Article Text

Abstract
Objectives To report cerebral blood flow changes during attacks of hemiplegic migraine with prolonged aura (HMPA) longer than 24 h in patients with familial hemiplegic migraine (FHM) with a novel gene mutation.
Methods The authors performed serial neuroimaging studies during acute stage and after recovery of aura symptoms in eight HMPA attacks in two affected individuals of the Japanese family of FHM during a 10-year-observational period. The authors also performed a mutational analysis for all exons of the CACNA1A, ATP1A2 and SCN1A genes in three individuals of this family.
Results Each patient had an individual ‘predominantly affected hemisphere,’ that is, susceptible to hemiplegia during an HMPA attack. Migraine aura lasted 4 to 12 days. Neuroimaging studies performed on days 1 to 4 showed hyperperfusion in the affected hemisphere contralateral to hemiplegia in five attacks, hypoperfusion in three, middle cerebral artery vasodilation in five and augmented vasogenic leakage with cortical oedema in one. Hyperperfusion developed more frequently than hypoperfusion in the ‘predominantly affected hemisphere,’ whereas only hypoperfusion developed in the ‘non-predominantly affected hemisphere.’ All changes were fully reversible. The authors identified a novel heterozygous p.H916L mutation in the ATP1A2 gene in all three individuals.
Conclusions Although the perfusion state could be different depending on the time course of migraine or the timing of scans in relation to cortical spreading depression, prolonged aura symptoms in this family were frequently associated with hyperperfusion and middle cerebral artery vasodilation. Hyperperfusion tended to occur in the ‘predominantly affected hemisphere,’ but the mechanism of HMPA awaits further investigations on additional cases of FHM2.
- Familial hemiplegic migraine
- prolonged aura
- cerebrovascular Circulation
- spect
- ATP1A2 gene
- headache
- mitochondrial disorders
- migraine
Statistics from Altmetric.com
- Familial hemiplegic migraine
- prolonged aura
- cerebrovascular Circulation
- spect
- ATP1A2 gene
- headache
- mitochondrial disorders
- migraine
Introduction
Typical migraine aura usually resolves within 60 min, but aura in hemiplegic migraine often persists longer than an hour. The duration of each aura symptom in hemiplegic migraine is now defined to be less than 24 h.1 The mechanisms that underlie hemiplegic migraine may be different from the usual migraine. Three genes have been identified as being responsible for familial hemiplegic migraine (FHM); CACNA1A (calcium channel, voltage-dependent, P/Q type, α 1A subunit),2 ATP1A2 (ATPase, Na+/K+-transporting, α 2 (+) polypeptide),3 and SCN1A (sodium channel, voltage-gated, type I, α subunit) genes.4 These mutations are considered to cause neuronal hyperexcitability predisposing to cortical spreading depression (CSD).5 Typical migraine aura is believed to be a primary neuronal event reflecting a propagating wave of neuronal and glial depolarisation in the cerebral cortex similar to CSD.6 Propagation of CSD causes transient hyperaemia, followed by long-lasting oligaemia.7 Hypoperfusion8–12 or normoperfusion13–15 has been reported to be associated with migraine aura, but hyperperfusion has also been documented in the area corresponding to prolonged aura during a hemiplegic migraine attack.16–21
We previously reported a 35-year-old woman as a case of sporadic hemiplegic migraine, in which we demonstrated focal hyperperfusion with augmented vasogenic leakage in the affected cortex corresponding to prolonged aura.21 After publication, her mother, who initially denied having migraines, was admitted to our hospital with hemiplegic migraines at 66 years of age. This prompted us to search for a gene mutation in this family.
In this study, we aimed to assess the regional cerebral blood flow (CBF) changes associated with prolonged aura, and to identify any gene mutations.
Patients and methods
Subjects
Three members of this family were enrolled in this genetic study (figure 1A). The proband (III-1: patient 1) and her mother (II-3: patient 2) had hemiplegic migraines fulfilling the criteria of the International Classification of Headache Disorder (2nd edition).1 The proband, a 42-year-old woman, had had migraines since 12 years of age, while her mother, a 69-year-old woman, had had migraines since 38 years of age. Her younger sister, a 39-year-old woman (III-2: patient 3), was initially considered to be asymptomatic but recently developed a first migraine attack with leg weakness at 39 years of age, and then she began to reveal that she had had migraines without auras since the age of 12. She had only one attack of migraine with motor weakness; therefore a diagnosis of probable hemiplegic migraine was used in the pedigree. All three subjects had febrile convulsion during early childhood but no ataxia. The maternal family history of the proband, including her grandfather, grandmother and three aunts, revealed no headaches or ataxia. All patients are described in detail in the supplementary material (online appendix e-1).

Pedigree of the family and gene analysis. Circle, female; square, male; black, hemiplegic migraine; left half black, probable hemiplegic migraine; white circles or squares, individuals without migraine, +/−, presence of heterozygous mutation. The arrow indicates the proband (A). Mutational analysis shows a heterozygous p.H916L mutation in the ATP1A2 gene (B). Schematic representation of the ATP1A2 protein shows the location of the p.H916L mutation (C, star sign) and pathogenic mutations reported to date. The residue is highly conserved across species on ATP1A2 (D).
In this study, we defined ‘hemiplegic migraine with prolonged aura (HMPA)’ as hemiplegic migraine with prolonged aura symptoms for longer than 24 h, and the ‘affected hemisphere’ as the cerebral hemisphere contralateral to hemiplegia.
Neuroimaging studies
Patients 1 and 2, who were repeatedly admitted to our hospital with HMPA, underwent serial neuroimaging studies, including CBF single-photon emission computed tomography (SPECT), three-dimensional time-of-flight MR angiography (3D-TOF MRA), diffusion-weighted MRI (DWI), fluid-attenuated inversion recovery (FLAIR) image, and EEG during the acute stage and after the recovery from aura symptoms in eight consecutive attacks of HMPA. The first neuroimaging studies were performed on days 1 to 4 when the patient had headache and aura symptoms (table 1). Enhanced FLAIR imaging was performed using standard procedures in six attacks; in three of these, enhanced FLAIR late images were obtained 2 h after intravenous injection of gadolinium to assess cerebrospinal fluid signal changes in the sulci of the affected cortex.22 Proton MR spectroscopy ((1)H-MRS) was performed using a single- or multivoxel analysis in two attacks to assess changes in MR spectra in the affected cortex, including the visual and non-visual cortex. MRI was performed with a Signa 1.5 T.
Clinico-radiological features during attacks of hemiplegic migraine with prolonged aura (HMPA)
In CBF SPECT, we used 99mTc-d,l-hexamethyl-propyleneamine oxime (740 MBq) as a flow tracer in the initial two attacks in patient 1, and N-isopropyl-p-123I iodoamphetamine (IMP) (167 MBq) in the remaining six attacks (table 1). IMP-SPECT acquisitions were performed using two-head rotating γ cameras (Siemens, Asahimedic ECAM+) equipped with 123I-specific fan-beam collimators. Autoradiography method with one-point arterial blood sampling23 was used in IMP-SPECT for quantitative CBF measurement, in which arterial input data were obtained by one-point arterial blood sampling 10 min after IMP infusion. The regional CBF was assessed using a 3D-stereotactic surface projection technique (Z-score mapping). Both hyperperfusion and hypoperfusion images were created from our control database (online appendix e-1). The regional CBF in the affected hemisphere was assessed based on a visual analysis, quantitative CBF measurement and 3D-stereotactic surface projection mapping.
Mutational analysis
In three members, we performed a genetic analysis for all exons of the CACNA1A and ATP1A2 genes using a DNA microarray-based high-throughput resequencing system.24 We also analysed the SCN1A gene by direct nucleotide sequence analysis. Genomic DNA was isolated from peripheral blood by standard procedures, and then nucleotide sequences were analysed using a resequencing DNA microarray. The obtained sequence variations were confirmed by direct nucleotide sequence analysis (online appendix e-2) and compared with those in the human gene-mutation database (http://www.hgmd.cf.ac.uk/ac/index.php). For the putative pathogenic mutations, further direct nucleotide sequence analyses were conducted using genomic DNAs from 260 unaffected Japanese individuals (560 chromosomes).
Studies were approved by Institutional Review Boards of Kitasato University and the University of Tokyo, and written informed consent was obtained from all subjects.
Statistical analysis
Statistical analyses were carried out using JMP (SAS V.6.0.3). Contingency tables were analysed with a Fisher two-sided exact test for CBF pattern in the affected hemisphere.
Results
Clinical features
Patient 1 had eight HMPA attacks requiring hospitalisation up to the age of 42 years, while patient 2 had four attacks up to the age of 69 years. Eight of the 12 attacks are summarised in table 1. The remaining four attacks were not included because of hospitalisation to another hospital. Both patients were neurologically intact during the interictal period. Premonitory symptoms, including increased appetite, fatigue or somnolence, often developed a few weeks before the onset of HMPA.
The body temperature was always elevated on admission and began to elevate along with exacerbation of headache or aura symptoms, but no attack was preceded by a flu-like illness. Although patient 1 developed left hemiplegia in two out of eight HMPA attacks, she stated that she developed right hemiplegia in most of the attacks, including those not requiring a hospitalisation. In contrast, patient 2 developed left hemiplegia in all four HMPA attacks. It is suggested that each patient had individual ‘predominantly affected hemisphere,’ that is, susceptible to hemiplegia during the HMPA attack.
Headaches usually began unilaterally, contralateral to hemiplegia, but the headache severity was difficult to evaluate owing to concomitant aphasia, psychiatric symptoms or altered level of consciousness. Hemiplegia was usually mild or moderate, and the severity fluctuated markedly. Headaches often intermingled with hemiplegia and fluctuated during the course of HMPA. Aura symptoms included aphasia, agnosia, apraxia or homonymous hemianopsia. These patients also had psychiatric symptoms, including fear, anxiety, agitation, delusion and hallucination, but no seizure developed. There was no sign of lateralised autonomic symptoms, such as pupil changes or flushing in the side of the affected hemisphere.
Both patients received corticosteroids during the active phase of six of eight attacks of HMPA: either prednisone (60 mg/day, 3–5 days) or intravenous high-dose methylprednisolone (1000 mg/day, 3 days) followed by a short taper (table 1). The rationale for the use of corticosteroids was based on clinical improvement to corticosteroids at the second attack of patient 1 when augmented vasogenic leakage with cortical oedema was demonstrated in the sulci of the affected cortex on day 4.21 The first imaging studies were obtained before administration of corticosteroids (table 1). Severe headache, emesis and prominent psychiatric symptoms began to improve after initiation of corticosteroids, while aphasia, weakness, hemianopsia or nocturnal visual hallucination gradually resolved. Psychiatric symptoms were not related to corticosteroid therapy, but prominent psychiatric symptoms required short-term use of propofol or tiapride. Aura symptoms persisted substantially for 4 to 12 days, and all symptoms were fully reversible. There was no distinct clinical feature in the second attack with vasogenic leakage compared with those without leakage (table 1).
During recovery of symptoms, these patients were empirically treated with lomerizine hydrochloride 10 mg/day (flunarizine analogue), topiramate 100 mg/day or amitryptyrine 10 mg/day or combinations of these medicines. Both patients began to receive lomerizine when they had aura symptoms, which were after the first neuroimaging studies were obtained.
Neuroimaging studies
SPECT
CBF-SPECT showed unilateral hyperperfusion in the affected hemisphere in five of eight attacks (figures 2–4), and hypoperfusion in the remaining three attacks (figures 2, 4).

N-Isopropyl-p-123I iodoamphetamine single-photon emission computed tomography during the acute stage of four attacks of hemiplegic migraine with prolonged aura (patient 1). Blood-flow single-photon emission computed tomography shows focal hyperperfusion in the left frontotemporal cortex (A, third attack at age 36 years) and left anterior frontal cortex (B, fourth attack at age 40 years), but hypoperfusion in the right hemisphere (C, fifth attack at age 42 years) and the left hemisphere (D, sixth attack at age 42 years). Crossed cerebellar diaschisis occurred during three attacks (A, B and D). Two selected axial images and hyperperfusion and hypoperfusion 3D-stereotactic surface projection images are shown. Yellow arrows reveal hyperperfusion in the affected hemisphere, while light blue arrows reveal hypoperfusion in the affected hemisphere.

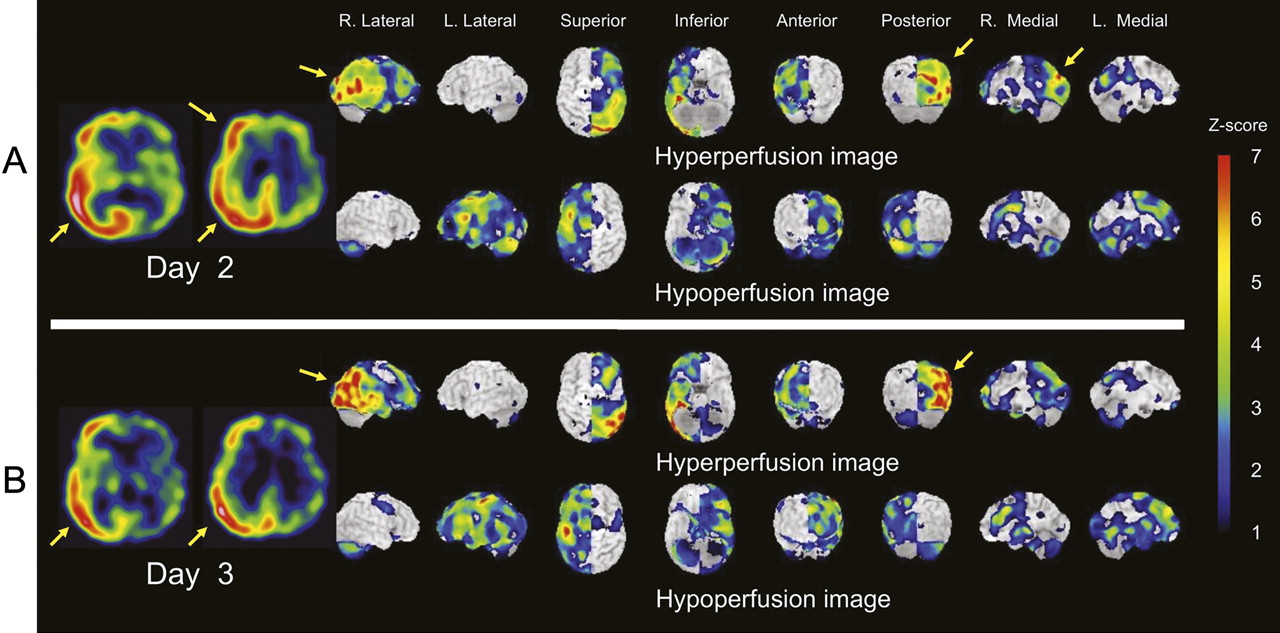
N-Isopropyl-p-123I iodoamphetamine single-photon emission computed tomography during the acute stage of two attacks of hemiplegic migraine with prolonged aura (patient 2). Blood-flow single-photon emission computed tomography shows focal hyperperfusion in the right posterior hemisphere (A, seventh attack at age 66 years) and (B, eighth attack at age 68 years). Two selected axial images, and hyperperfusion and hypoperfusion 3D-stereotactic surface projection images are shown. Yellow arrows reveal hyperperfusion area in the affected hemisphere.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time-of-flight MR angiography (MRA) and 99mTc-d,l-hexamethyl-propyleneamine oxime single-photon emission computed tomography during two attacks of hemiplegic migraine with prolonged aura (patient 1). The initial MRA shows prominent cortical branches of the right middle cerebral artery (MCA) despite extensive hypoperfusion in the right hemisphere contralateral to left hemiplegia during the acute stage of the first attack (A, age 33 years), but follow-up studies show no abnormal findings on MRA and single-photon emission computed tomography (B). During the second attack, MRA shows prominent cortical branches of the left MCA and marked hyperperfusion in the left posterior hemisphere (C, age 35 years). White arrows reveal a prominence of MCA branches, light blue arrows reveal hypoperfusion, and yellow arrows reveal hyperperfusion in the affected hemisphere.
Regardless of perfusion patterns, the CBF in the cerebellum contralateral to the affected cerebral hemisphere was reduced in six of eight attacks (75%), but not in the remaining two attacks. Hypoperfusion in the contralateral cerebellum (contralateral cerebellar hypoperfusion) is likely to be crossed cerebellar diaschisis (CCD), which is decreased metabolism and blood flow in the cerebellar hemisphere contralateral to a cerebral lesion.25 CCD is also reported in a case of cerebral hyperperfusion following carotid endarterectomy.26 Therefore, we used the term ‘CCD’ for contralateral cerebellar hypoperfusion associated with prolonged aura originating from unilateral hemisphere (table 1).
Hyperperfusion developed frequently in the ‘predominantly affected hemisphere’ (five of six attacks; second, third, fourth, seventh, eighth attacks), whereas hypoperfusion developed in the ‘non-predominantly affected hemisphere’ (two of two attacks; first, fifth attacks) but less frequently in the ‘predominantly affected hemisphere’ (one of six attacks; sixth attack). Although there was no significant difference in perfusion pattern between the ‘predominantly affected’ and ‘non-predominantly’ affected hemispheres (Fisher exact test, p=0.107), hyperperfusion was seen more frequently than hypoperfusion in the ‘predominantly affected hemisphere’ (83% vs 17%).
Interestingly, we noticed that the region of cortical hyperperfusion moved associated with changes in neuropsychiatric symptoms. For example, during one attack (second attack) SPECT showed continuous spread of focal hyperperfusion from the left posterior cortex (on day 2) to the ipsilateral anterior frontal cortex (on day 4) associated with exacerbation of disinhibited frontal-lobe syndrome.
MRA
3D-TOF MRA showed prominent dilation of the middle cerebral artery (MCA) branches in the affected hemisphere in two attacks, mild dilation of the MCA branches in three, mildly decreased visualisation of MCA branches in one and no laterality in the remaining two attacks (table 1). When compared with SPECT findings, MRA showed unilateral vasodilation accompanied by ipsilateral hyperperfusion in four attacks (figure 4C, second, fourth, seventh, eighth attacks). On the other hand, unilateral vasodilation despite ipsilateral hypoperfusion was seen in one (figure 4A, 1st attack) and unilateral possible vasoconstriction despite ipsilateral focal hyperperfusion in one (fourth attack).
DWI/FLAIR
DWI did not reveal any acute ischaemic lesion. Conventional enhanced FLAIR imaging did not reveal any abnormal cerebrospinal fluid enhancement, but enhanced FLAIR late imaging revealed augmented vasogenic leakage in the sulci of severely affected cortex with cortical oedema in one of three attacks (second attack). No cortical oedema was seen in the other seven attacks.
MRS
MRS did not reveal any abnormal spectrum peak, including N-acetylaspartate, choline, creatine, phosphocreatine and lactate, in the affected hemisphere including the visual cortex in two attacks.
EEG
EEG showed low-voltage slowing with attenuation of α waves in the affected hemisphere in all seven attacks, but no paroxysmal discharge was seen.
All of the above findings resolved after the recovery of symptoms.
Mutational analysis
Using a resequencing DNA microarray technique, we identified a novel heterozygous p.H916 L (c.2747A>T) mutation in the exon 20 of the ATP1A2 gene in all three subjects (figure 1B). This c.2747A>T transversion was further confirmed by direct nucleotide sequence analysis. This missense mutation was not detected in 260 Japanese unaffected individuals (520 chromosomes) and not described in the Human Gene Mutation Database. This mutation was located in the 8th transmembrane segment of the ATP1A2 protein (figure 1C). The residue is highly conserved across species (figure 1D) (http://www.ncbi.nlm.nih.gov/homologene). No mutations were detected in the exons of CACNA1A or SCA1A gene.
Discussion
This is the first CBF study performed in multiple attacks of HMPA of different individuals within a family of FHM2. Although only two patients were included in this study, and the results may not be generalised to other families, this long-term observational study revealed the following findings. First, each patient had an individual ‘predominantly affected hemisphere’. Second, both patients had premonitory symptoms and an elevated body temperature. Third, hemiplegia and headache intermingled and fluctuated during the course of HMPA. Fourth, hyperperfusion with MCA vasodilation was frequently seen in the ‘predominantly affected hemisphere,’ but vasogenic leakage was seen in only one attack. Finally, we identified a novel p.H916L ATP1A2 mutation in this family.
Our patients had an individual ‘predominantly affected hemisphere,’ but this lateralisation is not surprising because it is well known that one side of the body could be affected exclusively or predominantly in patients with hemiplegic migraine.27 Unilateral pain is a hallmark of migraine and is often ‘lateralised’ to one side of the head. The mechanism of ‘lateralisation of pain’ is not fully understood, but a PET study revealed the presence of ipsilateral brainstem dysfunction in migraineurs.28 Although premonitory symptoms have never been described in FHM2 with known mutations, our patients had long-lasting premonitory symptoms, including increased appetite or somnolence, implying hypothalamic dysfunction preceding the onset of HMPA, although no flow change was found in the diencephalon or brainstem.
After our experience of the second attack with vasogenic leakage, we administered corticosteroids as early as possible after the onset of symptoms to prevent development of vasogenic leakage in the subsequent attacks, except one (third attack). Vasogenic leakage or cortical oedema was seen in only a single attack at the peak of the symptoms, suggesting that these MRI changes likely reflect a part of the clinical syndrome but not a cause of prolonged aura, although early intervention with corticosteroids might have suppressed vasogenic leakage or oedema. Although it is difficult to assess clinical efficacy of corticosteroids based on this small study, and we cannot exclude the possibility of spontaneous recovery, some of the severe symptoms, such as headache, emesis and prominent psychiatric symptoms tended to improve after initiation of corticosteroids.
Most of the previous studies on CBF were based on a single attack of HMPA,10–21 and no study has been conducted to address serial CBF changes in repeated attacks of the same individual. There are only a few reports on CBF in genetically determined FHM.13 15 We confirmed unilateral hyperperfusion in the affected hemisphere corresponding to prolonged aura symptoms in repeated attacks of HMPA. In addition, we found unilateral hypoperfusion in the same individual despite similar attacks of HMPA, but hyperperfusion developed more frequently than hypoperfusion in the ‘predominantly affected hemisphere.’
In a case of extensive interhemispheric difference in CBF, it is difficult to determine which hemisphere is indeed involved based on SPECT without relevant clinical data. Therefore, we defined the ‘affected hemisphere’ as a ‘cerebral hemisphere contralateral to hemiplegia.’ Functional alteration of the affected hemisphere was also supported by the presence of a visual-field defect, low-voltage slowing on EEG and crossed cerebellar hypoperfusion. Selection bias for the affected hemisphere is unlikely to affect the results.
One might argue also that the perfusion state could be different depending on the time course of migraine or timing of the scan in relation to the onset of CSD, as CSD may occur in clusters in hemiplegic migraine. In migraine with a typical visual aura, occipital CBF decreases during visual aura and returns to normal or increases after resolution of aura symptoms or associated with development of headache.6 8 In contrast, in our series of HMPA, the clinical time course was different; headache and aura symptoms were intermingled and fluctuated over 4 to 12 days. Unilateral or focal hyperperfusion was repeatedly seen in two attacks, and observed at five attacks on days 2 to 8 when the patient had prolonged aura symptoms; however, unilateral hypoperfusion was also seen in the other three attacks on days 1 to 2. Further studies are necessary to confirm the time-course-dependent changes in CBF.
Another important issue includes changes in tracer kinetics in the pathological conditions. A focal increase in tracer accumulation may not directly reflect increased CBF in the affected cortex. We confirmed augmented vasogenic leakage in one severe attack,21 in which a dysfunction of the blood–brain barrier might contribute in part to increased tracer accumulation, but extensive hemispheric hyperperfusion without cortical oedema is not explained by vasogenic leakage alone. In most attacks, increased tracer accumulation is likely attributed to increased CBF. We used two different flow tracers, but both hypo- and hyper-perfusion patterns were seen with either tracer. We analysed only an early image of IMP-SPECT that reflected CBF. Different flow tracers did not seem to affect the results.
It is important to note that the cerebrovascular response was different, depending on the individual hemispheric susceptibility to hemiplegia. Hyperperfusion frequently developed in the ‘predominantly affected hemisphere,’ whereas hypoperfusion developed in the ‘non-predominantly affected hemisphere’ but less frequently in the ‘predominantly affected hemisphere.’ Although the interhemispheric difference in cerebrovascular response may be coincidental owing to the small numbers of subjects studied, a tendency of hyperperfusion in the ‘predominantly affected hemisphere’ may reflect clustering of CSD in the affected hemisphere intrinsically susceptible to hemiplegia. Hypoperfusion in the ‘non-predominantly affected hemisphere’ may reflect decreased cortical metabolism following CSD.
Although the previous 3T MRA study did not reveal any detectable vasodilation of cerebral blood vessels during a nitroglycerine-induced migraine attack,29 unilateral vasodilation of cerebral blood vessels has been reported in several cases of hemiplegic migraine.14 17 21 30 31 We also confirmed a similar vasodilation in multiple attacks in our family. Unilateral MCA vasodilation was seen with ipsilateral hyperperfusion in four attacks, but in the remaining four attacks we found discrepancies between MRA and SPECT, including unilateral vasodilation despite ipsilateral hypoperfusion and possible vasoconstriction despite ipsilateral hyperperfusion. The discrepancy may be explained by the difference in methodologies, parameters, timing of scans or target blood vessels (surface vessels vs parenchymal vessels). MRA detects the flow-related blood signal in the blood vessels at the surface, which are heavily innervated by sympathetic fibres, parasympathetic fibres and trigeminal nerve fibres,32 whereas intracortical parenchymal arterioles are tightly regulated by local neuronal and astrocytic mechanisms.33 34 Ascending projections from the brainstem nuclei also modulate the cortical arterial diameter.32 In one attack (first attack), MRA showed prominent MCA dilation despite ipsilateral hypoperfusion (figure 4A), in which MRA was performed on day 3 (1 day after SPECT). MCA dilation is presumably caused by sustained intense activation of the ipsilateral trigeminal and parasympathetic nerves following CSD. In another attack (fourth attack), MRA showed decreased signals of the MCA branches despite frontal hyperperfusion, in which MRA was performed on day 1 (1 day before SPECT). Transient vasoconstriction may occur, but we observed these phenomena in only one attack. We need further evidence for possible involvement of vascular changes in hemiplegic migraine.
This study provided a link between clinico-pathophysiological features and the ATP1A2 gene mutation. To date, approximately 70 mutations in the ATP1A2 gene have been identified associated with hemiplegic migraine or other phenotypes, including cerebellar ataxia, epileptic seizure or developmental delay (figure 1C). Half of the mutations are clustered in the intracellular loop connecting the fourth and fifth transmembrane segments, but 13 mutations have been reported in the transmembrane segments. This H916 L mutation is the second identified in the eighth transmembrane segments following Q927P.35 This mutation was not detected on 520 control chromosomes, and the residue is highly conserved among species, suggesting that this mutation is likely to be pathogenic. Febrile convulsion and elevated body temperature are probably associated with the mutation as previously reported in FHM2,35 36 but not specific for ATP1A2 mutations because fever or epilepsy has been described in FHM1 or FHM3.37 38 We found cortical oedema with vasogenic leakage in one attack, but similar findings are also reported in FHM239 or FHM1.40
One of the possible explanations for hemiplegic migraine in FHM2 includes loss of function of the Na+/K+-ATPase pump, which maintains the Na+ gradient in astrocytes. Loss of the Na+ gradient is thought to impair glutamate transporters, resulting in decreased glutamate clearance from the synaptic cleft. An increase in the level of extracellular glutamate is believed to cause neuronal hyperexcitability, predisposing the cortex to CSD.5 An increase in the extracellular glutamate level may also activate astrocytes through the metabotropic glutamate receptor, leading to intracellular Ca2+ signalling.33 34 Astrocyte Ca2+ signalling is considered to control synaptic-activity-dependent arteriolar dilation through astrocyte-derived molecules.33 34
The mechanism of uncoupling hyperperfusion to depressed neuronal activity remains speculative. Based on the current concept of neuron–astrocyte communications,33 34 we may propose that dilation of the large surface blood vessels is mainly caused by sustained activation of the ipsilateral trigeminovascular and parasympathetic nerves through vasoactive molecules, including calcitonin gene-related peptide, acetylcholine, vasoactive intestinal peptides or nitric oxide,32 whereas hyperperfusion could be attributed to the ipsilateral parenchymal arteriolar dilation by generation of astrocyte-derived vasodilators. Hyperperfusion may also be attributed to dilation of cortical surface vessels. Although there is no direct evidence of astrocytic activation, activation of the trigeminovascular system, including the trigemino-autonomic reflexes, which is sustained and intensified by astrocytic activation associated with ATP1A2 gene mutation, may cause prominent vasodilation and status migrainosus. This may also cause blood–brain barrier disruption, resulting in augmented vasogenic leakage and cortical oedema in some attacks; however, the mechanism of complex pathophysiology of HMPA remains to be elucidated.
Acknowledgments
We are extremely grateful to all participants for their contribution to this study, and acknowledge the efforts of all research staffs, who worked on the clinical and neuroimaging data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This study was supported in part by a grant from Research on Psychiatric and Neurological Diseases and Mental Health (H20-KOKORO-020).
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval for this genetic study was provided by the institutional review board in both Kitasato University and the University of Tokyo.
Provenance and peer review Not commissioned; externally peer reviewed.