Article Text

Abstract
Background: Duchenne muscular dystrophy (DMD) leads to progressive impairment of muscle function, respiratory failure and premature death. Longitudinal data on the course of physical disability and respiratory function are sparse.
Objectives: To assess prospectively physical impairment and disability, respiratory function and survival in patients with DMD over several years to describe the course of the disease with current care.
Methods: In 43 patients with DMD, aged 5–35 years, yearly assessments of physical disability by the Duchenne muscular dystrophy physical Impairment and Dependence on care (DID) score, ranging from 9 (no disability) to 80 (complete dependence), and forced vital capacity (FVC), were obtained over a mean time interval of 5.4 (SD 2.1) years.
Results: DID scores were correlated with age according to a hyperbolic function (f = 85.3×age/(10.05+age), R = 0.62, p<0.0001). FVC declined exponentially with age (f = 139.1×exp(−0.08×age), R = 0.52, p<0.0001). Mean age at which patients lost their ambulation was 9.4 (SD 2.4) years and they became dependent on an electric wheelchair at 14.6 (4.0) years. Age at the beginning of assisted ventilation was 19.8 (3.9) years, Three patients died during the observation period. The estimated probability of survival to age 30 years was 85% (median survival was 35 years).
Conclusions: Our detailed observations of the progression of physical disability, dependence on care and respiratory impairment in patients with DMD from childhood to adult life is valuable for predicting the clinical course with current medical care. Compared with historical data, survival has improved considerably.
Statistics from Altmetric.com
Duchenne muscular dystrophy (DMD) is the most common form of the inherited muscular dystrophies affecting approximately 1 in 3300 male births. The disorder is caused by mutations in the gene located at Xp21 which codes for the dystrophin protein. DMD leads to progressive muscular weakness, severe physical disability and ultimately death.1 2 Most patients with DMD become wheelchair users in childhood, and they depend largely on their parents for their daily activities and care.3 In more advanced stages of the disease, the progressive spinal and chest wall deformity and impairment of respiratory muscle function leads to hypercapnic respiratory failure, and cardiac muscle involvement may entail congestive heart failure.4 Recent studies suggest that non-invasive positive pressure ventilation and other supportive measures prolong survival of patients with DMD well into adulthood.5 6
With prolongation of life, physical impairment and dependence on care increases because of the progressive nature of the disorder but data on this topic from adult patients with DMD are limited or outdated.1 3 7 8 We are aware of only one cohort for whom longitudinal data on physical disability in adult patients with DMD were reported.7 9 Prediction of profiles was limited by the small number of patients included and a relatively short follow-up time.7 Knowledge of the course of physical impairment in DMD is of great importance to patients, parents and health care providers because it allows for a realistic outlook on the progression of the disease, facilitates planning of long term care, and defines the specific problems and needs of patients with DMD.
Previously, conventional evaluation of physical impairment has mainly focused on motor deficits based on measurement of muscle strength3 10 but such measures might not appropriately capture the clinically relevant functional disabilities of the patients. To overcome this limitation, several scores have been proposed to assess physical impairment in patients with neuromuscular diseases but they were not specifically designed for patients with DMD of various age ranges.11–15 Therefore, we recently introduced a simple DMD specific score that assesses the various aspects of physical impairment and dependency on help by others and technical aids5 that we termed the DID score (Duchenne muscular dystrophy physical Impairment and Dependency score).
In this study, we applied the DID score to prospectively investigate the long term course of physical impairment and dependence on care, along with lung function and survival in a cohort of 43 patients with DMD. The aim was to provide current profiles of the clinical presentation and natural history of DMD from childhood into adult life in order to predict the individual clinical course of the disease with current medical care.
METHODS
Patients
Patients with DMD living or attending school in a facility specialised in the care of patients with muscular dystrophy, the Mathilde-Escher-Heim, Zurich, Switzerland, were prospectively enrolled during the period from 1999 to 2006. The diagnosis of DMD was based on standard criteria: progressive symmetrical muscle weakness and other signs and symptoms starting before the age of 5 years; elevated serum creatinine kinase activity; muscle biopsy and/or genetic analysis; and, in some, a family history consistent with X chromosome linked recessive inheritance.16 Information on genetic analysis was available from 10 patients (nine patients had a deletion in at least one of the exons 48–52 of the DMD gene locus whereas a duplication mutation was found in one patient). The study protocol was approved by the local ethics committee and patients gave informed consent to participate.
Measurements
A physical examination, including measurement of body weight and height, was performed and body mass index (BMI) was calculated. Height was used for calculation of reference values of pulmonary function. It was determined by a flexible ruler fitted along the contours of the body, from the head, along the vertebral spine and the back of the legs, to the heels to account for kyphoscoliosis and leg contractures.
Spirometry was performed in the sitting position with a flowmeter attached to a flanged rubber mouthpiece with the nose occluded.17 Reference values for ages up to 17 years18 and above19 were computed.
Physical impairment and the inability to perform activities of daily living and dependence on others and on technical aids was evaluated with the DID score specifically developed at our centre for patients with DMD, as described previously (see appendix online).5 The DID score consists of the following eight aspects of daily life: mobility without technical aids, mobility with technical aids, transfers (eg, from bed to wheelchair), changes in body position, dressing, static body control, feeding and breathing. Each aspect is rated with up to 10 points, with higher scores reflecting greater impairment and disability. The sum score of all eight domains is calculated as a measure of overall impairment, disability and dependency, with a minimal value of 9 (no impairment in any of the domains) and a maximum value of 80 points (completely impaired and dependent on help by others in all domains). The DID score was prospectively applied on a yearly basis.
For evaluation of interobserver agreement, two experienced physical therapists independently applied the DID score to all patients with DMD alive in 2006.
Data analysis
Data are expressed as means (SD). Regression analysis was used to determine the relationships among the DID score, forced vital capacity (FVC) and age. Survival probability was calculated by the Kaplan–Meier method. Interobserver agreement between DID scores obtained by two observers was evaluated by Pearson’s correlation and by calculating the mean difference (bias) and limits of agreement (±2 SD).20 A probability value of <0.05 was considered statistically significant.
RESULTS
Demographics
Forty-three patients with DMD with a mean age of 15.3 (SD 5.2) years and a BMI of 20.0 (7.3) kg/m2 at enrolment were followed over a time period of 5.4 (2.1) years (range 1–8). The course of weight, height and BMI is shown for selected ages in table 1.
Physical impairment and dependency
In total, 227 yearly assessments were performed in 43 patients. Milestones of the clinical course in patients with DMD are described in table 1. Individual trends in DID scores over time are shown in fig 1. Progression of physical impairment and disability, as reflected by the DID score at any particular age, was strongly correlated with age (in years) according to the hyperbolic function: DID score = 85.33×age/(10.05+age), R = 0.62, p<0.0001. The DID scores of 19 out of 20 patients (95%) whose initial score was above the fitted hyperbolic line remained above this line. Thus an advanced disability at the first observation was associated with a subsequent further continuous progression in disability. The DID score of only nine patients crossed the fitted line on a total of 11 occasions, eight in an upward direction (worse) but only three in a downward direction (improved) (χ2 test, p = 0.03).

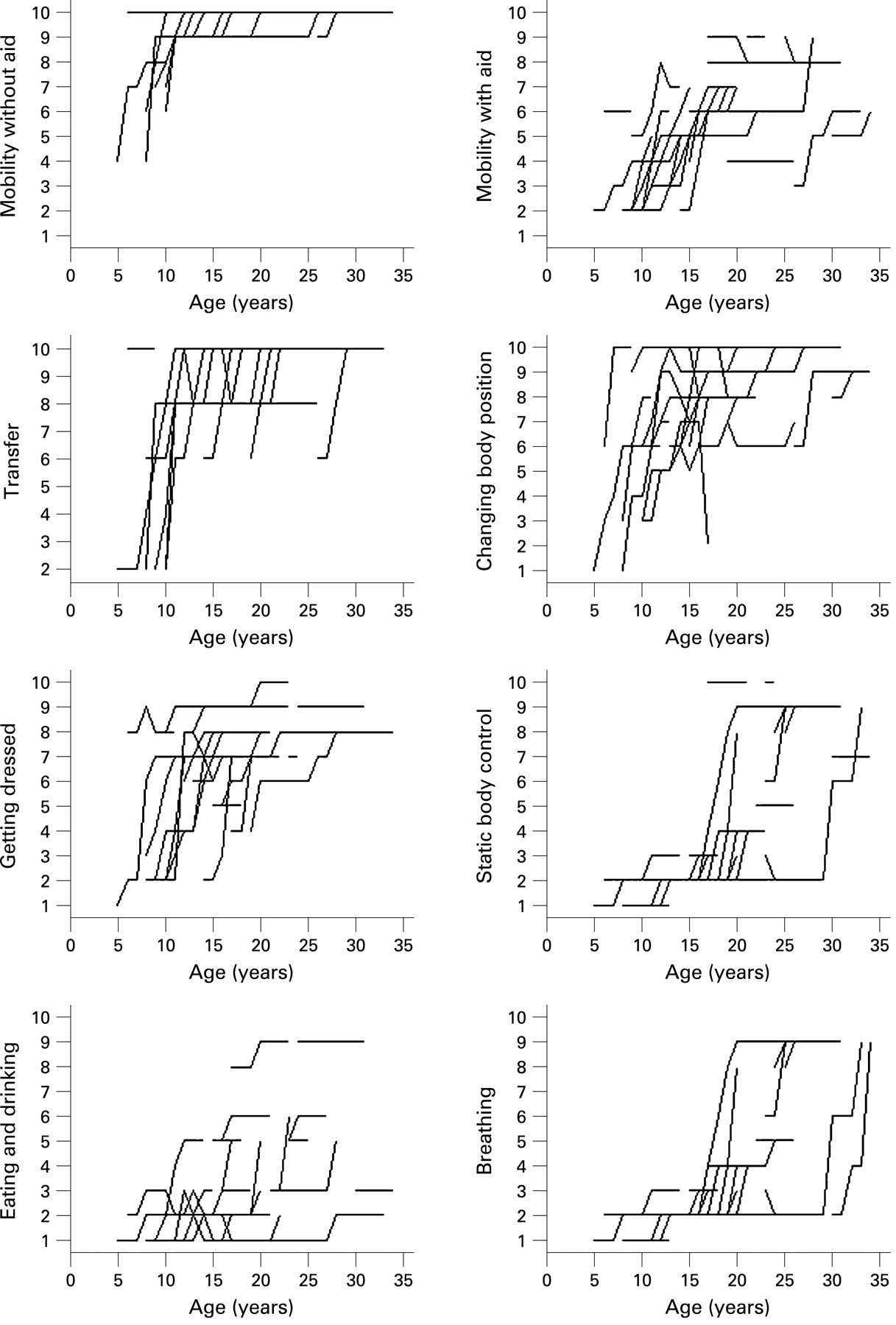
Follow-up assessments of the eight domains of the DID score revealed that the impairment in the domains “mobility without technical aid”, “mobility with technical aid”, “transfer”, “changes in body position” and “getting dressed” started at around the age of 5 years and increased rapidly until the age of 10–15 years with a subsequent plateau at the maximum level of disability. In contrast, progression of impairment in the domains “static body control”, “eating and drinking” and “breathing” was moderate in early life but accelerated in adulthood (fig 2).

For some domains of the DID score specific milestones in the clinical course of the disease are listed in table 1. Mean age at which patients lost their ambulation was 9.4 (2.4) years (range 6–15). They became dependent on an electric wheelchair at 14.6 (4.0) years (range 11–28). Thirty-three patients (77%) had undergone spinal fusion surgery at a mean age of 14.2 (2.6) years (range 8–21). Age when food and drinks had to be given to a patient by a caregiver was 18.2 (4.2) years (range 12–23), and the age at which 22 of the patients required assisted mechanical ventilation was 19.8 (3.9) years (range 14–31). In eight patients (19%) a gastrostomy had been performed at a mean age of 24.7 (4.9) years (range 20–34) because of feeding problems.
DID scores obtained independently by two observers in 40 patients were closely correlated (r = 0.96, p<0.0001) with a mean difference of 2.1 points and limits of agreement (±2 SD of bias) of 4.6 points.
Lung function
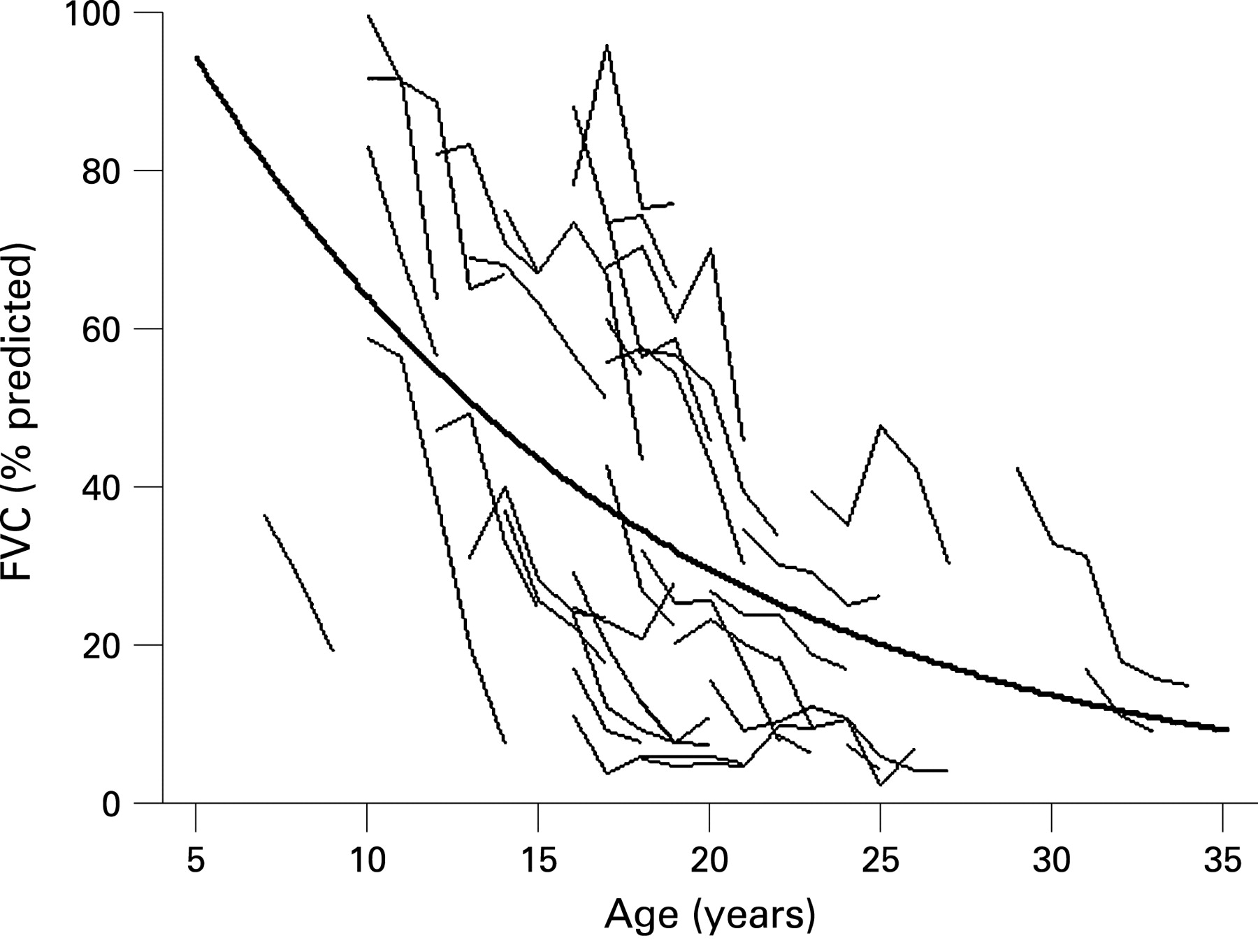
FVC revealed an exponential decline with age according to the function: FVC = 139.1×exp(−0.08*age), R = 0.52, p<0.0001 (fig 3). Mean age at which FVC fell below 1 litre was 18.1 (5.0) years (range 13–31).

Twenty-two of the 43 patients (51%) received long term assisted mechanical ventilation for chronic respiratory failure. Seventeen of these patients were ventilated non-invasively with a nasal or oral–nasal mask, and five patients via tracheotomy. Mean age at the beginning of mechanical ventilation was 19.8 (3.9) years (range 14–31) and mean FVC was 0.73 (0.34) litre (20 (10)% of predicted).
Survival
Only three of the 43 patients with DMD died during the follow-up period. One patient died because of heart failure due to cardiomyopathy at the age of 35 years, one patient died suddenly 8 days after tracheotomy at the age of 22 years and one patient died of respiratory failure at the age of 24 years. Kaplan–Meier analysis revealed a median survival of 35 years. The probability of surviving 10 years after initiation of assisted mechanical ventilation was 68% (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
We prospectively investigated the clinical course in patients with DMD from childhood to adult life and identified milestones of disease progression. The strength of our study is the detailed observation of the course of physical impairment and dependence on care over several years by using the DID score along with spirometry and survival in a large patient cohort. The current update on the clinical course of DMD is valuable for patients, families and health professionals as an adjunct in planning medical care and future life. The median survival of 35 years compares favourably with historical data and presumably reflects advances in assisted mechanical ventilation and other supportive care.
We recorded the clinical course of patients with DMD using a recently introduced instrument, the DID score, that assesses eight different aspects of impairment and disability in daily life.5 The DID score quantifies the physical impairment in patients with DMD with high interobserver agreement and identified clinical milestones such as loss of ambulation at a mean age of 9.4 years, dependence on an electric wheelchair at 14.6 years, dependence on being dressed and fed by caregivers at 18.2 years and requirement for assisted mechanical ventilation at 19.8 years. In contrast with other (generic) scores such as the index of activities of daily living which was designed for the elderly,11 the DID score incorporates aspects of disability typical for patients with DMD and relevant to their entire life span. Similar to the EK score, which focuses on disability in non-ambulatory patients with DMD,15 the DID score assesses wheelchair mobility, transfer, static body control and dependence on help with eating and drinking. But unlike the EK score, the DID score also incorporates observations on mobility without technical aids (see appendix, domain 1 online), and specifically addresses the need for assisted mechanical ventilation (see appendix, domain 8 online) which has become an essential life saving component of care.
The DID scores progressed rapidly in childhood and subsequently approached maximal values corresponding to nearly total dependence on caregivers and technical aids such as a wheelchair and mechanical ventilation. Individual grades of disability at a certain age varied, possibly related to differences in treatment and lifestyle,21–23 although all patients with DMD in our study received medical care by the same institution. We observed an increase in DID scores over time according to a hyperbolic function (fig 2). Almost all patients (95%) who initially scored above the regression line did so in every subsequent follow-up (fig 1). Scores for the eight domains incorporated into the DID score followed two different patterns (fig 2): the progression in the domains ”mobility without technical aid”, “mobility with technical aid”, “transfer”, “changes of position” and “getting dressed” followed a hyperbolic function characterised by a steep initial increase to an asymptotically approached maximum value, while the scores for the domains ”static body control”, “eating and drinking” and “breathing” progressed exponentially indicating that these functions were severely affected late in the course. This may be related to the different types of muscles involved in these functions, as proximal skeletal muscles, which contain large muscle fibres, are affected early in the course of DMD, whereas muscles containing small calibre fibres are relatively spared initially, so that breathing and eating are more gradually impaired, a finding supported by animal models.24 25
FVC progressed with advancing age in accordance with our previous report and that of others.5 6 Lung function rapidly deteriorated in young patients but declined less steeply thereafter (fig 3). Correspondingly, a more rapid yearly FVC decline of 8.5% was reported in patients with DMD at 10–20 years of age, whereas the decline was reduced to 6.2% per year above the age of 20 years.26 It has been previously reported that patients with DMD are more likely to develop chronic respiratory failure if their vital capacity falls below 1 litre and the 5 year survival rate was only 8% if assisted ventilation was not provided.27 In an early study, Brooke and colleagues3 found that patients with DMD passed this milestone at a median age of 13.5 years whereas in the current study FVC was reduced to 1 litre at a considerably older age of 18.1 years. A possible explanation is the more general application of glucocorticosteroid therapy and other changes in treatment within the past two decades.23 Unfortunately, there was no reliable information on previous glucocorticosteroid therapy available from our study cohort and thus we have not been able to explore the potential impact of this treatment on lung function. The less rapid reduction of FVC compared with earlier studies is unlikely related to the use of cough assist devices as our patients used such devices only during periods of increased mucus production (eg, during chest infections). Half of our patients had less than 20% of predicted FVC by the age of 20 years which corresponds approximately to the age at which assisted mechanical ventilation was initiated (on average 19.8 years). Similar to our findings, Toussaint and colleagues6 reported a mean age of 19.4 years and FVC of 21% predicted at the time of initiation of positive pressure ventilation.
Median survival of 35 years which we observed (fig 4) is considerably higher than the median survival of 14.4–20.5 years reported in patients not treated with assisted ventilation,27–29 and 26–33 years in patients receiving long term mechanical ventilation.6 30 31 The probability of surviving 5 years after initiation of assisted ventilation was 70% in two studies analysing this outcome.6 32 In our cohort, survival 5 and 10 years after beginning assisted mechanical ventilation was 82% and 68%, respectively (fig 4). The recent improvement in survival of patients with DMD may not only reflect advances in treatment but also the changing attitudes of caregivers regarding various therapeutic options (eg, therapy of cardiomyopathy, and spinal fusion surgery).30
In conclusion, our prospective longitudinal study provides novel data on the clinical course of DMD from childhood to adult life which updates and extends earlier cross sectional observations. The DID score is a valuable instrument to describe the distinct patterns of disease progression in several domains of physical impairment and dependence on care. Our observations on clinical milestones and on the improved survival represent essential information for patients with DMD, their families and caregivers as a basis for planning and evaluating care and therapeutic interventions.
REFERENCES
Footnotes
Competing interests: None.
Funding: The study was supported by unconditional grants from the Zurich Lung League, Switzerland, and Weinman AG, Switzerland.
Ethics approval: The study protocol was approved by the local ethics committee.
▸ An appendix is published online only at http://jnnp.bmj.com/content/vol80/issue3