Article Text

Abstract
Objectives: To describe functional recovery after surgical resection of low grade gliomas (LGG) in eloquent brain areas, and discuss the mechanisms of compensation.
Methods: Seventy-seven right-handed patients without deficit were operated on for a LGG invading primary and/or secondary sensorimotor and/or language areas, as shown anatomically by pre-operative MRI and intraoperatively by electrical brain stimulation and cortico-subcortical mapping.
Results: Tumours involved 31 supplementary motor areas, 28 insulas, 8 primary somatosensory areas, 4 primary motor areas, 4 Broca’s areas, and 2 left temporal language areas. All patients had immediate post-operative deficits. Recovery occurred within 3 months in all except four cases (definitive morbidity: 5%). Ninety-two percent of the lesions were either totally or extensively resected on post-operative MRI.
Conclusions: These findings suggest that spatio-temporal functional re-organisation is possible in peritumoural brain, and that the process is dynamic. The recruitment of compensatory areas with long term perilesional functional reshaping would explain why: before surgery, there is no clinical deficit despite the tumour growth in eloquent regions; immediately after surgery, the occurrence of a deficit, which could be due to the resection of invaded areas participating (but not essential) to the function; and why three months after surgery, almost complete recovery had occurred. This brain plasticity, which decreases the long term risk of surgical morbidity, may be used to extend the limits of surgery in eloquent areas.
- direct electrical stimulations
- functional mapping
- low grade glioma
- plasticity
- IES, electrical stimulations
- LGG, low grade gliomas
- NFI, neurofunctional imaging
- SMA, supplementary motor area
Statistics from Altmetric.com
- IES, electrical stimulations
- LGG, low grade gliomas
- NFI, neurofunctional imaging
- SMA, supplementary motor area
Resection of infiltrative tumours such as low grade gliomas (LGG) that are located in eloquent brain areas remains a neurosurgical challenge. Although many studies show that the quality of life and the median survival in LGG seems correlated to the extent of resection,1–6 the role of resection remains unproven.3 Additionally, resection of these tumours, with no clearly defined boundaries and often occurring in functional regions, carries a high risk (13–19.7%) of permanent deficit.7–9 The development of methods of pre-operative neurofunctional imaging (NFI)10–14 and intra-operative electrical stimulations (IES)2,15–21 functional mapping has allowed the identification and the organisation of specific brain regions. These techniques can be used to decrease the risk of complications following surgical resection of tumours in eloquent brain. However, if brain functions are considered to remain in their classical anatomical locations, and these locations are infiltrated by tumour, then excision of the tumour will either be considered impossible or result in an unacceptable postoperative morbidity.19 Given the brain plasticity and functional compensation seen after stroke,22,23 with congenital malformations24,25 or following brain injury, we hypothesise that brain infiltration by gliomas leads to reshaping or local reorganisation of functional networks. This would explain the frequent lack of clinical deficit despite LGG growing in eloquent brain areas,27–29 and also the transient nature of post-operative deficits. To illustrate the background to this hypothesis we describe our experience and observations of functional recovery in patients having resection of LGG from eloquent brain regions.
PATIENTS AND METHODS
Between November 1996 and June 2001, a consecutive series of 77 patients had resection of LGG, with IES, from secondary and/or primary functional brain areas. This series comprises 37 males and 40 females (mean age 37 years) who all presented with seizures and a normal neurological examination (except a mild dysphasia in three cases). A neuropsychological evaluation using a standardised questionnaire30 showed that all the patients were right handed.
Pre-operative MRI showed a tumour involving the supplementary motor area (SMA) in 31 cases (9 right, 22 left), the insular lobe in 28 cases (20 right, 8 left), the primary somatosensory area (S1) in eight cases (5 right, 3 left), the primary motor area (M1) in four cases (three non-dominant facial regions—in one case with also infiltration of S1 of the face—and one hand/forearm left site), Broca’s area in four cases (pars opercularis Brodman Area (BA) 44, pars triangularis (BA 45), and the left dominant temporal lobe in two cases.
All surgical procedures used IES (5 mm spaced tips bipolar electrode, biphasic current with pulse duration of 1 ms, frequency of 60 Hz, intensity of 4 to 18 mA, Ojemann Cortical stimulator, Radionics*).17,18 The patients harboring tumours involving the right supplementary and primary motor areas, and the right insular lobe underwent surgery under general anaesthesia, with cortical and sub-cortical IES allowing the detection of the whole cortico-spinal pathways.31 Although the motor mapping definition might be considered as not very accurate under general anaesthesia, particularly in subcortical regions, we have recently shown the effectiveness of such a technique,32 without “awake surgery”. Conversely, the patients with left and somatosensory tumours were operated under local anaesthesia with performance of intraoperative sensorimotor and language mappings.18 We never used the technique of extraoperative mapping after placement of subdural grid. Ultrasonography and/or image guidance were used to show the anatomical limits of the tumour. We found the former more useful because of a major brain shift seen during extensive resections.
The 77 patients were examined immediately and three months after the surgery by the same neurologist. An immediate and delayed (three months) post-operative MRI was performed to evaluate the quality of resection.
RESULTS
The clinical, radiological, and surgical data of the 77 patients are summarised in table 1. In surgery of medial precentral LGG, the resection was continued posteriorly until the primary motor pathways were detected by cortico-subcortical IES, thus incorporating total SMA removal (fig 1). Laterally, in left LGG, the resection was pursued up to the language structures, notably the head of the caudate nucleus and corresponding white fibres deeply.18 No response was elicited during SMA IES. All patients had an immediate post-operative SMA syndrome, with controlateral motor deficit in the 31 cases, and speech disorders in the 22 left LGG. A complete recovery was seen within 1–3 months, in all except one patient with residual right lower limb monoparesia (there was an infiltration of M1 associated with the invasion of SMA). Two patients with a mild preoperative dysphasia improved.
Clinical, radiological, and surgical characteristics of the 77 patients (37 males, 40 females; mean age 37 years) with resection in a glioma in secondary and/or primary functional brain areas

(A) Preoperative axial and sagittal T1-weighted MRI, showing a right medial precentral low grade glioma, involving the supplementary motor area. The neurological examination was normal. (B) Intraoperative photograph after tumour removal. The primary motor cortical sites (marked by numbers from 1–7) and their corresponding descending cortico-spinal pathways, both identified using electrical stimulations, represented the posterior functional boundaries of the resection. A, anterior; P, posterior; M, midline. (C) Postoperative axial and sagittal T1-weighted MRI, showing a total glioma removal, with resection of the supplementary motor area (the posterior edge of the surgical cavity comes into the contact with the paracentral area). The patient had an immediate post-surgical hemiplegia, then completely recovered within one month.
During right insular glioma removal, the resection was conducted up to the internal capsule identified by sub-cortical IES, thus with a total removal of the insula and most of the time of a part of the lentiform nucleus (fig 2). There was no motor response elicited by insular IES. In left LGG, the insular resection was incomplete in six out of the eight cases, due to the induction of a speech arrest during dominant insula IES (fig 3). Complete insular tumoural removal was possible in two cases because there was no language disturbance during IES. All patients with right LGG had a post-operative motor deficit (10 total hemiplegias, 10 moderate hemiparesis), with complete recovery within three months except in three cases (persistant hemiparesis due to vascular injury shown by post-operative MRI). Patients with left LGG had transient mild speech disturbances in seven cases, whilst one patient had an improvement of the preoperative dysphasia (one of the two cases with total removal). There were no motor deficits.

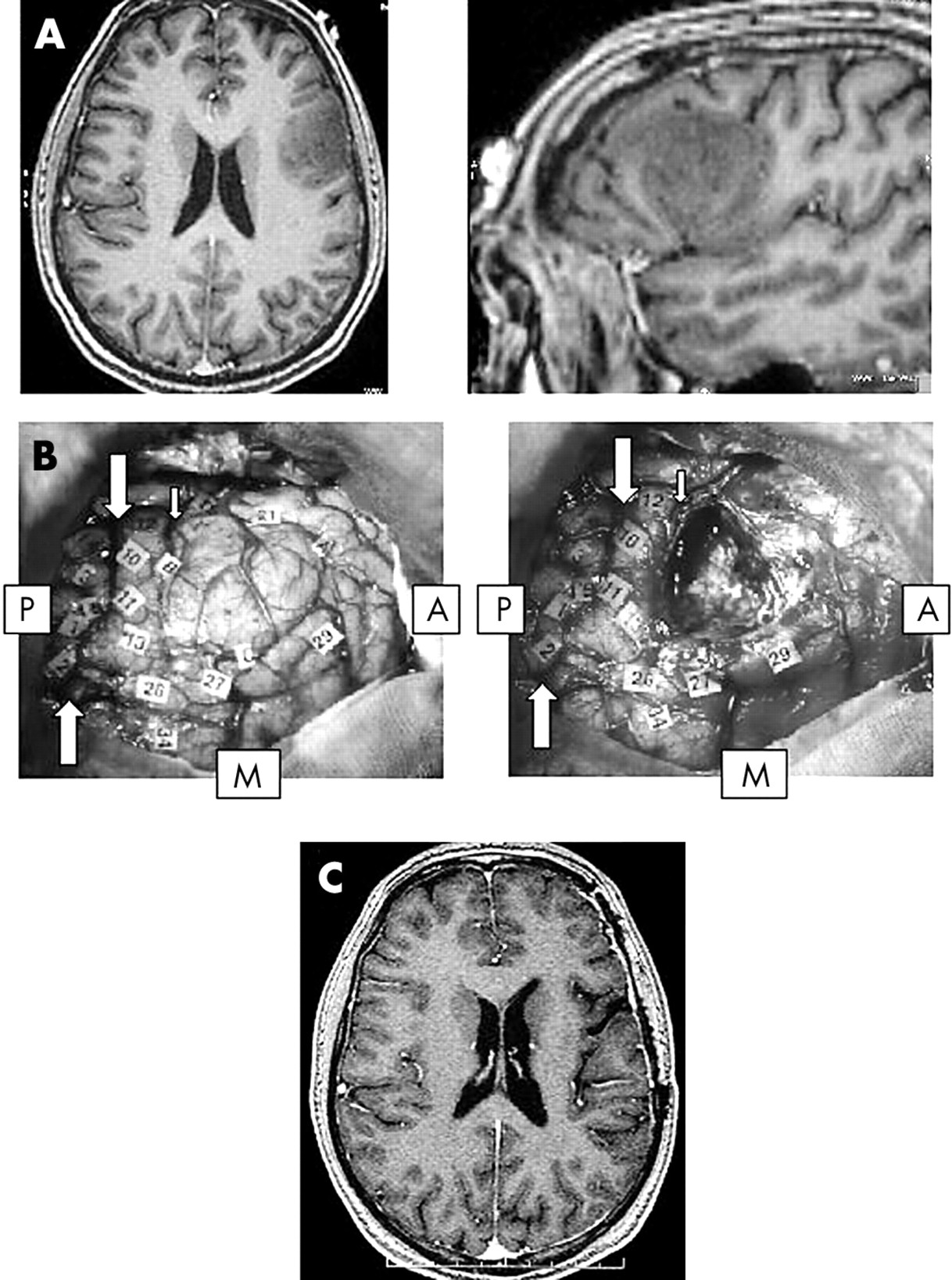
(A) Preoperative axial and coronal T1-weighted MRI, showing a right temporo-insular low grade glioma. The neurological examination was normal. (B) Intraoperative photograph after tumoural removal. The primary motor cortical sites (marked by the tags on the frontal cortex) were preserved, and their corresponding descending cortico-spinal pathways were identified and followed from the corona radiata to the brain stem all along the internal capsule, using electrical stimulations: these motor fibres represented the deep functional boundaries of the resection (numbers 11 and 12, under the sylvian vessels (arrow)). A, anterior; P, posterior; M, midline. (C) Postoperative axial and coronal T1 weighted MRI, showing a total glioma removal, with resection of the entire right insular lobe. The patient had an immediate post-surgical hemiparesia, then completely recovered within three months.

Preoperative axial T2 weighted MRI, showing a left fronto-insular low grade glioma, in the dominant hemisphere. The neurological examination was normal. (B) Left photograph: Intraoperative view before tumour removal. The glioma boundaries were defined using ultrasonography, and marked by letter tags. The eloquent cortical sites identified using electrical stimulations were marked by numbers as follows: 7, primary motor area of the face; 8, primary somatosensory area of the face; 10, language site, inducing anarthria during stimulation; 11, language site, inducing speech arrest during stimulation. Right photograph: Intraoperative view after tumour removal. The eloquent cortical sites were preserved (7,8,10,11). However, following the operculum resection, the stimulations of the left dominant insular lobe induced speech arrest (20), leading to stop prematurely the glioma removal. A, anterior; P, posterior; M, midline. (C) Postoperative axial T1 weighted MRI, showing a partial glioma removal—that is, with resection of the left frontal operculum, but preservation of the left dominant insular lobe despite its tumoural invasion. The patient had immediate post-surgical speech disturbances, then completely recovered within three months.
In surgery of LGG involving the retrocentral gyrus, primary somatosensory sites were systematically detected by IES within the tumour. However, during glioma removal, repetitive cortical mappings performed with the same electrical parameters allowed the detection of several somatosensory sites that induced the same sensitive responses. These “unmasked”, or extra-tumoural sites were located within the postcentral gyrus, but more laterally or medially than the intratumoural sites. The primary areas invaded by the glioma were then removed up to the corticospinal tracts anteriorly. All eight patients had a severe post-operative sensory loss, but recovered within three months, with mild residual dysesthesias in two cases (allowing a return to normal life).
In the three LGG invading the right lateral precentral gyrus, M1 of the face was identified within the tumour, and totally removed, since the precentral gyrus resection was continued medially until the hand cortico-spinal pathways were detected by IES. In one case, S1 of the face was also removed because it was invaded by the tumour (fig 4). All three of these patients had a central facial palsy that recovered completely within month. The patient who had resection of both M1 and S1 had a transient hypophonia.

(A) Preoperative axial and coronal T1-weighted MRI, showing a right central supra-sylvian low grade glioma. The neurological examination was normal. (B) Intraoperative photograph after tumour removal. The primary motor cortical sites of the hand (marked by the tags 1 and 2) were preserved, and their corresponding descending cortico-spinal pathways were identified and followed all along the corona radiata (27, 26, 25), using electrical stimulations. Since these motor fibres of the superior limb represented the deep functional boundaries of the resection, it means that the entire primary sensorimotor area of the face (detected by stimulations within the tumour before its resection) was totally removed. A, anterior; P, posterior; M, midline. (C) Postoperative axial and coronal T1 weighted MRI, showing a total glioma removal, with resection of the rolandic operculum. The patient had an immediate post-surgical central facial palsy with hypophonia, then completely recovered within one month.
In the patient with a left central LGG invading M1 of the hand/forearm, the detection of a primary motor site within the lesion (with controlateral superior limb response during IES) led to cessation of the resection, despite the unmasking of “redundant” motor sites identified by repetitive intraoperative mappings. Two years later, during a second surgery for tumour recurrence, a functional reorganisation of the motor map without any eloquent site within the glioma was observed using IES, and allowed the performance of a total tumoural removal—for example, with resection of a part of the precentral gyrus. The patient had a post-operative monoplegia (right upper limb), but totally recovered within two weeks.
During the removal of the four LGG invading Broca’s area (BA 44, BA 45), the limits of resection were represented by the language areas which elicited speech arrest when stimulated, and located around but not within the tumour—that is, in the precentral gyrus, the middle frontal gyrus, and in the pars orbitaris of the inferior frontal gyrus (fig 5). Interestingly, these four patients had only slight transient speech disturbances after surgery, with total recovery within a few days.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Preoperative axial and sagittal T1 weighted MRI, showing a left fronto-opercular low grade glioma (dominant hemisphere), invading pars opercularis (BA 44) and pars triangularis (BA 45) of the inferior frontal gyrus. The neurological examination was normal. (B) Left photograph: Intraoperative view before tumour removal. The glioma boundaries were defined using ultrasonography, and marked by letter tags (A, B, C). The eloquent cortical sites identified using electrical stimulations were marked by numbers as follows: 1, 2, 3, 5: primary somatosensory area of the face, within the retrocentral gyrus; 10, 11, 13: language sites, inducing anarthria during stimulation, within the precentral gyrus; 26, 27, 29, 34: language sites, inducing anomia during stimulation, within the middle frontal gyrus—the more anterior site at the level of the BA 46; 21: language site, inducing speech arrest during stimulation, in the pars orbitaris of the inferior frontal gyrus (BA 47). No eloquent site was found within the pars opercularis and pars triangularis of the left inferior frontal gyrus, e.g. Broca’s area. Right photograph: Intraoperative view after tumour removal. All the eloquent cortical sites were preserved, with resection of the entire pars opercularis and pars triangularis of the left inferior frontal gyrus. A, anterior; P, posterior; M, midline; large arrows: central sulcus; small arrow: precentral sulcus. (C) Postoperative axial T1 weighted MRI, showing a total glioma removal, with resection of the Broca’s area. The patient had immediate post-surgical slight speech disturbances, then completely recovered within one week.
Finally, in two left temporal LGG, language (naming) sites were detected within the posterior part of the tumour, leading to incomplete tumour resection. Several months later, during a second procedure for recurrence, the intraoperative cortical mapping did not find any language area either within or around the tumour, allowing total LGG removal. The patients had a post-operative dysphasia that was more severe than after the first procedure, but recovered in three months.
In summary, all patients had post-operative complete or partial deficits, that recovered in all except four cases (overall definitive morbidity 5%). The 73 other patients returned to a normal life.
Postoperative MRI assessment of extent of glioma removal was according to the classification described by Berger et al,1 either total (no signal abnormality on T1, T2, and SPGR-weighted MRI) or subtotal (less than 10cc of residual tumour) in 92% (71 patients ), and partial in 8% (six patients) (left insular gliomas). Histological examination confirmed WHO Grade II gliomas in all cases.
DISCUSSION
The preoperative findings and postoperative results suggest a dynamic spatio-temporal re-organisation of the focal brain functions can be induced by LGG. This hypothesis would explain:
1. Preoperative functional compensation:
The lack of deficit despite a growing tumour in eloquent regions may be explained by the recruitment of compensatory areas—most of the time incorporating local brain sites around the LGG. This is suggested by preoperative NFI.28,29,33–35 We have already reported, using both fMRI and IES, the brain’s ability to compensate for speech function in the dominant insula, infiltrated by tumour, by recruiting the left superior temporal gyrus and left putamen.27 We have also observed, using IES, a reorganisation of the language sites around the Broca’s area (BA 44, BA 45), when invaded by LGG (fig 5). Thus, functional compensation is related to recruitment of adjacent regions—for example, the precentral cortex, the middle frontal gyrus, and the inferior frontal gyrus (pars orbitaris BA 47). Interestingly, these four patients had only slight transient speech disturbances after surgery, with total recovery in only a few days. This transient deficit may be explained by the preoperative reorganisation of language functions. Our data seem in accordance with NFI results, since recent PET data have shown that even limited salvage of peri-infarct tissue after acute stroke treatment can have an important impact on the rehabilitation of cognitive function.36 More specifically, Thiel et al37 suggested in cases of brain tumours invaded dominant BA 44 and BA 45 (as in our patients), a functional replacement of these areas by other left fronto-lateral regions such as BA 46 and BA 47.
However, eloquent structures may persist within LGG. Indeed, paresthesias were induced during S1 IES despite its tumoural invasion in eight patients, and motor face responses were elicited during M1 IES involved by LGG in three patients. Moreover, the speech arrest induced by the left insular cortex IES in six patients, means that a dominant insular lobe entirely infiltrated by a LGG still retains essential language functions (fig 3). Our findings confirm previous reports which detected eloquent areas within tumours (in 7% to 24% of cases) using preoperative NFI38,39 or IES.16,40,41 These data, likely explained by the Type III spatial configuration of the LGG in the Daumas-Duport’s classification,42 suggest the persistence within the tumour not only of eloquent neural networks, but also of functional astrocytes and intact neuron-glial interactions.43,44 Thus, for the neurosurgeon, the difficult question is to know if eloquent functions can be compensated after removal of functioning “brain” tissue, whilst the basic neuroscientist is interested in the mechanisms underlying such compensation.
2. Intraoperative functional reshaping
Repetitive IES unmasked several brain regions that performed the same function in patients with LGG involving S1, and M1 of the upper limb.45,46 These findings show the existence of multiple cortical representations or “functional redundancy” within the primary sensorimotor area, and the human brain’s ability to rapidly reorganise its motor map, as seen in animals.47 The surgical act itself might induce this reshaping, by generating an hyperexcitability due to changes in the ratio of Gaba:NMDA receptors,45 previously described in brain injuries.48–50 Indeed, since LGG resection implies removal of functional glio-neuronal structures, this resection might generate changes in neurono-synaptic networks by modulating inhibitory and/or excitatory inputs, as observed using transcranial magnetic stimulations (TMS).51 Thus, we may consider that this short term plasticity can lead to a long term plasticity, as supported by the results of IES in the patients reoperated on several months later, showing modifications of the motor and language maps. These phenomena could explain the postoperative functional recovery.52
3. Postoperative functional compensation
The main point of this paper is that secondary and even primary eloquent areas may be removed without inducing a definitive deficit. This postsurgical functional compensation could be due to brain plasticity, as in stroke and other injuries.22,23,26,53–55 Indeed, the immediate post-operative deficit observed in all patients confirms that some structures remain functional within the tumour mass or peri-tumoural brain, because this deficit is too prolonged to be explained by a simple edema, despite a possible preoperative loco-regional reshaping due to LGG.28,29,33–35 Immediately after surgery, this peritumoural reorganisation is insufficient to maintain function, more so if parts of the “reorganised” brain tissue around the tumour cavity has been transitorily damaged by the surgical trauma itself. Subsequent postoperative development or a reinforcement of this loco-regional mechanism of reshaping and/or the recruitment of remote areas might explain the secondary recovery.56 The delay of this recovery (1–3 months) could reflect that neosynaptogenesis, combined with sprouting of axons and dendritis to loco-regional and remote regions, may represent the main plasticity mechanism, as described in vitro and in animals.47,57,58
On the basis of the NFI results in recovery after stroke,22,23,26,53–55 the regions recruited to compensate following resection of eloquent brain invaded by a LGG can be considered for each secondary or primary functional brain area.
SMA resection
We showed that the occurrence of the SMA syndrome59–61 was spatially62 and temporally63 due to the removal of the SMA proper.64 We currently perform postoperative fMRI after SMA syndrome recovery: the preliminary results argue in favour of a compensation by the controlateral SMA,65 and also by M1 (explaining the lack of complete recovery in one patient of our series, due to the associated invasion of the paracentral area).
Insular resection
We already showed that the left insula, known to play a key role in language,66 could be compensated by the left opercula and lentiform nucleus.27 This compensation seems possible only when the opercula are not invaded, explaining the total left insular resection in the two LGG type IIIA of Yasargil,67 but the partial resection in the six other left paralimbic LGG (with invasion of the insula and the opercula—type IIIB of Yasargil).31 Concerning the motor function, despite an hemiparesis after insula removal, likely because this region is a non-primary motor area,68 all patients recovered (except three due to vascular injury), which could be explained by the recruitment of other non primary motor areas, strongly connected with the insular lobe.68
S1 resection
The first results using pre- and post-operative MEG suggest the possible recruitment of “redundant” eloquent sites around the cavity, within the postcentral gyrus.69 This is in accordance with the IES data, showing unmasking of redundant somatosensory sites during resection, likely explained by the decrease of the cortico-cortical inhibition.70 The recruitment of the second somatosensory area or posterior parietal cortex,71 M1 (due to strong anatomo-functional connections between the pre- and retro-central gyri),45,72 and the controlateral S173,74 should also be considered.
Resection of non-dominant M1 of the face
The recovery of the central facial palsy and hypophonia (already described in opercular syndrome due to cortical or subcortical lesion,75 and—in our experience—may be due to the resection of both M1 and S1 of the face) is likely explained by the disinhibition of the controlateral homologous sites, via the transcallosal pathways.76
Resection of M1 of the upper limb
If we hypothesise the existence of multiple cortical representations, observed in animals,77 in humans using fMRI,78 and IES,46 the compensation of the motor function could be explained by the recruitment of parallel networks within M1—allowing the superior limb area removal during a second surgery, since the initial rapid reshaping could be durable.79
Broca’s area resection
The language compensation may be underlied by the recruitment of adjacent regions (in particular BA46 and BA47). Moreover, Broca’s could be not systematically essential for language, as suggested by recent NFI studies in healthy volunteers.80
Temporal language area resection
In the light of fMRI results after recovery from aphasia due to stroke,36,81 language compensation following left dominant temporal resection could be explained by the fact that this function seems to be organised with multiple parallel networks.82,83 Consequently, beyond the recruitment of areas adjacent to the surgical cavity, the long term reshaping (between two surgeries) could be related to progressive involvement of, firstly, remote regions within the left dominant hemisphere—such as the posterior part of the superior temporal gyrus,84,85 the triangular part of inferior frontal gyrus86 or other left frontolateral regions (BA 46 and BA 47)37 and, secondly, the controlateral right non-dominant hemisphere87–89 due to a transcallosal disinhibition phenomenon.37
However, despite this brain plasticity, mechanisms of compensation are limited, explaining why previous studies of such patients reported irreversible deficits. Firstly, it would seem that reorganisation would be of more importance in secondary than in primary areas. Secondly, if a damaged area is compensated by another region, a lesion of this recruited region will induce a permanent deficit. Consequently, surgical resection should avoid involvement of an eloquent structure if its compensatory area(s) is (are) not perfectly functional (notably if infiltrated by tumour or also removed): this explains why one patient did not completely recover following SMA resection, due to the combined invasion by LGG of M1 of the lower limb (lesion of both secondary and primary eloquent structures).