Article Text

Abstract
Objective: To evaluate the effects of a brain tissue oxygen (Ptio2) guided treatment in patients with traumatic brain injury.
Methods: Ptio2 was monitored in 93 patients with severe traumatic brain injury. Forty patients admitted from 1993 to 1996 were treated with intracranial pressure/cerebral perfusion pressure (ICP/CPP) management alone (ICP < 20 mm Hg, CPP > 70 mm Hg). Fifty three patients admitted from 1997 to 2000 were treated using ICP/CPP management, but in this second group CPP was also increased as individually required to raise the Ptio2 above 1.33 kPa (10 mm Hg) (Ptio2 guided group).
Results: Cerebral hypoxic phases with Ptio2 values below 1.33 kPa occurred significantly less often in the Ptio2 guided group. Ptio2 values were higher over the whole monitoring period. No statistical differences could be observed in outcome at six months, despite a positive trend in the Ptio2 guided group.
Conclusions: Cerebral hypoxic events can be reduced significantly by increasing cerebral perfusion pressure as required. To show a clear beneficial effect of Ptio2 guided cerebral perfusion pressure management on outcome, a multicentre randomised trial needs to be undertaken.
- brain tissue oxygen
- cerebral hypoxia
- traumatic brain injury
Statistics from Altmetric.com
Secondary brain damage is a major factor in determining patient outcome following traumatic brain injury.1 Cerebral hypoxia caused by cerebral ischaemia—through impaired autoregulation, systemic hypotension, hypoxia, and intracranial hypertension—has been identified as a principal cause of secondary brain damage.2–6 As a result, the prevention of cerebral hypoxia should result in an improved outcome in patients with traumatic brain injury. In the clinical setting, patients suffering from traumatic brain injury are thus treated by strict avoidance of systemic hypoxia or hypotension. In addition, blood pressure and cerebral perfusion pressure are kept at higher levels than normal in order to provide sufficient cerebral blood flow and avoid cerebral ischaemia in the presence of impaired autoregulation.7 However, despite maintaining a cerebral perfusion pressure of > 70 mm Hg, cerebral ischaemia and hypoxia may still occur, worsening the patient’s chances of a satisfactory outcome.8,9
Measuring the regional partial pressure of brain tissue oxygen (Ptio2) with a polarographic Clark-type probe has proved to be a reliable tool for monitoring cerebral tissue oxygen and detecting secondary cerebral hypoxic insults. Several investigators have reported a significant relation between patient outcome and the duration and frequency of monitored Ptio2 values below the thresholds of 0.67 kPa (5 mm Hg), 1.33 kPa (10 mm Hg), or 2.0 kPa (15 mm Hg).10–13 Furthermore, the Ptio2 monitoring technique provides a high percentage of artefact-free “good quality” data,14,15 is easy to use, and the rate of complications reported so far is very low.16
Our aim in this study was to investigate whether treating cerebral hypoxic episodes following traumatic brain injury by increasing the cerebral perfusion pressure as individually required whenever Ptio2 values fall below 1.33 kPa leads to a reduction in the frequency and duration of cerebral hypoxia; and whether, as a result, this may lead to an improved outcome in such patients.
METHODS
We studied 93 patients suffering from severe traumatic brain injury (Glasgow coma score (GCS) ⩽ 8.17. All patients were treated in the neurosurgical intensive care unit at the Würzburg University Hospital. Patients with multiple trauma were not included. We recorded age, GCS, pupillary response, the incidence of initial shock (hypotension) or hypoxia, and treatment intensity level18 in all patients. The type of injury was classified from the initial computed tomography (CT) according to Marshall et al.19
Neuromonitoring
For advanced multimodal neuromonitoring we used intracranial pressure catheters (Camino Laboratories, San Diego, California, USA) and Ptio2 catheters (Licox Systems, GMS mbH, Kiel, Germany). The catheters were inserted into the brain as soon as possible after the trauma—that is, on the ICU after admission or during emergency craniotomy for haematoma evacuation. They were usually placed in the frontal region of the more severely injured side. In case of a diffuse injury, the right frontal region was chosen. The Ptio2 probes were implanted into normal tissue (on CT examination) at a depth of 22 to 27 mm subdurally. Correct positioning of the Ptio2 probes was checked by routine CT. Further details of the implantation technique have been reported previously.15
Mean arterial pressure was monitored by a catheter inserted into the radial artery and referenced to the foramen of Monro. Data on mean arterial pressure, intracranial pressure, and Ptio2 were digitally sampled at a rate of 4 per minute and stored automatically on a computer. Cerebral perfusion pressure was calculated as mean arterial pressure minus intracranial pressure. Artefacts, which were mainly caused by nursing interventions or by temporary disconnection of catheters because of transport, were eliminated from the datasets manually.
Treatment protocols
To evaluate the effects of a therapeutic regimen using Ptio2 levels above 1.33 kPa (10 mm Hg) as an additional therapeutic target, two separate groups were studied.
ICP/CPP guided group: For the first group of patients (admitted between 1993 and 1996) treatment aimed at keeping intracranial pressure (ICP) below 20 mm Hg and cerebral perfusion pressure (CPP) above 70 mm Hg, with the following options. All patients were sedated, intubated, and ventilated to maintain Pao2 at 13.33 to 16 kPa (100 to 120 mm Hg) and Paco2 ~4.67 kPa (35 mm Hg). Mannitol, vasopressors, volume expansion, and barbiturates were given to keep intracranial pressure under 20 mm Hg and cerebral perfusion pressure above 70 mm Hg. Surgical options in the treatment protocol included the evacuation of haematomas and decompressive craniectomy in case of intractably raised intracranial pressure. Treatment was performed in accordance to the guidelines established by the European Brain Injury Consortium.20
Ptio2guided group: For the second group of patients (admitted between 1996 and 2000) the treatment targets were the same as those for the ICP/CPP guided group but in addition, the avoidance of hypoxic Ptio2 levels of less than 1.33 kPa was attempted. Hypoxic episodes were counteracted by further increasing the cerebral perfusion pressure to the point where Ptio2 values reached 1.33 kPa. This goal was accomplished by increasing vasopressor and fluid intake as individually required. We would like to emphasise that increasing the fraction of inspired oxygen (Fio2) was not used to raise the Ptio2.
The rationale for the study design—with the two groups being investigated in a sequential fashion over several years each rather than randomised—was determined by the development Ptio2 monitoring as a clinical tool. After the introduction of this new technique, an observational study was undertaken in our department in order to gain experience and to define its clinical significance. Based on the analysis and experience of this observational study (ICP/CPP guided group), we found that 1.33 kPa (10 mm Hg) was the threshold for significant cerebral hypoxia,12 and the prospective treatment protocol for the Ptio2 guided group was initiated.
Approval for the use of advanced multimodal neuromonitoring was given by the ethics committee of Würzburg University.
Data analysis
For each patient, median values of intracranial pressure, cerebral perfusion pressure, and Ptio2 were derived from neuromonitoring time series for the whole monitoring period, as well as for each post-trauma day of monitoring. Comparison of daily and whole monitoring medians of both treatment groups was done using the Mann–Whitney U test. Temporary variations in individual parameters for each patient group were analysed using the Kruskal–Wallis test. In addition, frequencies of critical events lasting 30 minutes or more (intracranial pressure > 20 mm Hg, cerebral perfusion pressure < 70 mm Hg, Ptio2 < 1.33 kPa) were derived from pooled data for each treatment group during individual post-trauma days of monitoring, as well as for the whole monitoring period. Comparisons between frequencies of critical v non-critical values for both treatment groups were done using a 2 × 2 table χ2 test.
The two treatment groups were also analysed for differences in outcome using the Glasgow outcome scale (GOS).21 The GOS score was assessed by a neurosurgeon not involved in the study at a follow up examination six months after the trauma.
RESULTS
Of the 93 patients enrolled in the study, 40 were in the ICP/CPP guided group and 53 in the Ptio2 guided group. Clinical data on the two groups are presented in table 1. No significant differences between the groups were seen with respect to age, GCS, pupillary response, injury type, treatment intensity level, and incidence of initial hypoxia or initial hypotension.
Clinical characteristics of the two treatment groups
Neuromonitoring was started significantly earlier after trauma in the Ptio2 guided group (median delay = 12.9 hours) than in the ICP/CPP guided group (median delay = 22.0 hours). The end of monitoring and the time of valid monitoring (that is, where artefact-free data were obtained) did not differ significantly between the groups (table 2).
Median values (with 25th and 75th centiles) of the time interval between the trauma, the start of monitoring, the end of monitoring, and the time of valid monitoring
Analysing the whole monitoring period for each patient, no differences were observed for median intracranial pressure and cerebral perfusion pressure values between the two treatment groups (table 3). In contrast, median Ptio2 values in the Ptio2 guided group (median = 3.55 kPa (26.6 mm Hg)) were significantly higher than in the ICP/CPP guided group (median = 3.07 kPa (23.0 mm Hg); p = 0.03).
Neuromonitoring variables of the two treatment groups for the whole monitoring period
With respect to the critical time intervals, no difference was found in the frequency of cerebral perfusion pressure readings below 70 mm Hg between the ICP/CPP guided group and the Ptio2 guided group (55% v 54%, respectively). Critical intracranial pressure above 20 mm Hg was slightly more common (39% v 30%) in the ICP/CPP guided group. Finally, hypoxic events (Ptio2 < 1.33 kPa) were 2.5 times more frequent (8.5% v 3.4%) in the ICP/CPP guided group than in the Ptio2 guided group (table 3).
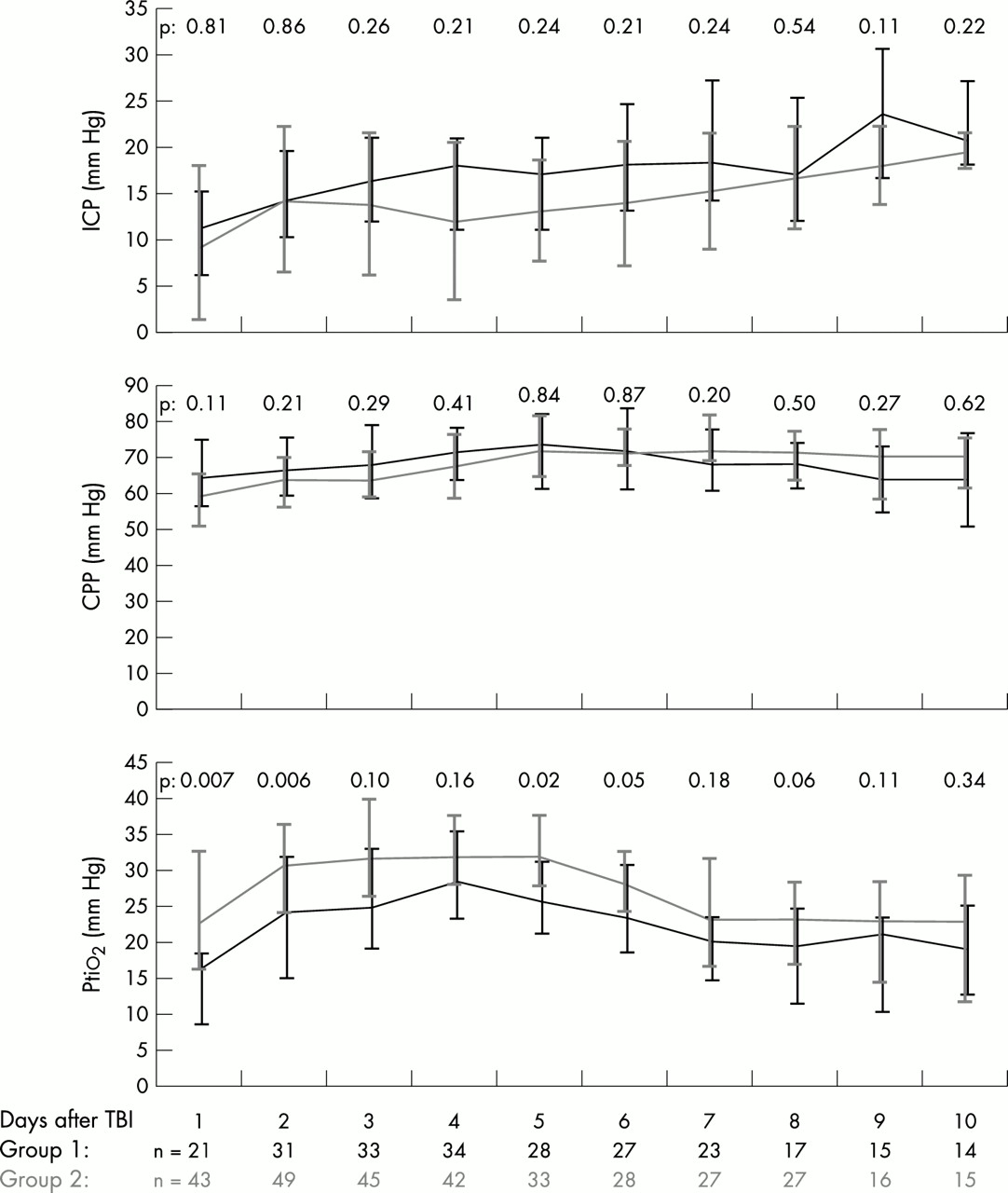
Median daily values of intracranial pressure, cerebral perfusion pressure, and Ptio2 from the first to the 10th day after trauma for both treatment groups are presented in fig 1. For intracranial pressure and cerebral perfusion pressure, differences between the treatment groups did not reach significance. In contrast, Ptio2 values were systematically about 0.53 to 1.07 kPa (4 to 8 mm Hg) higher in the Ptio2 guided group during all days, and differences were significant for days 1, 2, 5, and 6 after the trauma. Both groups showed a similar time course, with the lowest Ptio2 values obtained on the first day after trauma, the maximum values on days 4 and 5 after the trauma, and a return to lower Ptio2 values after day 7 to 10. All variables except cerebral perfusion pressure in the ICP/CPP guided group showed significant temporal variations during the post-trauma period. Note that owing to the variable times of starting and finishing the monitoring, the numbers of patients varied on different post-trauma days.
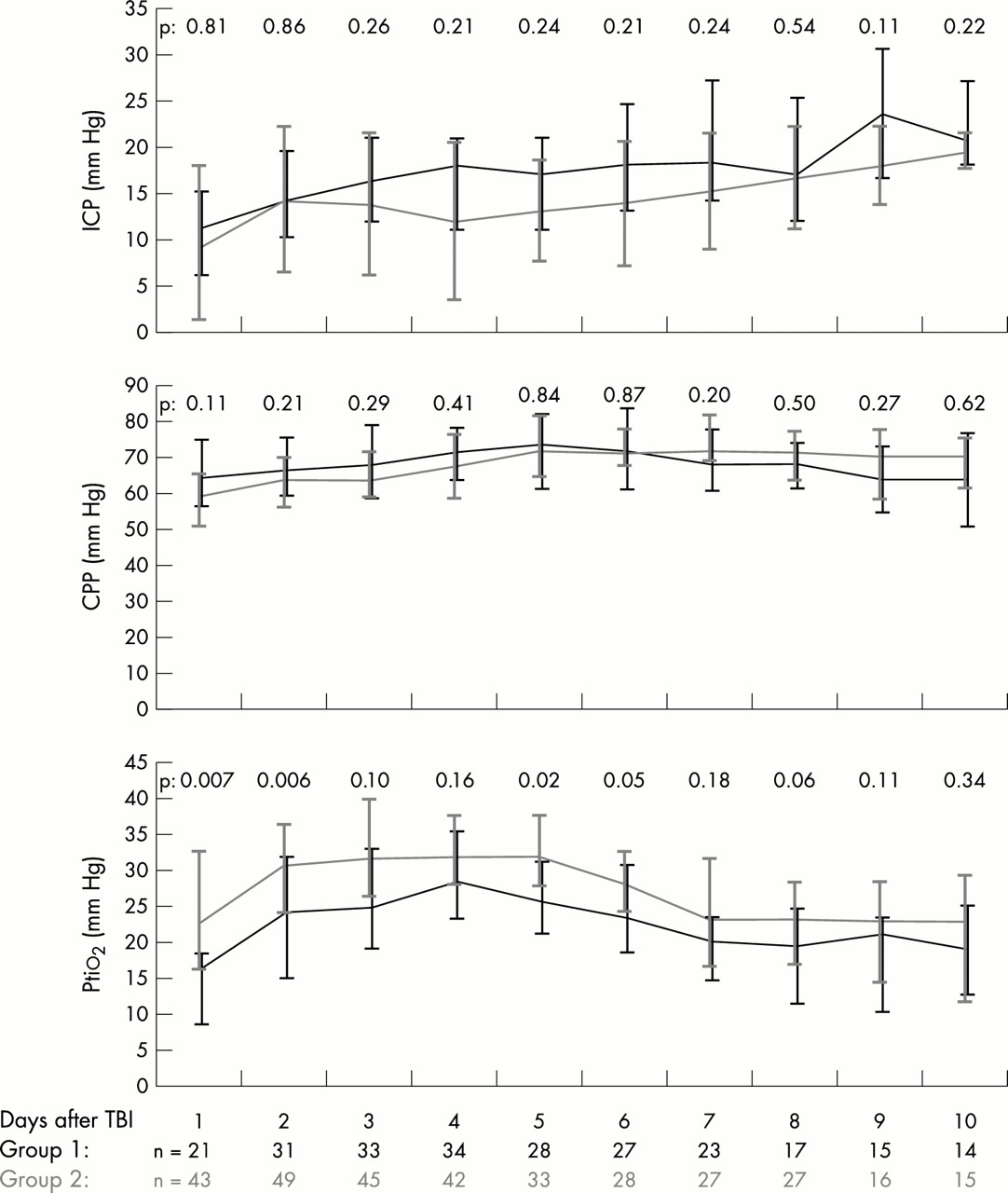
Daily median values of intracranial pressure (ICP), cerebral perfusion pressure (CPP), and brain tissue oxygen (Ptio2) for the ICP/CPP guided group (black line) and the Ptio2 guided group (grey line). Range bars indicate upper and lower quartiles. Significance levels from the Mann–Whitney U test are shown for each variable on each monitoring day. The numbers of patients monitored on each post-trauma day in the two groups are given at the bottom of the figure.
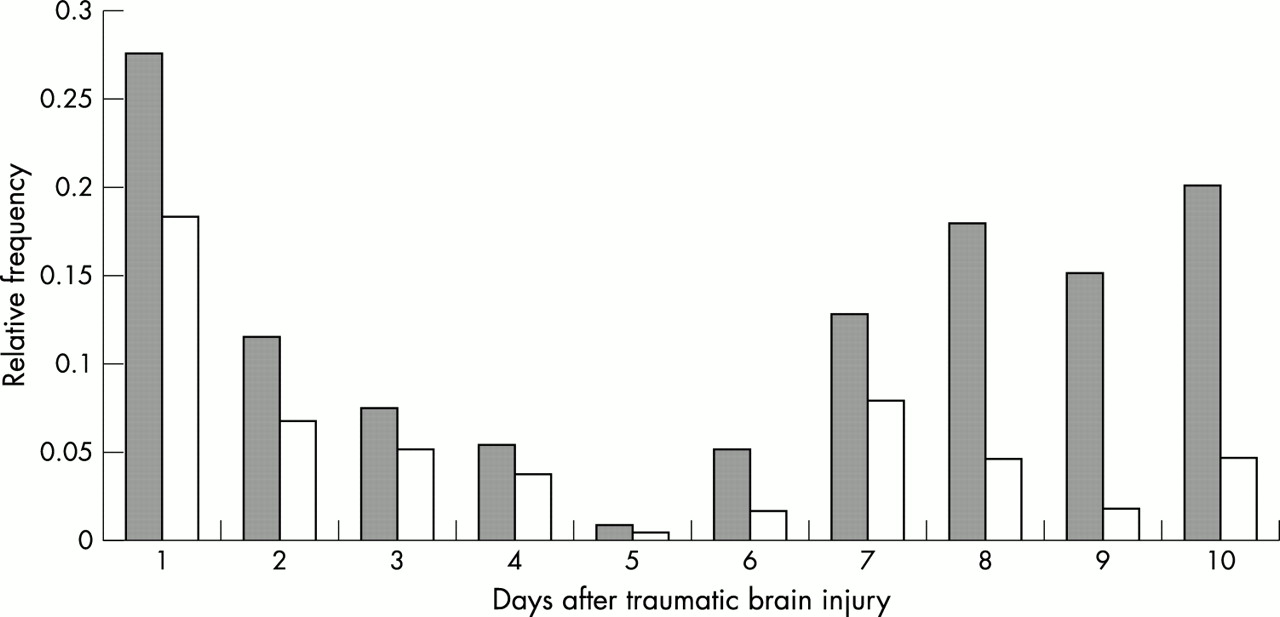
The relative frequency of hypoxic Ptio2 events of 30 minutes’ duration in the post-trauma period (fig 2) was almost inversely related to the time course of the median Ptio2 values. In both treatment groups, the frequency of hypoxic events was highest on the first post-trauma day, decreased to almost zero on the fifth post-trauma day, and increased again after six days. For all but the fourth and the fifth post-trauma days, the frequency of hypoxic Ptio2 was significantly higher in the ICP/CPP guided group.

{kind=link}
{kind=link}
Relative frequency of hypoxic events (Ptio2 < 1.33 kPa (10 mm Hg)) lasting ⩾ 30 minutes for the ICP/CPP guided group (grey columns) and the Ptio2 guided group (white columns) on each post-trauma day. CPP, cerebral perfusion pressure; ICP, intracranial pressure.
Outcome
To analyse the clinical outcome after six months, both treatment groups were divided into a poor outcome (GOS = 1–3) and a good outcome group (GOS = 4–5). In each group, one patient was lost to follow up. There was an increased proportion of patients with a good outcome in the Ptio2 guided group (65% v 54%) where Ptio2 was used as an additional monitoring parameter to avoid cerebral hypoxia (table 4).
Outcome after six months for the two treatment groups
DISCUSSION
The treatment of Ptio2 values below 1.33 kPa (10 mm Hg), a level indicating cerebral hypoxia, was successful in reducing secondary hypoxic insults following severe traumatic brain injury. The frequency of critical hypoxic phases with a Ptio2 under 1.33 kPa lasting for more than 30 minutes was reduced on all post-trauma days. In order to achieve this, the cerebral perfusion pressure was increased as individually indicated to raise the Ptio2 above 1.33 kPa. In addition, with this therapeutic approach of Ptio2 targeted cerebral perfusion pressure management, the median Ptio2 values over the whole monitoring period were significantly higher in the Ptio2 guided group than in the ICP/CPP guided group.
As described by other investigators, our data provide evidence of a time course of Ptio2 values over the various post-trauma days.11,22 In the first 24 hours after the impact, Ptio2 values are lowest, indicating a high risk of ongoing brain damage immediately after trauma. However, treatment of low Ptio2 values by raising cerebral perfusion pressure is highly successful in reducing early hypoxic episodes. After this critical early phase, cerebral oxygenation approaches normal values by days 4 and 5. From days 7 to 10, the frequency of hypoxic episodes increased again in our datasets. We are not sure whether this triphasic pattern is representative of the situation in all our patients, as advanced multimodal neuromonitoring was carried out only as long as was clinically indicated, and by day 9 the number of patients monitored had decreased to 15 and 16 in groups 1 and 2, respectively. Thus the data from days 9 and 10 refer to the more severely ill patients, who still require close observation even after more than a week after the injury. However, such a triphasic response might well reflect the patterns of post-traumatic cerebral blood flow alterations found previously.23,24
Recent reports indicate that the long term outcome in patients suffering from traumatic brain injury is mainly determined by cerebral protection.25 However, associated injury and other systemic factors have a powerful impact on secondary cerebral damage.26 As demonstrated recently in a large trial, the benefits of treating patients with traumatic brain injury by aggressively increasing their cerebral perfusion pressure to avoid cerebral ischaemia may be offset by the adverse systemic effects of this treatment strategy.27 Induced pulmonary failure is of special concern. The use of vasopressor agents and a high fluid input have been identified as major risk factors for severe pulmonary complications.28 This contrasts with current therapeutic concepts, where vasopressors and fluids are the cornerstones of maintaining a cerebral perfusion pressure of more than 70 mmHg. In this context, Ptio2 guided cerebral perfusion pressure management may help to reduce unnecessarily high cerebral perfusion pressures by limiting the perfusion pressure to that necessary to ensure adequate oxygenation. Future research should focus on the use of Ptio2 as an indicator of sufficient cerebral blood flow at perfusion pressures below 70 mm Hg. The use of Ptio2 guided cerebral perfusion pressure management should help to establish a satisfactory regimen tailored to the needs of the individual patient.
From today’s understanding of the pathophysiology of traumatic brain injury, cerebral autoregulation is impaired to an unknown extent after trauma, and thus the brain is very susceptible to secondary ischaemic insults. Increases in cerebral perfusion pressure are thought to improve cerebral blood flow and cerebral oxygenation. However, despite these conclusions, Ptio2 in the acutely injured brain can be manipulated not only by variations in cerebral perfusion pressure but also by simply changing the Fio2. Increasing Fio2 to 1.0 will result in an increase of oxygen dissolved in the plasma, though this accounts for only 2–3% of the oxygen transport in the blood with haemoglobin saturated to 100%. Nevertheless, recent research has reported improved brain tissue oxygenation with aggressive management of Fio2 (= 1.0) following traumatic brain injury.29 This interesting finding needs to be validated in future research, because it might play an important role in supporting oxygen delivery to the injured brain and in improving treatment results. However, the hazards of ventilation with high Fio2—for example, hyperoxia induced lung injury—will have to be carefully balanced against possible beneficial cerebral effects.
With respect to outcome, the successful reduction of cerebral hypoxia did not translate into a statistically significant improvement six months after the trauma. There was a tendency for a better outcome in the Ptio2 guided group, with 65% good outcome v 54% in the ICP/CPP guided group, but because treatment was probably started earlier in the Ptio2 guided group—as indicated by the shorter interval between the trauma and start of monitoring (table 2)—this might well explain any observed trends towards an improved outcome in the Ptio2 guided group. Furthermore, owing to the severe nature of the injury, differences in outcome are expected to be rather minor, and thus the number of patients is rather small to allow reliable assessment of an improved outcome in our cohorts. Still, the promising results of Ptio2 guided cerebral perfusion pressure management in reducing cerebral hypoxic events justify further clinical evaluation, ideally in the form of a multicentre trial.
As Ptio2 monitoring is gaining increasing acceptance among head injury centres, a critical comparison with the well established technique of intracranial pressure monitoring in neurosurgical critical care seems opportune. As stated in the guidelines of the American Brain Trauma Foundation, the monitoring of raised intracranial pressure and its treatment have not yet been proven to be efficient when applying the standards of evidence based medicine.30 Despite a large amount of data indicating the beneficial effects of managing intracranial pressure, there is still no definite proof that this affects the outcome after brain injury. As mentioned, only a randomised multicentre trial with more than 700 patients would produce the data necessary to meet today’s requirement for evidence based practice. Such a trial is almost impossible to carry out, as intracranial pressure monitoring has become an integral part of today’s neurointensive care monitoring. With the introduction of a new treatment approach for traumatic brain injury based on the relatively new technique of monitoring brain tissue oxygenation, it is important to demonstrate the therapeutic value of the procedure at an early stage, in conjunction with intracranial pressure monitoring, before its use has become generalised. We therefore feel that a randomised multicentre trial is desirable to avoid the uncertainty that we still have to face with respect to the use of intracranial pressure monitoring.
Conclusions
This trial showed that Ptio2 guided cerebral perfusion pressure management is successful in reducing cerebral hypoxic episodes following traumatic brain injury. Lack of significant improvement in neurological outcome may reflect the relatively small patient cohorts. With the possibility that Ptio2 guided cerebral perfusion pressure management will reduce secondary brain damage and the systemic side effects of ICP/CPP management, a multicentre trial is desirable to demonstrate the effects on outcome.
REFERENCES
Footnotes
-
Competing interests: none declared