow up period (table 3).
Category and severity of adverse events (AE) in the whole group and in patients with PD and ET
Four patients died during the study: three from causes unrelated to surgery or stimulation and one from lead implantation surgery following an intracerebral haemorrhage. Only adverse events reported more than twice are discussed in detail.
Of the 119 adverse events, 56 (47%) neurological adverse events occurred in 34 patients (28 PD and 6 ET) during the study. Sixteen were classified as gait disorders and occurred in 10 PD patients. Mental and psychiatric disturbances—attention or cognitive deficits, depression, mental confusion, and psychiatric disorders—occurred 12 times in 10 patients. The other adverse effects were dysarthria (three patients), dysphagia (three patients), paraesthesia (three patients), and eyelid apraxia (three patients). Twelve of the 56 neurological adverse effects were classified as severe. All were resolved at the end of the study, two of them with residual effects.
Six technical adverse events were reported and were completely resolved at the end of the study. Four technical adverse events were related to telemetry malfunction in three patients. The remaining two of the six were related to patient therapy controller malfunction. None of these technical adverse events could be verified by technical assessment as technical failures.
Sixteen of the 36 surgery related adverse events were linked to lead implantation in 12 patients (one patient died of intracerebral haemorrhage, one subcutaneous haematoma, three additional intracranial haemorrhages, two lead dislodgements, one seizure, and eight others). Eleven adverse events were related to extension and Kinetra system implantation in nine patients (five subcutaneous haematomas, two seromas, one pain at the neurostimulator site, and three others). All subcutaneous haematomas and all but two intracranial haemorrhages were resolved at the end of the study. Infections occurred nine times in seven of the 129 patients. In six patients the infection was related to the Kinetra and in one patient it was related to the lead. All infections but one were resolved. The unresolved haematomas and the infection were still under observation at the end of the study.
In conclusion, most adverse events were resolved at the end of the study. Of the 129 patients treated with DBS one patient died of intracerebral haemorrhage (0.8%) and two patients with intracerebral haemorrhage had residual signs (1.6%). Two neurological adverse events were resolved with residual effects (1.6%) and one infection of the stimulator was unresolved at the study closure.
DISCUSSION
This multicentre, prospective, open label clinical study was conducted in patients who suffered from severe PD or ET. All patients received bilateral stimulation in the STN (104 patients with PD), the VIM (18 patients with ET and 5 with PD), or the GPi (2 patients with PD). The study design focused on the safety and performance of the new Kinetra dual channel stimulator. This device was specifically developed to facilitate bilateral surgical DBS implantation procedures. Clinical evaluations were based on the UPDRS for PD and on the ETRS upper and lower limb tremor subscores for ET. These scores were determined before surgery and three and six months after DBS implantation.
The parameter settings programmed with the Kinetra system were in the same range as those chronically used with the bilateral application of a single channel stimulator (Itrel II).2–25 In ET patients the pulse width tends to be higher with the Kinetra system. Rates of stimulation higher than 185 Hz and other special features of the Kinetra, such as battery checks and control of parameter settings with the patient therapy controller, are not available in the single channel stimulators. Use of the patient therapy controller increases the comfort and independence of the patient, who can control the battery state of the Kinetra and adjust stimulation parameter settings within the physician programmed limits. Furthermore, the Kinetra is easier to use for the physicians, who can control both leads separately with one stimulator.
Previous studies showed an improvement of major contralateral symptoms with STN stimulation in patients with PD11–15 and with VIM stimulation in patients with ET.20–27 Our results confirm that both bilateral STN stimulation in PD and bilateral VIM stimulation in ET are safe and effective treatments for disabling motor symptoms and that they improve activities of daily living. There were too few patients with PD who had leads implanted in the GPi and the VIM to derive conclusions regarding treatment efficacy but safety and adverse events in this small group of patients were included in the analysis reported in this paper. The baseline characteristics of the patients with PD or ET and the improvement in the UPDRS parts II, III, and IV in patients with PD and in the upper and lower limb tremor in patients with ET were comparable with those previously reported.2–28
The surgical technique used to implant the leads, the extension cables, and the Kinetra varies from one centre to another but the main steps were similar to those reported in previously published studies of DBS for movement disorders using single channel stimulators. For neurosurgeons, an advantage of the Kinetra is the potential reduction of operating room time, which for the first time was systematically documented in this study. Use of the Kinetra eliminates one skin incision at the subclavicular level and the need for bilateral subcutaneous tunnelling of the extension cable connecting the DBS lead and the Kinetra.
The adverse events reported in this study were not more severe than those reported in other published studies.3–20 The mortality rate (3%), of which only one death (0.8%) was treatment related, was similar to that reported previously for either unilateral or bilateral surgical procedures irrespective of the target and the disease. Permanent morbidity as a result of surgery and DBS was 3.1% and the frequency of infections 7%. The learning curve for dual channel stimulator related surgical procedures and the larger size and weight of the Kinetra system may explain a trend towards a slightly higher occurrence of surgery related adverse events than that with the single channel stimulators. However, only one procedure is required to implant a dual channel stimulator compared with a single channel stimulator. The size of the dual channel neurostimulator may theoretically increase the risk of cutaneous erosion, previously reported with the single channel system; however, none was reported during this study.3–29 The few technical adverse events reported during this study were not related to battery end of life or to Kinetra malfunction. However, the follow up of the study was shorter than that of other studies in which single channel stimulator battery life or neurostimulator malfunction were reported.26–30 Repeated impedance measurements led to the conclusion that the measurements may not reflect the correct value of the impedance when it is measured with the chronic electrical stimulation parameters, which is the practice for the single channel stimulator. For the Kinetra, consistent electrode impedance is obtained by using standardised stimulation parameters—that is, amplitude 1.0 V, pulse width 210 μs, and frequency 30 Hz. As in other studies of unilateral or bilateral VIM or STN stimulation, most neurological adverse events were related to the baseline medical status of the patient and to the stimulation parameter settings. This last group of adverse events was always reversible when the stimulation parameters were changed.3–30 There were no device failures due to magnetic resonance imaging performed postoperatively. However, this cannot be recommended without specific guidelines.24
In conclusion, the new dual channel stimulator (Kinetra), indicated for the treatment of patients with severe PD or ET, by DBS in either the STN or the VIM is safe and effective. Implantation of the Kinetra device reduces operating room time without increasing adverse events. The Kinetra is easy to use for the patient, the care giver, and the physician.
APPENDIX
The following investigators were members of the Kinetra Study Group: S Chabardes, V Fraix, A Koudsie, A L Benabid, N van Blercom, J Xie, P Pollak (CHU de Grenoble, Grenoble); N Sunde, K Østergaard (Århus Kommunehospital, Århus); J Vesper, U Kestenbach (Universitätsklinikum Benjamin Franklin, Berlin); F Alesch (AKH Wien, Privatklinik Josefstadt, Vienna); V Tronnier, W Fogel (Klinikum der Ruprecht Karls Universität, Heidelberg); G Røste, R Gerdts (Rikshospitalet, Oslo); M Scerrati, A R Bentivoglio (Università Cattolica del Sacro Cuore, Rome); R Figueiras, M Riva (Hospital Ramon y Cajal, Madrid); L Augustinsson, B Johnels (Sahlgrenska University Hospital, Gothenburg); J Villemure, F Vingerhoets (University Hospital, Lausanne); F Ammannati, A Scotto di Luzio (Ospedale Universitario di Careggi, Firenze); J K Krauss, J M Burgunder (Inselspital, Bern); J Lemaire, F Durif (CHU de Clermont Ferrand, Clermont Ferrand); K Ray Chaudhuri, G Hotton (Kings College Hospital, London); J-L Houéto, S Navarro (Hôpital de la Salpêtriére, Paris); D O'Sullivan, M Pell (St Vincent's Clinic, Darlinghurst); I Mendez (Queen Elizabeth II Health Sciences Centre, Halifax).
Acknowledgments
The authors are indebted to the following representatives from Medtronic for their support and helpful comments: Frans Gielen PhD, who participated in the design, management, and analysis of the baseline to 12 month follow up study; Carin Wensing, who was responsible for the management of the long term follow up study and the data analysis; Monique Pirson for the logistics of study management; and Marc Janssens for data and statistical analysis. Parts of the clinical results of 17 patients appear in Oestergaard K, Sunde NA, Dupont E. Effects of bilateral stimulation of the subthalamic nucleus in patients with severe Parkinson's disease and motor fluctuations. Mov Disord 2002;4: (in press).
REFERENCES
Footnotes
-
Competing interests: KO and NS are supported in part by grants from the Novo Nordisk Foundation, the Danish Parkinson Foundation, and Medtronic.