Article Text

Abstract
Background: Studies on the prevalence of multiple sclerosis have been carried out worldwide, showing a heterogeneous distribution between countries and even between the different regions of the same country.
Methods: We estimated the regional and national prevalence of multiple sclerosis in France on 1 January 2003, based on the computerised database of the national farmer health insurance system (“Mutualité Sociale Agricole”).
Results: There were 2667 cases of multiple sclerosis registered on the prevalence date, out of 4 098 477 affiliates. After standardisation on age, estimates for the national prevalence of multiple sclerosis in French farmers were 65.0 per 100 000 inhabitants (95% confidence interval 62.5 to 67.5), 41.9 per 100 000 in men (39.1 to 44.7) and 96.3 per 100 000 in women (92.0 to 100.6). The prevalence of multiple sclerosis was significantly higher in the north eastern regions (approximately 100 per 100 000 inhabitants) compared with the south western regions (around 50 per 100 000 inhabitants).
Conclusion: Our study is the first to evaluate the overall prevalence of multiple sclerosis in France and its 22 regions using the same methodology. Our results may be generalised to the whole French population as there is no convincing evidence of an increased or decreased susceptibility to multiple sclerosis among farmers or persons living in the countryside. This places France among the countries of medium to high prevalence. Confirming the uneven distribution of multiple sclerosis that correlates with latitude, raises once more the question of the role of genetic and environmental factors in the susceptibility to multiple sclerosis.
- ALD, Affections de Longue Durée
- MS, multiple sclerosis
Statistics from Altmetric.com
Studies on the prevalence of multiple sclerosis (MS) have been carried out worldwide, showing a heterogeneous distribution of cases between countries. This heterogeneity seems to correlate with latitude, with an increasing south to north gradient in the Northern hemisphere. Whether this gradient is caused by genetic or environmental factors remains a matter of debate.1–3 France is considered a country of medium to high prevalence for MS.4–8 To date, there has been no overall estimate of the prevalence of MS in France using the same methodology for all regions. The Mutualité Sociale Agricole is the second health insurance system in France. It has exclusive coverage of farmers and farm workers, as well as their spouses and children, provided they do not work outside the farm. Our objective was to estimate the overall prevalence of MS in France and in each of its 22 administrative regions.
METHODS
Source population
We studied the prevalence of MS on 1 January 2003, based on the computerised database of the Mutualité Sociale Agricole. In France, health insurance is a branch of the social security system. The active population is covered by statutory, occupation based, national health insurance schemes. All affiliates are automatically covered, as are the unemployed and the retired. The Mutualité Sociale Agricole is the second branch of social protection in France. It is a private professional organisation in charge of a public service mission, the management of the social risk of rural workers. It concerns farmers, salaried workers and their families. Its coverage among this population is complete and exclusive. When being affiliated, most of the general healthcare needs are partially reimbursed. The difference is generally covered by additional, private insurances. However, the treatment costs for those who suffer from chronic illnesses are completely reimbursed, provided the illness is on a list of the 30 admitted chronic diseases (Affections de Longue Durée, ALD). MS is listed as ALD No 25. Once the diagnosis has been established by a neurologist, a detailed request is addressed to the health insurance system by the neurologist or the family doctor. Since the approval of disease modifying treatments, some of them approved after the first clinical episode, this request is often made as soon as MS is diagnosed. We searched in our database for all registered cases of MS on 1 January 2003.
Statistical analysis
The crude prevalence proportions were estimated for France and each of the 22 administrative regions. Estimates and structure by age and sex of the French population were provided by the Institut National de la Statistique et des Etudes Economiques for the same date.9 The population of farmers covered by the Mutualité Sociale Agricole is older than the French population. The distribution is however similar in terms of sex. Therefore, we provided estimates of the prevalence proportions after standardisation according to the structure by age, but not by sex.
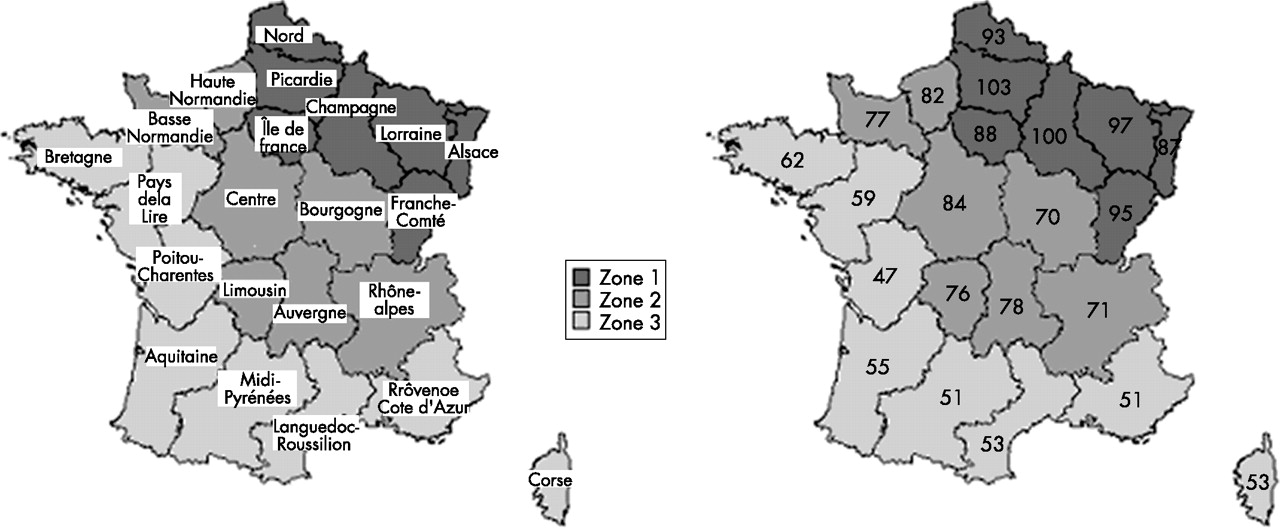
A χ2 trend test was performed to test the hypothesis of a north eastern to south western gradient, after dividing the 22 regions into three geographically defined zones, as shown in figure 1.
{kind=link}
Estimates of the regional prevalence of multiple sclerosis on 1 January 2003, per 100 000 inhabitants, standardised by age, among French farmers.
RESULTS
Overall prevalence of MS in France
On 1 January 2003, the Mutualité Sociale Agricole covered 4 098 477 persons, aged 49.9 (SD 25.8) years; 50% were women. There were 2667 cases of MS registered. Mean age was 54.9 (SD 14.5) years; 69% were women. The French population was 59 634 980 persons on the same date, aged 39 (23.2) years; 51% were women. After standardisation on age, estimates for the national prevalence of MS were 65.0 per 100 000 inhabitants (95% confidence interval 62.5 to 67.5), 41.9 per 100 000 in men (39.1 to 44.7) and 96.3 per 100 000 in women (92.0 to 100.6).
Prevalence of MS in the 22 administrative regions
Results are presented in table 1 and fig 1. The prevalence of MS was significantly higher in the north eastern (approximately 100 per 100 000 inhabitants) compared with the south western (approximately 50 per 100.000 inhabitants) regions, in the overall population as well as in women or men separately (p<0.001 for all comparisons).
Estimates of the prevalence of multiple sclerosis in French farmers after standardisation on age, on 1 January 2003
DISCUSSION
Our study addressed the question of the overall prevalence of MS in France. It is the first to evaluate the prevalence in each region using the same methodology. We estimated that the standardised prevalence of MS in France was 65 per 100 000 inhabitants among French farmers. We also demonstrated the existence of an uneven geographical distribution, with a gradient in prevalence that decreased by 50%, from 100 per 100 000 inhabitants in the north east to 50 in the south west. The same general trend was observed separately for men and women.
These estimations sound robust, as the whole French rural population is covered by the same health insurance system, without any limitation on access to healthcare. The mean age of the farmer’s population was 49.9 years (54.9 years for MS cases). The estimate is therefore unlikely to be biased because the disease has not yet appeared, as MS starts before the age of 40 years in more than 80% of patients.10,11 However, our figures may be underestimated. Report of MS as a long term illness to the health insurance system is usually conditioned by the need for treatment, either immunoactive or symptomatic. Early and benign cases may be missed by the system. This does not occur with more severe cases. This bias, however, is less in France because of the trend towards early prescription of disease modifying treatments.
Some patients may have changed their profession after the diagnosis of MS was established, for a less physically demanding occupation. In such cases, they would also have changed their insurance system. We have no precise data regarding this situation, which we consider to be rare. Ascertainment of cases may be discussed. Most of the MS cases are reported directly by neurologists, as neurologists are in charge of the diagnosis and are the only healthcare professionals allowed to prescribe approved immunoactive drugs in France. Some cases may be reported by general practitioners but usually after a diagnosis by a neurologist. Nevertheless, demonstration of the geographical gradient may be considered as very robust and reliable, as a differential declaration bias between the different regions would have been very unlikely.
Our results may be generalised to the whole of the French population, as there is no convincing evidence of increased or decreased susceptibility to MS among persons living in the countryside,3 apart from one positive association found in Norway between a rural inland residence and MS.12 The north east to south west gradient we observed for France is similar to that previously described in other countries.1–3 Furthermore, our estimates are in accordance with those already available in France.2,4–7 In 1994, the main French health insurance system (“Régime général de la Sécurité Sociale”) carried out a study of the prevalence of long lasting conditions, by random sampling of 2% of the patients declared as ALD.8 They estimated a prevalence rate of 40/100 000, which is lower than that reported in our study (65/100 000). However, there have been significant changes in reporting MS cases between 1994 and 2003, especially as a result of the introduction of immunoactive drugs for MS which are paid by the health insurance system. In 1994, the rule was to report only disabling cases, providing a systematic underestimation. The existence of a north to south gradient in the prevalence of MS in France had also been suggested previously from the systematic analysis of death certificates.4
Our results place France among countries of medium to high prevalence. Confirming the uneven distribution of MS raises the question of genetic and environmental factors in the risk of developing MS. It has been suggested that the north to south gradient observed in the USA could rather match immigration patterns of Europeans at higher or lower risk of developing MS.13 However, migration studies in South Africa, Israel, the UK and French West Indies suggest that the prevalence of MS can also depend on the environment, as it may even vary within populations sharing the same genetic background, depending on the age at immigration.14–18
Acknowledgments
The authors are indebted to Mr Laurent Laforest, Mrs Cécile Ritleng and Dr Eric Van Ganse for their help in the statistical analysis.
REFERENCES
Footnotes
-
Published Online First 13 February 2007
-
Competing interests: None.