Article Text

Abstract
Background: Positron emission tomography and single photon emission computed tomography scanning have 87–94% sensitivity and 80–100% specificity to differentiate patients with Parkinson’s disease (PD) from control subjects and patients with essential (ET) or atypical tremor. More than 10% of patients diagnosed as early PD can have scans without evidence of dopaminergic deficiency (SWEDDs). This study investigated whether smell tests can help identify possible cases with SWEDDs.
Methods: The 40 item University of Pennsylvania Smell Test (UPSIT) was used to evaluate the sense of smell in 21 SWEDDs patients. Twenty-six ET patients, 16 patients with a diagnosis of idiopathic adult onset dystonia (D), 191 non-demented PD patients and 136 control subjects were also tested. Multiple regression analyses were used to compare the mean UPSIT score in the SWEDDs group with the other four groups (ET, D, PD and controls) after adjusting for the effects of relevant covariates.
Results: The mean UPSIT score for the SWEDDs group was greater than in the PD group (p<0.001) and not different from the mean UPSIT in the control (p = 0.7), ET (p = 0.4) or D (p = 0.9) groups. Smell tests indicated a high probability of PD in only 23.8% of SWEDDs as opposed to 85.3% of PD patients.
Conclusions: In a patient with suspected PD, a high PD probability on smell testing favours the diagnosis of PD, and a low PD probability strengthens the indication for dopamine transporter imaging.
Statistics from Altmetric.com
Parkinson’s disease (PD) affects as many as 2% of all adults over the age of 65 years1 and most commonly presents with rest tremor although the presence of bradykinesia on neurological examination is a sine qua non for its clinical confirmation.2 The severity of bradykinesia loosely correlates with the extent of the nigrostriatal dopaminergic lesion assessed in vivo using dopamine transporter single photon emission computed tomography (SPECT) (DaTSCAN) or F-DOPA positron emission tomography (PET) imaging.3 DaTSCAN has been licensed in Europe to differentiate PD patients from patients with essential tremor (ET),4 a condition which is commonly confused with PD in general practice.5 The diagnostic accuracy of movement disorder specialists in patients with late stage PD can exceed 90%.6 However, 4–14.7% of early patients enrolled in “de novo” drug trials with a clinical diagnosis of PD have scans without evidence of dopaminergic deficiency (SWEDDs),7–9 and almost all of these are now thought to be due to clinical misdiagnosis.
Hyposmia occurs in 80–100% of PD cases,10–12 and because smell identification in ET is normal or only mildly decreased, smell tests have also been suggested as a way to help distinguish PD from ET.13 14 We hypothesised that olfaction would be normal in SWEDDs patients, and that smell tests might be useful in the routine assessment of atypical tremor syndromes where PD is suspected. A more accurate distinction between these commonly confused disorders would also help to reduce the number of non-parkinsonian patients enrolled in clinical trials. We have administered smell identification tests to 21 patients with SWEDDs and compared the scores with those of groups of patients with clinically diagnosed PD and normal controls. We have also tested some patients with ET and adult onset dystonia, syndromes which have been considered as possible alternative diagnoses for SWEDDs patients.15 16
METHODS
Smell testing
The North American version of the 40 item University of Pennsylvania Smell Identification Test (UPSIT)17 was used to test odour identification.
Subjects
UPSIT testing was performed in 21 patients who had been diagnosed with PD by a neurologist and who subsequently had normal dopamine transporter SPECT scanning using [123I]-FP-CIT SPECT (DaTSCAN) (SWEDDS group). Smell tests were also carried out on 26 patients diagnosed with ET by a movement disorder specialist (group ET), and who fulfilled TRIG criteria18 for definite (n = 5), probable (n = 17, seven of whom had normal DaTSCAN) or possible ET (n = 4, three of whom had normal DaTSCAN); 16 patients with a clinical diagnosis of idiopathic adult onset dystonia (group D), 12 of whom had cervical dystonia, two had dystonia with tremor in the arms, one had writer’s cramp and one had essential blepharospasm; 191 non-demented patients who fulfilled the clinical diagnostic criteria for PD2 (group PD); and 136 control subjects. All subjects were screened for dementia using the first item of part I of the Unified Parkinson’s Disease Rating Scale19 and those who scored ⩾1 underwent additional Mini-Mental State Examination (MMSE).20 No patient presented cognitive complaint or scored less than 27 in the MMSE, except for one patient from the SWEDDs group who scored 24/30.
All patients in groups PD, D and control, and 18 SWEDDs and 16 ET subjects were recruited from patients, visitors and staff at the National Hospital for Neurology and Neurosurgery, London, UK. Three subjects with SWEDDs and 10 with ET were recruited from the movement disorder clinic at the Institute of Neurological Sciences, Glasgow, UK. Informed consent was obtained from all subjects according to ethical protocols approved by the regional and local ethics committees.
All patients with SWEDDs had a tremor at rest and difficulty with fine finger movements, and most also had some accompanying limb rigidity. After the normal DaTSCAN result, patients were re-examined and all but two failed to show a clear decrement in speed and amplitude on sequential fine finger movement testing, although most had slowness. A detailed clinical description of 18 of the 21 subjects with SWEDDs that were smell tested as part of this study is reported elsewhere.21
Statistical analysis
To compare the mean UPSIT score in the SWEDDs group with the other four groups (ET, D, PD and controls), we used a multiple linear regression analysis for the UPSIT as the dependent variable and region of living, gender, age and four group indicator variables as covariates. To compare the mean UPSIT score in the control group with the other four groups (SWEDDs, ET, D and PD), we used a multiple linear regression analysis for the UPSIT as the dependent variable and region of living, gender, age, smoking and four group indicator variables as covariates. The assumptions underlying the regression analysis were checked by a study of the residuals and were found to be satisfactory. A significance level of 0.05 was used for all hypothesis testing. We classified the result of the smell test in each patient of the SWEDDs group in terms of high or low probability of PD22 to see if low PD probability in the smell test could identify potential SWEDDs.
RESULTS
Table 1 shows a summary of clinical data of participants from all groups and fig 1 illustrates the distribution of UPSIT results in the five patient groups.

University of Pennsylvania Smell Identification Test (UPSIT) scores in the five patient groups. The median (horizontal line) is within the box containing the central 50% of the observations (ie, the upper and lower limits of the box are the 75th and 25th percentiles): the extremes of the “whiskers” contain the central 95% of the ordered observations. Outliers are showed as circles. ET, essential tremor; PD, Parkinson’s disease; SWEDDs, patients with scans without evidence of dopaminergic deficit.
The mean UPSIT score for the SWEDDs group was greater than in the PD group (p<0.001, 95% CI for β = −13.7 to −8.1) and did not differ from the mean UPSIT in the control (p = 0.7, 95% CI for β = −2.4 to +3.3), ET (p = 0.4, 95% CI for β = −2.2 to +5.1) or D (p = 0.9, 95% CI for β = −4.2 to +3.6) groups. Mean UPSIT score in the controls was greater than in the PD group (p<0.001, 95% CI for β = −12.7 to −10.1) and not different from the mean UPSIT in the ET (p = 0.5, 95% CI for β = −2.1 to +4.0), D (p = 0.6, 95% CI for β = −3.8 to +2.3) or SWEDDs (p = 0.7, 95% CI for β = −3.3 to +2.4) groups. In both regression analyses, age (p<0.001, 95% CI for β = −0.3 to −0.1), gender (p = 0.009, 95% CI for β = −2.7 to −0.4) and region of living (p = 0.02, 95% CI for β = −8.4 to −0.7) were significant covariates but smoking was not (p = 0.06, 95% CI for β = −3.7 to +0.1).
Table 2 shows the clinical data for the 21 SWEDDs patients, including the result of the smell test in terms of score and corresponding PD probability22 and core signs of parkinsonism.
DISCUSSION
The clinical significance of normal presynaptic dopaminergic imaging in a patient with a clinical diagnosis of degenerative Parkinsonism is still controversial but follow-up studies suggest that only a minority of patients with SWEDDs actually have nigrostriatal denervation or are due to supranigral causes of parkinsonism (eg, cerebrovascular disease or cryptic neuroleptic use). A 4 year follow-up study in 150 subjects with suspected presynaptic dopaminergic deficiency who had normal DaTSCANs showed that in only four was the diagnosis of degenerative parkinsonism upheld clinically.15 In a “de novo” therapeutic trial which enrolled 186 patients with a diagnosis of early PD, 21 subjects were found to have normal baseline 18F-dopa PET scans; the scans were repeated after 2 years in 19 of these patients and all were still normal.9 In another similar trial,7 21 of 142 subjects with early “de novo” PD had a normal dopamine transporter scan at baseline and “had no worsening of the 123Iβ-CIT uptake at week 40” of follow-up. Furthermore, most of these cases did not respond to L-dopa, and another study showed successful withdrawal of antiparkinsonian therapy in 11 patients who fulfilled Queen Square Brain Bank criteria for PD but had normal DaTSCAN.23 Essential tremor has been considered as a probable diagnosis for a number of these cases.9 Dopamine transporter imaging with SPECT using [123I]-FP-CIT SPECT (trade name DaTSCAN) is licensed in Europe to differentiate ET from PD4 based on data showing a sensitivity of 87–94% and specificity of 80–100%.24–27 Our data provide further support for the notion that most cases of SWEDDs do not have Parkinson’s disease as their smell test scores were in the same range as control subjects and significantly different from patients with PD. One of our patients with 2 years’ disease duration who fulfilled diagnostic criteria for PD was found to have a normal DaTSCAN and entered the study in the SWEDDs group. The patient scored 14/40 in the UPSIT, indicating high PD probability. During follow-up, his parkinsonism worsened and a repeat DaTSCAN was abnormal, leading to revised inclusion in the PD group.
Focal or segmental dystonia is a frequent accompaniment in atypical tremor syndromes which masquerade as PD.16 Smell test scores in the 16 patients with idiopathic adult onset segmental or focal dystonia were in the control range, and did not differ from the scores recorded in the patients with SWEDDs. Further larger studies are needed, however, before one can conclude that olfaction is unaffected in dystonia. Most of the patients with ET included in this study did not fulfil the stringent TRIG criteria18 for definite ET as they presented either with atypical features or short disease duration. However, they had all been seen by movement disorder specialists and carried the label of ET. Their inclusion in this study under the ET label seems reasonable, and is in broad agreement with standard clinical practice, although in our view some of them might better be labelled as dystonic tremor or atypical tremor. These cases are also the ones most likely to be confused with PD. The ambiguity in current definitions of essential tremor may partly explain the finding of normal smell sense in some series13 14 28 29 and mild hyposmia in others.30–32 Even if one accepts that mild smell deficits may be seen in some ET cases, there is still a large gap between the average UPSIT in ET and PD patients.
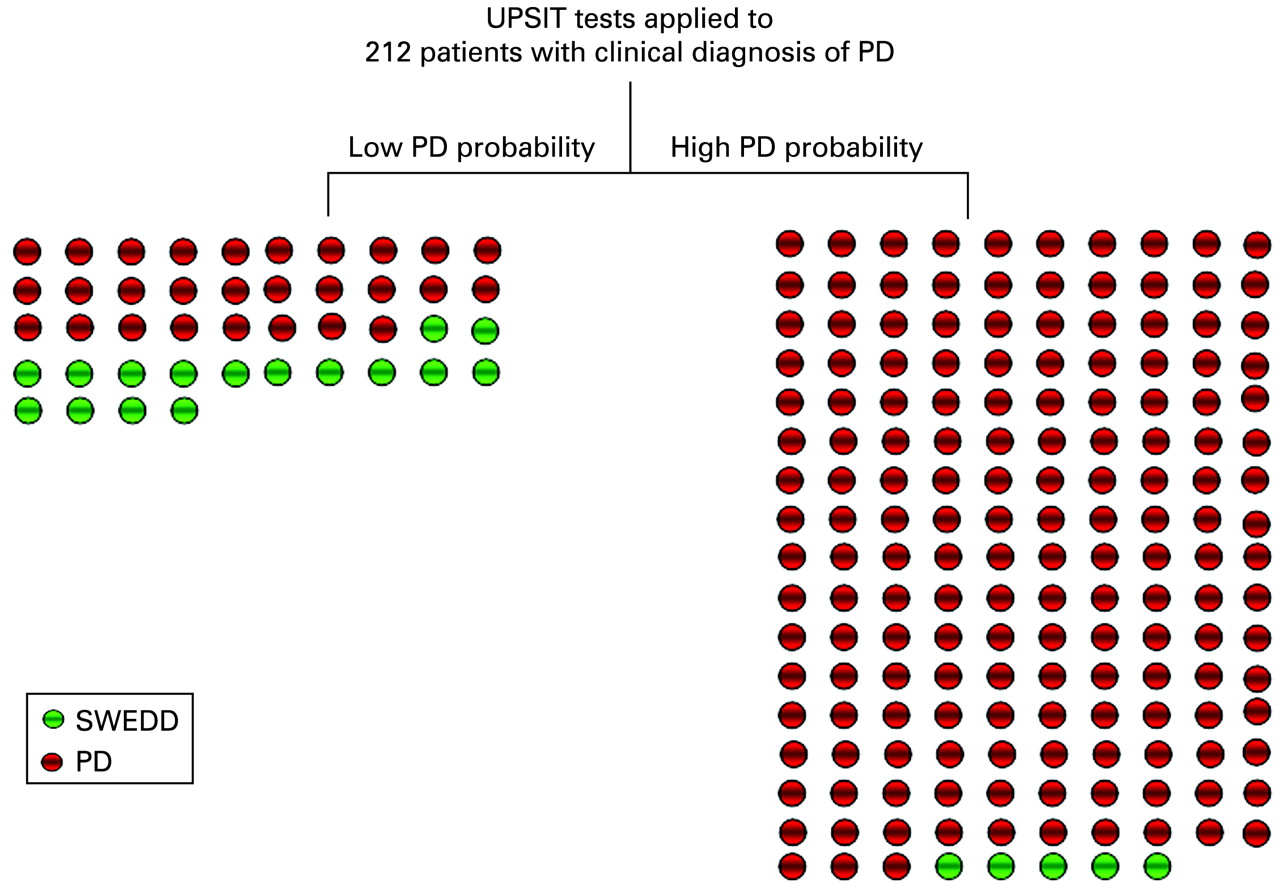
Although only 29 of the patients with PD in the study had undergone a DaTSCAN, we believe the number of SWEDDs cases in the entire group is likely to be small as all the patients fulfilled the Queen Square Brain Bank Criteria and importantly had been under continuous observation in a specialist movement disorder clinic for several years. We have used our data to extrapolate the accuracy of smell tests in the clinical setting of a population with suspected PD based on the assumption that most if not all of them will turn out to have pathologically confirmed PD. It remains conceivable that some of our PD patients might have had SWEDDs but the progressive nature of their illness and the positive response to L-dopa with the emergence of dyskinesias makes it unlikely that the diagnostic error rate would be substantial. As schematised in fig 2, taking 212 patients with a presumptive diagnosis of PD (all of our patients from the PD group plus our patients from the SWEDDs group), the UPSIT gives a high probability of PD in 168 (163/191 (85%) PD and 5/21 (23%) SWEDDs patients). The smell test result would be accurate in 97% (ie, of the 168 patients with a high PD probability on UPSIT, 163 would be real PD; 95% CI 94.4% to 99.6%). On the other hand, although the majority of SWEDDs patients (16/21, 73%) had a low PD probability on the UPSIT, 14% (28 out of 191) of the PD patients also did, indicating that for the 44 subjects with low probability, the smell test would be accurate in 36% (16/44, 95% CI 23.7% to 51.2%). Given that the overall number of SWEDDs is 21 out of 212 (9.9%, similar to the literature), normal smell testing increases threefold the likelihood that a patient with a clinical diagnosis of PD would have a normal DaTSCAN and therefore a diagnosis other than PD.
{kind=link}
{kind=link}
Distribution of patients with Parkinson’s disease (PD) and scans without evidence of dopaminergic deficiency (SWEDDs) according to the University of Pennsylvania Smell Identification Test (UPSIT). UPSIT tests applied to 212 patients with a clinical diagnosis of PD. Each circle represents a patient.
Five of the 21 SWEDDs patients had a high probability of PD on smell testing, indicating that false positive results can occur. Chronic rhinitis33 and a cold or sinusitis are confounding factors which can lead to temporary or even permanent smell sense loss34 and it is possible that the low UPSIT observed in these patients could be due to non-neurological causes. As hyposmia may also be found in persons with mild cognitive impairment and Alzheimer’s disease,35 the low MMSE (24/30) in SWEDDs patient number No 19 could also be of relevance. If smell tests are to be incorporated into a research protocol, a counsel of perfection would be to arrange an evaluation by an otorhinolaryngologist to exclude other causes of hyposmia, and to apply a stringent cut-off in the MMSE score.
A high UPSIT score suggesting a low probability of PD does not per se make an individual highly unlikely to have PD because there is a significant number of false positives but it does increase threefold the probability of an alternative diagnosis. In routine clinical practice this finding is relevant and should lead to a careful review of the other clinical findings (eg, Is there a poor response to levodopa? Has there been negligible disease progression? Is there unequivocal bradykinesia?). If doubt increases after review, then the findings on smell testing strengthen the clinical indication for a DaTSCAN. Baseline smell testing also offers a less expensive and more convenient alternative to baseline DAT scanning in a clinical research setting where one wants to minimise the possibility of including patients without Parkinson’s disease, especially in trials for de novo patients or early stage PD. The cost of a DaTSCAN is approximately €762 (£672) per patient without the cost of medical personnel36 while an UPSIT costs US$26.95 (£19),37 making it at least 30 times cheaper. In addition, there are other smell test batteries which are even less expensive, such as the 16 item smell identification test from Sniffin’ Sticks, which has been shown to have similar accuracy to the UPSIT in differentiating PD patients from controls.22
REFERENCES
Footnotes
Competing interests: None.
Funding: This work was funded by the Reta Lila Weston Trust for Medical Research and LS-M is a beneficiary of a Reta Lila Weston fellowship. PS was funded by the Austrian Science Fund (FWF, Erwin Schrödinger Grant).
Ethics approval: Ethics Committee approval was obtained from the regional and local ethics committee in the National Hospital for Neurology and Neurosurgery, London, UK and regional and local ethics committee in the Southern General Hospital, Glasgow, UK.