Article Text

Abstract
Objectives: The aim of this study was to evaluate the influence of total drainage time on the risk of catheter infection, and the predictive value of standard laboratory examinations for the diagnosis of bacteriologically recorded cerebrospinal fluid (CSF) infection during external ventricular drainage.
Methods: During a three year period, all patients of the neurosurgical intensive care unit (ICU), who received an external ventricular drain, were prospectivly studied. Daily CSF samples were obtained and examined for cell count, glucose and protein content. Bacteriological cultures were taken three times a week, and serum sepsis parameters were determined.
Results: 130 patients received a total of 186 external ventricular drains. The ventricular catheters were in place from one to 25 days (mean 7.1 days). In 1343 days of drainage, the authors recorded 41 positive bacteriological cultures in 21 patients between the first and the 22nd drainage day (mean 6.4). No significant correlation was found between drainage time and positive CSF culture. The only parameter that significantly correlated with the occurrence of a positive CSF culture was the CSF cell count (unpaired t test, p<0.05).
Conclusions: Drainage time is not a significant risk factor for catheter infection. Increasing CSF cell count should lead to the suspicion of bacteriological drainage contamination. Other standard laboratory parameters, such as peripheral leucocyte count, CSF glucose, CSF protein, or serum sepsis parameters, are not reliable predictors for incipient ventricular catheter infection.
- ventricular drainage
- infection
- CSF cell count
- CSF, cerebrospinal fluid
- ICU, intensive care unit
Statistics from Altmetric.com
External ventriculostomy for cerebrospinal fluid (CSF) drainage or for intracranial pressure monitoring is frequently used in intensive care unit (ICU) patients. For these patients, the risk of CSF infection caused by a contaminated ventricular catheter is reported to range from 3.5% to 21.9%.1–11 Early detection of a catheter related ventriculitis is important for the successful specific treatment, which includes the removal or the exchange of the catheter, and in selected cases also the intraventricular administration of antibiotics.12–14 The results from bacteriological cultures, however, are not available before at least 48 hours. Therefore they cannot contribute to the early detection of incipient catheter contamination and therapeutic measures. Routine clinical and laboratory parameters of infection may lack predictive value for the diagnosis of ventriculostomy related infection, as these may be changed by the underlying patient comorbidity.15
The aim of our study was to investigate the usefulness and reliability of various clinical and laboratory parameters for the early detection of incipient ventriculostomy related CSF infection, and furthermore to discover if the total drainage time related to the risk of a positive bacteriological CSF culture.
METHODS
All patients of the neurosurgical ICU who received external ventricular drainage during the three year observation period from 1993 to 1995 were included in the prospective study. Indications for external ventricular drainage included incipient hydrocephalus caused from intracranial haemorrhage (70 patients), CSF pathway occlusion because of posterior fossa or ventricular tumours (42 patients), treatment of post-traumatic brain oedema (12 patients), or treatment of a primary hydrocephalus, especially in children (six patients). Patients were either in critical conditions because of their underlying disease and were therefore referred to the ICU, or there was need for postoperative sedation and ventilation for brain protective reasons or for other reasons, such as pulmonary infection.
Catheter insertion procedure
All patients received antibiotic therapy either co-amoxiclav or ampicillin and sulbactam before ventricular catheter placement. After scalp shaving and preparation with chlorhexidine-ethanol solution, a silicone catheter was introduced through a precoronal burr hole into the ventricle. The catheter was tunnelled subcutaneously 4 cm to 6 cm from the insertion site. It was then connected to an 8 cm long pressure resistant tube, and further to a manifold consisting of two three-way stopcocks.
Catheter care and CSF sampling
The extracranial components of the drainage system and the ICP transducer were exchanged every 48 hours. The vacant tap was used to zero the ICP transducer, to take CSF samples and to flush the catheter in case of occlusion. Aseptic technique was applied, and meticulous desinfection of the connecting sites with chlorhexidine-ethanol solution was performed when manipulating the system, especially for daily CSF sampling. Only experienced ICU staff were involved with the sampling procedure, and they followed a strict protocol.
Labaratory parameters
CSF samples were obtained daily from the ventricular drain. They were examined for cell count, total protein concentration, and glucose concentration. Bacteriological CSF cultures were grown three times every week. The colour and appearance of the CSF samples were recorded. When considerable blood content made CSF cell counting unreliable or impossible, the respective data of these samples were excluded from the study. CSF pleocytosis was defined as a white cell count above 50/mm3.
Serum values of α1 antitrypsin, haptoglobin, fibronectin, C reactive protein as well as candida antigen and antibody were determined once every week. Peripheral white cell counts were taken daily. Peripheral leucocytosis was defined as a white cell count higher than 11 000 cells/mm3.
The daily maximum body temperature was recorded. Fever was defined as oral body temperature beyond 38°C. The occurrence or the course of infections at other bodysites was recorded. After the ventricular catheter was removed, the tip was cultured.
Statistical analysis of the respective data was performed using Fisher’s test and the Student’s t test.
RESULTS
Altogether 130 patients aged from 6 months to 79 years of age (mean 46 years) were included in the study (68 female and 62 male patients). Their diagnoses are summarised in table 1.
Diagnoses of 130 patients included in the study
A total of 186 external ventricular drains were inserted. The catheters remained in place between 1 and 25 days (mean 7.1 days). Total drainage time of the respective patients was between 1 and 50 days (mean: 10.3 days). Four hundred and seventy bacteriological CSF examinations were performed. In 41 samples from 21 patients the culture was reported positive between drainage day 1 and day 22 (mean 6.4 days). Bacteriological contamination of the cultured catheter tip was found in four cases (Staphylococcus epidermidis in three cases, Staphylococcus saccharolyticus in one case). The incidence of positive cultures in relation to the drainage day is illustrated in figure 1. The data from the bacteriological findings, the related CSF cell counts, and the treatment of the respective patients are summarised in table 2.
Bacteriological findings, CSF cell counts, and treatment in patients with positive CSF cultures
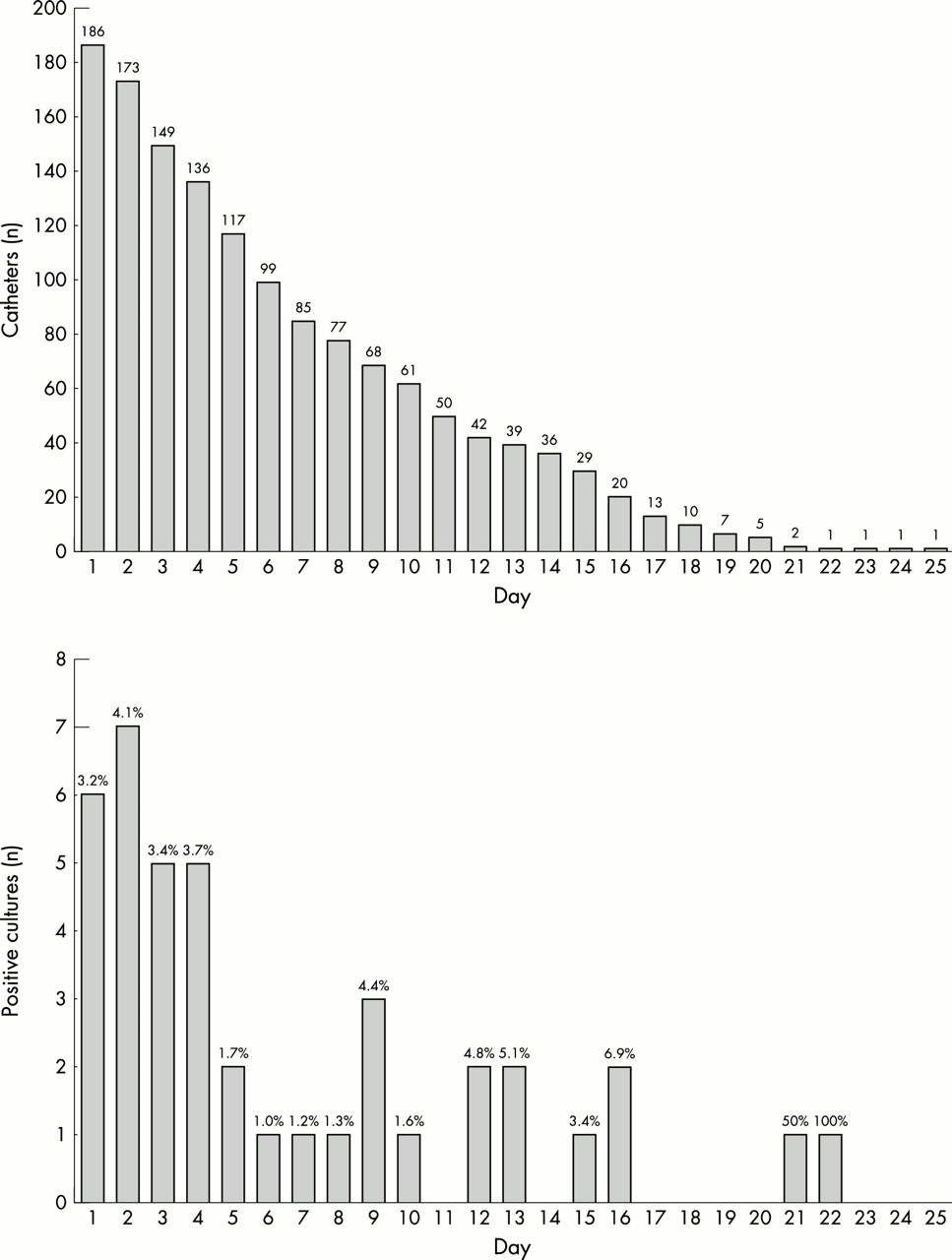
Total number of ventricular catheters and incidence of positve cultures in relation to drainage day.
Six patients with positive CSF cultures from day zero or day 1 after catheter insertion were treated with systemic antibiotic therapy only. In four patients with positive CSF culture the ventricular catheter was removed, and in 11 patients it was exchanged. Seven patients also received intraventricular antibiotic treatment using vancomycin.
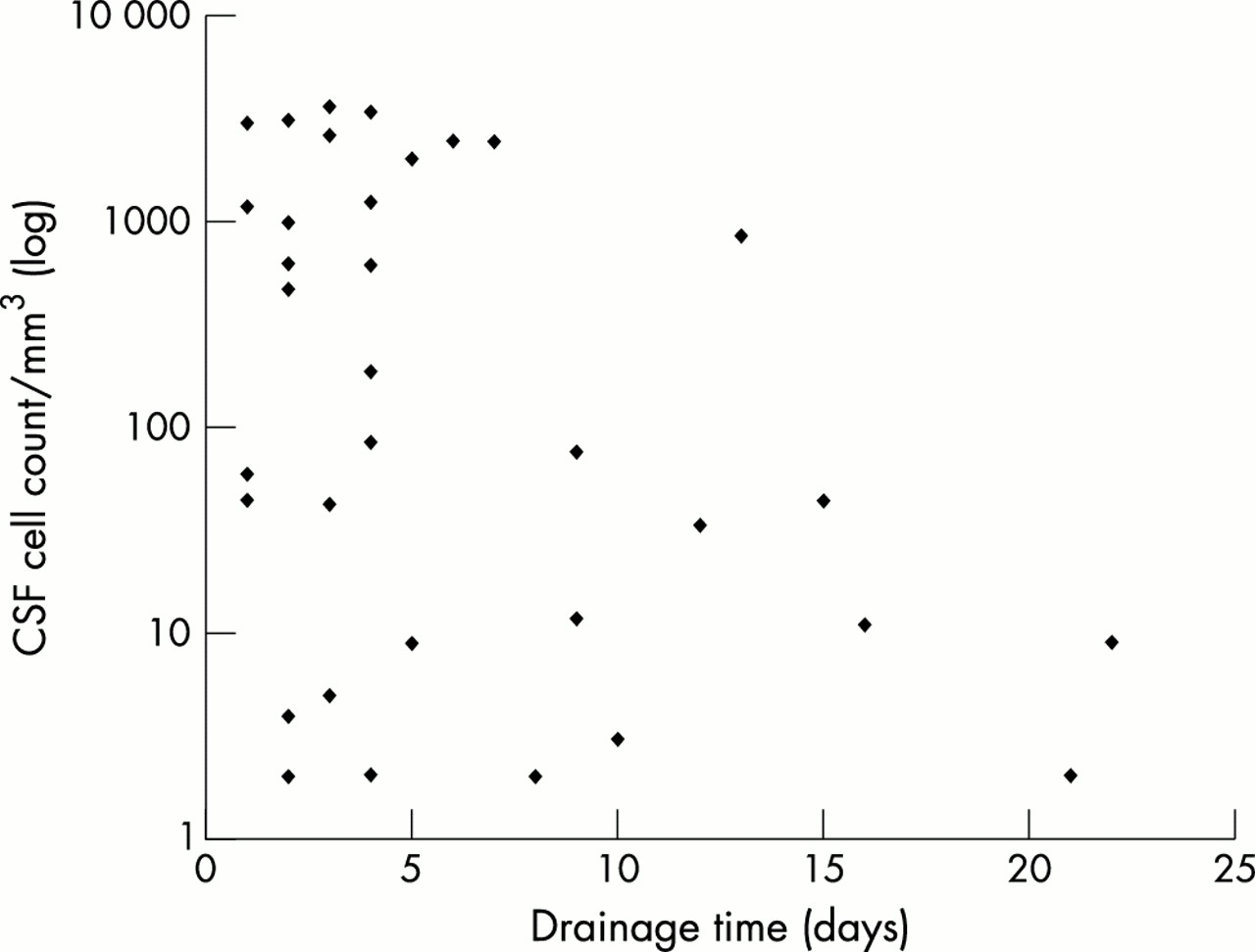
From 259 CSF samples no cell counts were obtained because of blood content. The cell counts from the remaining 1084 CSF samples, in relation to drainage time, are shown in figure 2. No significant correlation between drainage time and CSF cell count was found.

Distribution of CSF cell counts in relation to drainage day.
CSF cell counts that were taken together with bacteriological CSF examinations at the same day were available from 356 samples. In samples with positive bacteriological cultures, the CSF cell counts from the same day are shown in figure 3. They were significantly higher than with negative bacteriology (two tailed t test: p<0.05). CSF cell count significantly correlated with CSF infection.

{kind=link}
{kind=link}
{kind=link}
Distribution of CSF cell counts from bacteriologically positive samples.
No other significant correlation between the finding of a positive CSF culture and any of the following laboratory parameters was recorded (Fisher’s test): peripheral leucocytosis (p=0.86), fever (p=0.16), α1 antitrypsin (72 samples; p=0.16), haptoglobin (72 samples; p=0.66), fibronectin (72 samples; p=0.50), and C reactive protein (120 samples; p=0.61).
DISCUSSION
CSF infection and bacterial meningitis caused by contaminated ventricular catheters may become life threatening complications for ICU patients. Therefore, both the prevention of catheter infection and the early diagnosis of bacteriological CSF infection are of upmost importance in these patients.
The need for prophylactically administered antibiotics in external ventricular drainage is controversial.1,4,7,11,13,15–18 All patients in our study received antibiotics before insertion of their ventricular catheters. Yet, a positive CSF culture was found later in 21 patients (16.2%). This high incidence of CSF infections outlines the need for a prompt diagnosis to permit immediate specific treatment, such as the intraventricular administration of vancomycin, or the change of the ventricular catheter in severe infections.12–14,19,20
Clinical features are generally not helpful in detecting incipient bacteriological meningitis in ICU patients. Patients suffering from intracranial haemorrhage or severe head surgery frequently show signs of aseptic meningits, such as headache, nausea, and neck stiffness.14,15,18 In ventilated and sedated ICU patients the evaluation of clinical signs and the detection of a new focal neurological deficit or changes in their mental status is impossible. Therefore, in most cases with an external ventricular drainage the diagnosis of CFS infection is dependent upon laboratory findings.
A positive CSF culture or contamination establishes the definite diagnosis of a bacteriological infection. However, the result of such a culture is not available before at least 48 hours. Therefore, it is necessary to search for additional parameters that permit immediate recognition of an incipient infection from a CSF sample. It is reported in the literature, that routine laboratory infection parameters, such as peripheral leucocyte count, CSF glucose, or CSF protein levels, are not reliable predictors in CSF infections.15,21 Our study confirms these findings. However, our study also demonstrates, that additional parameters, such as serum, α1 antitrypsin, haptoglobin, fibronectin, and C reactive protein, do not correlate with the occurrence of positive bacteriological CSF cultures, and they are therefore not helpful to establish an early diagnosis of bacteriological meningitis in external ventricular drainage patients.
In our study, the only laboratory parameter that significantly correlated with positive CSF cultures was the CSF cell count. This is easy and cheap to obtain, it can be routinely determined every day, and the result is promptly available. However, besides CSF infection, there are numerous other reasons that can cause CSF pleocytosis, such as previous cranial surgery or subarachnoid haemorrhage.4,8 In our study we found a considerable number of patients showing CSF pleocytosis with negative CSF cultures. Therefore increases in the daily CSF cell count serial is highly suspicious of an incipient bacteriological CSF infection. We believe that this finding has adequate predictive value to change a previous therapeutic regimen, even if the bacteriological culture is not yet available. However, a rise in the CSF cell count cannot be determined during the first one or two days of external ventricular drainage and it lacks diagnostic potential during this period.
Drainage time is reported as a significant risk factor for catheter infection and even the routine change of ventricular catheters at every fifth day has been recommended.1,4 The findings of our study, however, do not determine drainage time as a significant risk factor for catheter infection. There was no significant correlation between drainage time and the occurrence of positive bacteriological CSF cultures. Therefore we do not recommend routine change of ventricular catheters after a certain drainage period. Moreover, we regard the bleeding risk with such a procedure, which is about 0.9% at our department, to be more hazardous than the risk for catheter infection from prolonged drainage time. In our opinion, daily CSF sampling does not lead to an increased risk for catheter infection, when aseptic techniques are applied and the procedure is performed by experienced ICU staff members following a standardised protocol.
REFERENCES
Footnotes
-
Competing interests: none declared