Article Text

Abstract
Background Intravenous recombinant tissular plasminogen activator (rt-PA) is the only approved pharmacological treatment for acute ischaemic stroke. The authors aimed to analyse potential causes of the variable effect on early course and late outcome.
Methods and results 136 patients (42% women, 58% men) treated with intravenous rt-PA within 3 h of stroke onset in an acute stroke unit over a 3-year period, were included. Early clinical profiles of evolution at 48 h were divided into clinical improvement (CI) (decrease >4 points in the National Institute of Health Stroke Scale (NIHSS)); clinical worsening (CW) (increase >4 points NIHSS); clinical worsening after initial improvement (CWFI) (variations of >4 points in the NIHSS). Patients with clinical stability (no NIHSS modification or <4 points) were excluded. The patients showed in 66.9% CI, 13.2% CW 8.1 % CWFI and 11.8% remained stable. Female sex, no hyperlipaemia and peripheral arterial disease were associated with CW. Male sex and smoking were associated with CI. Absence of arterial occlusion on admission (28.4%) and arterial recanalisation at 24 h were associated with CI. Main causes of clinical deterioration included symptomatic intracranial haemorrhage (sICH), persistent occlusion and cerebral oedema. 23.5% developed ICH, 6.6% of which had sICH. At 3 months, 15.5% had died. Mortality was increased in CW, mainly related to sICH and cerebral oedema. The outcome of CWFI was intermediate between CW and CI.
Conclusions Early clinical profiles of evolution in thrombolysed patients vary considerably. Even with CI, it is critical to maintain vessel permeability to avoid subsequent CW.
- Fibrinolysis
- cerebral ischaemia
- thrombolysis
Statistics from Altmetric.com
Introduction
Intravenous recombinant tissular plasminogen activator (rt-PA) has been approved in 1996 by the Food and Drugs Administration for the USA and in 2002 by the European Medicines Agency for Europe, for acute stroke treatment within 3 h of stroke onset. After intravenous rt-PA treatment, clinical evolution varies, with minimal or no changes in clinical status, improvement or worsening, sometimes after some clinical improvement. The aim of our study was to analyse the causes of these clinical profiles of evolution within 48 h after intravenous rt-PA treatment in a thrombolysed stroke population.
Methods
We studied consecutive patients treated with intravenous rt-PA at a University Hospital (Centre Hospitalier Universitaire Vaudois—Lausanne). Inclusion criteria were ischaemic stroke in any territory, age 18 years or older (if over 80 years old, treatment depending on prestroke dependency and comorbidity), onset to treatment time ≤3 h, cranial tomography (CT) scan without haemorrhagic lesion and neurological status ≥6 points in the National Institute of Health Stroke Scale (NIHSS). Exclusion criteria were similar to those used in the NINDS study.1 The treatment was initiated in the emergency department after the CT study, using intravenous rt-PA (0.9 mg/kg). Non-contrast CT scan and perfusion CT (P-CT) was performed prior to the rt-PA treatment, whereas intracranial and extracranial angio-CT was usually performed after initiation of rtPA. A repeat CT scan and intra- and extracranial angio-CT were performed at 24 h after the procedure and whenever the patient worsened. If creatinine clearance was <30 ml/min using the Cockroft formula (<50 ml/min if patient on metformin), the patient was not given intravenous contrast. If creatinine clearance was 30–50 ml/min, the patient received 300 ml of isotonic sodium chloride solution in 30 min followed by 1 ml kg−1 h−1 over the following 12 h, and oral N-acetylcysteine for 48 h. None of the patients who received contrast medium developed renal failure.
The P-CT examination consisted of two 40-series at an interval of 5 min, each series consisting of one image per second in cine mode during intravenous administration of iodinated contrast material. The acquisition parameters for both series were 80 kV and 100 mA. For each series, CT scanning was initiated 7 s after the injection of 50 ml iohexol at a rate of 5 ml s−1 into an antecubital vein with a power injector. The time delay before contrast material reached the brain parenchyma allowed the acquisition of baseline images without contrast enhancement. Multidetector-array technology allowed data acquisition from two adjacent 10 mm sections for each series. The two P-CT series thus allowed data acquisition in four adjacent 10 mm cerebral CT sections.2 The mean transit time map results from a deconvolution of the parenchymal time–concentration curves by a reference arterial curve. The deconvolution operation requires a reference arterial input function, the selection of which is automatically performed by the P-CT software. The cerebral blood volume (CBV) map is inferred from a quantitative measurement of the partial size-averaging effect, which is absent at the centre of the large superior sagittal venous sinus. A simple equation combining CBV and mean transit time (MTT) values leads to the cerebral blood flow (CBF) value.2 Penumbra and infarct maps can thus be inferred from relative CBV and relative CBF maps. The cerebral and cervical CT angiography was performed from the origin of the aortic arch branch vessels to the circle of Willis.
Carotid and transcranial duplex were carried out within 48 h after admission. NIHSS, Barthel Index and modified Rankin Scale (mRS) were used to assess clinical status and functional status. Patients who died were given the worst possible score in clinical scales such as the NIHSS. We used the TOAST3 criteria for stroke aetiological classification. Information on demographics, risk factors and previous strokes was obtained from the patient, next of kin and family physician. Pretreatment glycaemia, temperature, cholesterol, fibrinogen, INR, platelet count, blood pressure and haematocrit were recorded.
Clinical profiles of evolution within the first 48 h were divided into clinical improvement (CI), with a decrease of ≥4 points NIHSS; clinical worsening (CW), with an increase of ≥4 points NIHSS; and clinical worsening after initial improvement (CWFI), with a decrease of ≥4 points NIHSS followed by an increase of ≥4 points NIHSS. Patients with clinical stability (no NIHSS modification or <4 points in the NIHSS) were excluded. Patients were observed clinically in a neurological intermediate care unit on an hourly basis during the day and every 3 h at night. We defined intracranial symptomatic haemorrhage (sICH) as clinical worsening of ≥4 points in the NIHSS best attributed to intracranial haemorrhage. Any other ICH was considered as asymptomatic (aICH).
We classified causes of clinical deterioration as symptomatic intracranial haemorrhage (sICH), cerebral oedema, early stroke recurrence defined as an acute onset clinical worsening that was best explained by a new ischaemic event after repeat radiological evaluation, persistent arterial occlusion (or reocclusion) and others (including systemic and unknown causes). Occlusion that was still present at the neuroimaging control study at approximately 24 h was labelled ‘persistent arterial occlusion,’ although we cannot exclude early recanalisation followed by reocclusion in some patients.
Statistical analyses were performed with the SPSS v.13.0 software for Windows (SPSS, Chicago). Standard univariate analyses (χ2, t tests and Mann–Whitney U test) were carried out; and values were given as percentages, means and SD or median and the IQR for descriptive purposes. Kaplan–Meier survival curves were used to examine crude survival. Cox multiple regression analyses for censored survival data were performed to compare survival between subjects with stable or clinical worsening and patients with clinical improvement. This multivariate analysis was also performed to determine the causes of worsening. All analyses were adjusted according to age, sex, onset to lysis, admission NIHSS, hyperlipaemia, diabetes mellitus, high blood pressure (>140 mm Hg/90 mm Hg) and smoking.
The P-CT and angio-CT protocol has been the standard of care for patients with suspected acute supratentorial stroke since 2002 in our institution. The ethical committee for clinical research of the University of Lausanne has approved the retrospective analysis of these patients.
Results
A total of 136 patients fulfilling all criteria were treated: 57/136 (42%) women and 79/136 (58%) men. The mean age was 64.6 years (19–85). The mean stroke onset to fibrinolysis time was 150 min (CI 151 min; CW 143.6 min; CWFI 154.3). Aetiology was cardioembolic in half of the patients. Early clinical profiles were CI in 91/136 patients (66.9%), CW in 18/136 patients (13.2%) and CWFI in 11/136 patients (8.1%). Therefore, of the 102 patients with initial clinical improvement, 11 (10.8%) deteriorated in the following 48 h. The other 16/136 patients (11.8%) remained stable according to our definitions.
Cerebrovascular risk factors
Female sex, no hyperlipaemia and peripheral arterial disease were associated with CW within 48 h (p<0.05). Smoking was associated with CI within 48 h (p<0.01). No correlation was found with previous ischaemic stroke, cardiac disease or antithrombotic treatment on admission (table 1).
Demographic and clinical variables and their relationship with clinical evolution
Neuroimaging studies
Of the 136 patients, 119 (87.5%) had a good-quality P-CT prior to thrombolysis. The P-CT study without perfusion deficit or more penumbra than infarct was related to CI. Still, 3/20 patients (15%) with a normal study and 21/95 patients (22.1%) with more penumbra than core worsened within 48 h (table 2).
Perfusion-CT variables on admission and its relationship with clinical evolution
Of the 136 patients, 127 (93.3%) had good-quality angio-CT at admission; angio-CT study was not possible for renal or technical reasons in nine patients (6.6%) at admission and in four patients (2.9%) at 24 h. On admission, 91/127 patients (71.6%) had intra- and/or extracranial occlusion in the territory of the acute stroke (table 3). Absence of arterial occlusion was associated with CI (p<0.05). Angio-CT at 24 h showed recanalisation in 52/87 patients (59.7%) which was associated with CI (p<0.001).
Angio-CT variables on admission and its relationship with clinical evolution
Most patients (14/20 patients, 70%) with normal P-CT showed no occlusion on angio-CT at admission, 1/20 patients (5%) extracranial occlusion, 2/20 patients (10%) intracranial occlusion and 1/20 patients (5%) extra- and intracranial occlusion. Patients with core>penumbra (three patients) showed arterial occlusion in angio-CT.
Clinical deterioration
In CW, the main causes of worsening were sICH in 6/18 patients (33.3%), persistent arterial occlusion in 6/18 patients (33.3%) and cerebral oedema in 6/18 patients (33.3%) (table 4). In CWFI, the main cause of worsening was persistent arterial occlusion in 8/11 patients (72.7%), followed by systemic causes in 1/11 patients (9%) and unknown causes in 2/11 patients (18.1%) (table 4).
Causes of clinical deterioration
Concerning the time of worsening, in CW, 15/18 patients (83.3%) were within 24 h and 3/18 patients (16.7%) within 36–48 h. The exact time points of worsing were: five patients during the first 12 h (one at 3 h, two at 4 h, and two at 12 h); 10 patients in 12–24 h (eight at 12–24 h, two at 24 h); two patients at 36 h; and one patient at 40 h. In CWFI, 10/11 patients (90.9%) had initial worsening within 24 h, and 1/11 patients (9.1%) one at 48 h. The exact time points of worsening before improvement were: five patients during the first 12 h (one at 2 h, one at 3 h, one at 10 h, one at 12 h and one at 12 h); three patients during 12–24 h; two patients at 24 h; and one patient 48 h.
Within 24 h, 32/136 patients (23.5%) had ICH, and 9/136 patients (6.6%) showed sICH.
Outcome at 3 months
At 3 months, 21/135 available for follow-up patients had died (15.5%), 13 females and eight males. In these patients, stroke aetiology was predominantly cardioembolic (52%).
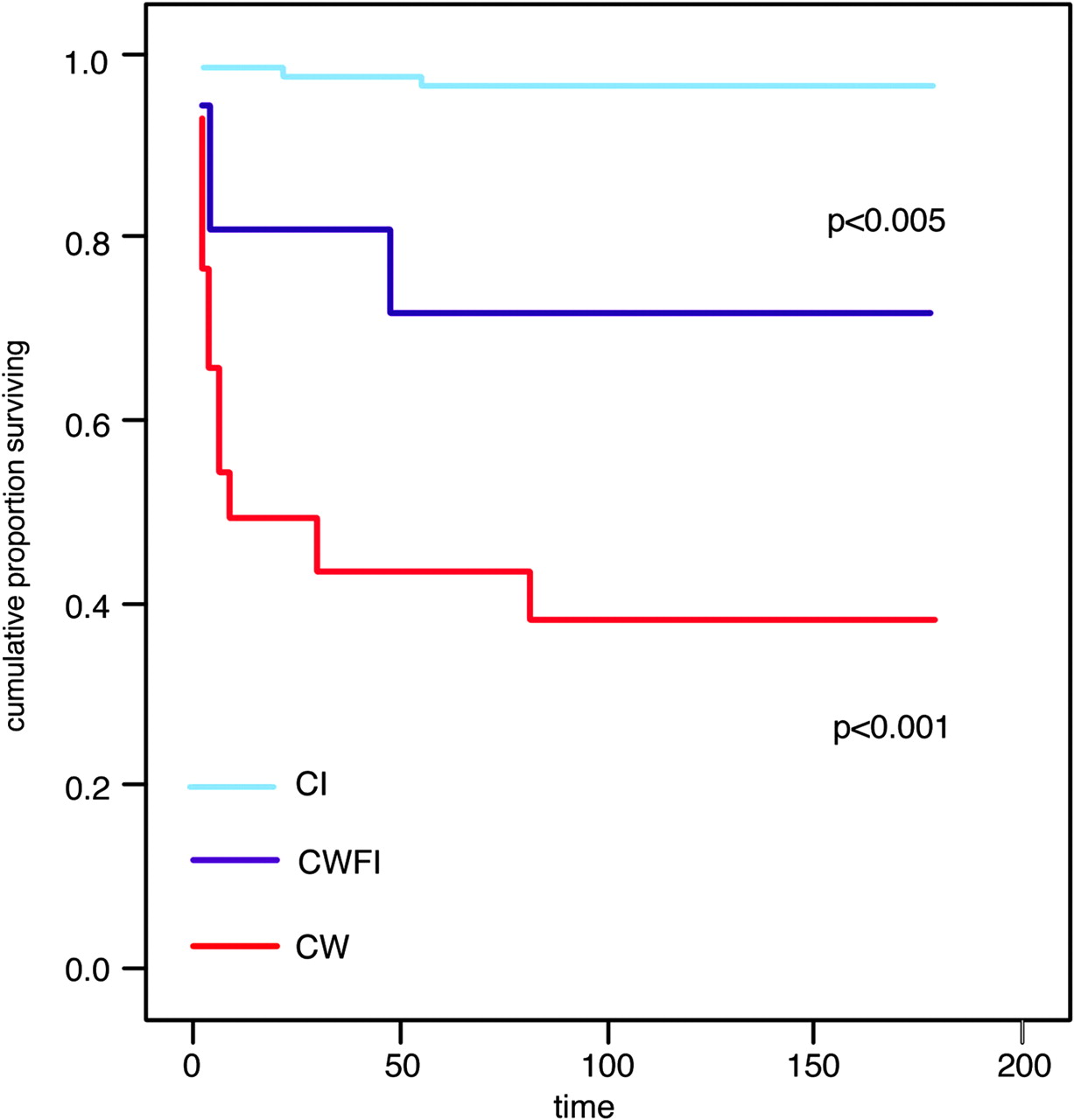
Of the patients who died, two patients were in the CI group, 11 patients in the CW group and three patients in the CWFI group (figure 1). Compared with the CI group, the multivariate analysis showed a higher mortality risk in the CW group (RR=43.6, 95% CI 9.6 to 197.8) and in the CWFI group (RR=14.7, 95% CI 2.4 to 88.1).

Mortality at 3 months regarding clinical evolution. CI, clinical improvement; CW, clinical worsening; CWFI, clinical worsening after initial improvement.
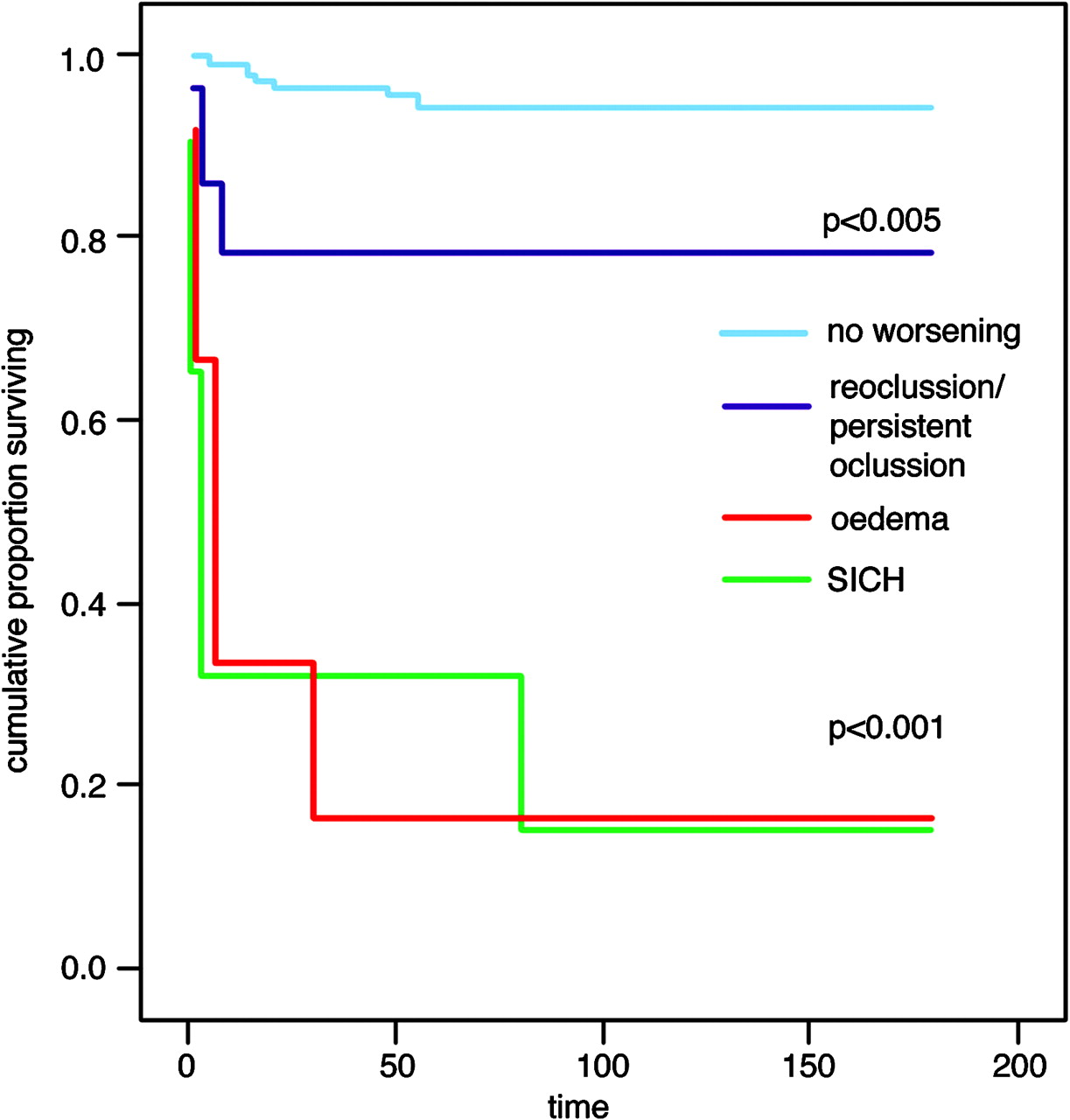
The Kaplan–Meier curve showed that mortality was higher in sICH and oedema (figure 2). After adjustment for potential confounders (age, sex, onset to lysis, admission NIHSS, hyperlipaemia, diabetes mellitus, high blood pressure and smoking), the presence of sICH increased the risk of mortality (RR=30.0, 95% CI 9.0 to 100.1). aICH was not associated with mortality. In addition, the presence of oedema and persistent occlusion also increased the mortality risk (RR=29.1, 95% CI 8.6 to 97.7 and RR=4.3, 95% CI 1.0 to 17.4, respectively).
{kind=link}
{kind=link}
Mortality at 3 months regarding causes of worsening. SICH, symptomatic intracranial haemorrhage.
Discussion
In this series of thrombolysed patients, we found that CW was related to female sex, no hyperlipaemia and peripheral arterial disease, whereas CI was related to male sex and smoking. Moreover, CI was related to absence of arterial occlusion and arterial recanalisation, whereas CW and CWFI were associated with persistent arterial occlusion.
Cerebrovascular risk factors
Female gender was associated with early clinical worsening in our study, which in turn was associated with increased mortality. This is in line with a generally increased stroke mortality in women.4 This contrasts with reports of higher response to thrombolysis in women in some studies5 6 but not in others.7
Our study supports previous observations of a beneficial effect of smoking on better functional outcome,8 although we have not observed a protective role against. ICH.9
Absence of hyperlipaemia was correlated with CW, and there were more patients without hyperlipaemia in the sICH group (7:2). A neuroprotective effect of cholesterol has also been postulated.10
Peripheral arterial disease is closely associated with coronary and carotid atherosclerosis.11 The relationship with CW in our study may be due to this association.
We did not find any differences either in previous ischaemic cerebrovascular events or in previous antithrombotic treatment for early clinical evolution after intravenous thrombolysis.
Given the small number of patients examined in our study, some correlations between clinical and radiological variable and clinical evolution may be over- or underestimated.
Neuroimaging studies
In our patients, a normal perfusion study or a larger penumbra than infarct volume was correlated with CI. Still, nearly a quarter of these patients had CW (sometimes after initial improvement). Whereas patients with a large penumbra may benefit more from recanalisation, non-recanalisation in these patients may lead to death of at-risk tissue,12–14 explaining CW or CWFI in some of them. Cases have been described using P-CT as exclusion criteria for intravenous thrombolysis treatment,15 intravenous thrombolysis within 3 and 6 h15 16 and in unknown stroke onset.17
We confirmed previous observations that arterial recanalisation in angio-CT was associated with CI.18 Similarly, mortality was greater at 3 months in patients with persistent occlusion at 24 h. We also found a greater tendency towards CI in patients with MCA occlusions than in patients with associated internal carotid artery (ICA) occlusions. ICA occlusions have been described as being more resistant to intravenous treatment than middle cerebral artery (MCA) occlusions,1 vertebral arteries and basilar artery.18 Thrombus burden may explain this response.18
Persistent occlusion and arterial reocclusion correlates with clinical deterioration, though the latter has a better prognosis than the former, because a temporary recanalisation may allow for a partial penumbra rescue.19
Early clinical deterioration and outcome at 3 months
Approximately 15% of patients with stroke (spontaneously or after intravenous thrombolysis) may have worsening after initial improvement.20 Clinical progression usually occurs within 48 h but was seen as late as 96 h in 13% patients.21
In our study, cerebral oedema, sICH and persistent arterial occlusion contributed equally with CW. Patients of this group had the worst clinical and functional prognosis and greater mortality at 3 months.
Any ICH was observed in 23.5% of patients, less than in the ECASS studies (48.4% within the first week in ECASS II22). SICH as defined by ECASS criteria was observed in 6.6% of patients, somewhat more than in the ECASS-II. A correlation was observed between no ICH and CI, and between ICH and CW. Moreover, ICH and cerebral oedema patients had the worst clinical and functional prognostic at 3 months. Among ICH, aICH had no influence in the clinical prognosis.
Our patients with CWFI were characterised by persistent arterial occlusion at 24 h and a better outcome than CW patients. CWFI has been described in 13% of patients in the literature. Arterial reocclusion1 is suspected as the main cause of CWFI.19 However, some authors did not find any differences between patients treated and those not treated with rt-PA in clinical deterioration, which supports evidence against reocclusion.23 As we did not perform early (<6 h) or continuous monitoring of the arterial patency in our study, we do not know the frequency of early recanalisation followed by reocclusion in our patients.
The improved functional prognosis in CWFI group as compared with CW may be explained by penumbra rescue from temporary recanalisation, as mentioned above.
Conclusions
We conclude that early clinical profiles of evolution after intravenous rt-PA treatment in an unselected stroke population vary considerably. It can be predicted by vascular risk factors, perfusion patterns and arterial pathology. Patients with no hypoperfusion or with large penumbras, and patients with early and persistent recanalisation seem to have a more favourable early and late outcome.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the Commission D'Ethique de la Recherche Clinique, Université de Lausanne.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.