Article Text

Abstract
Introduction Psychogenic non-epileptic seizures (PNES) resemble epileptic seizures, but lack epileptiform brain activity. Instead, the cause is assumed to be psychogenic. An abnormal coping strategy may be exhibited by PNES patients, as indicated by their increased tendency to dissociate. Investigation of resting-state networks may reveal altered routes of information and emotion processing in PNES patients. The authors therefore investigated whether PNES patients differ from healthy controls in their resting-state functional connectivity characteristics and whether these connections are associated with the tendency to dissociate.
Methods 11 PNES patients without psychiatric comorbidity and 12 healthy controls underwent task-related paradigms (picture-encoding and Stroop paradigms) and resting-state functional MRI (rsfMRI). Global cognitive performance was tested using the Raven's Matrices test and participants completed questionnaires for evaluating dissociation. Functional connectivity analysis on rsfMRI was based on seed regions extracted from task-related fMRI activation maps.
Results The patients displayed a significantly lower cognitive performance and significantly higher dissociation scores. No significant differences were found between the picture-encoding and Stroop colour-naming activation maps between controls and patients with PNES. However, functional connectivity maps from the rsfMRI were statistically different. For PNES patients, stronger connectivity values between areas involved in emotion (insula), executive control (inferior frontal gyrus and parietal cortex) and movement (precentral sulcus) were observed, which were significantly associated with dissociation scores.
Conclusion The abnormal, strong functional connectivity in PNES patients provides a neurophysiological correlate for the underlying psychoform and somatoform dissociation mechanism where emotion can influence executive control, resulting in altered motor function (eg, seizure-like episodes).
- Psychogenic non-epileptic seizures
- functional MRI
- functional connectivity
- dissociation
- emotion
- executive control, neuropsychology
- clinical neurology
- EEG
- epilepsy
- electrical stimulation
- neurophysiology
- MRS
- functional imaging
- cognitive neuropsychology
- head injury
- neuropsychiatry
- rehabilitation
- channels
- neuromuscular
- motor neuron disease
- neuropathy
Statistics from Altmetric.com
- Psychogenic non-epileptic seizures
- functional MRI
- functional connectivity
- dissociation
- emotion
- executive control, neuropsychology
- clinical neurology
- EEG
- epilepsy
- electrical stimulation
- neurophysiology
- MRS
- functional imaging
- cognitive neuropsychology
- head injury
- neuropsychiatry
- rehabilitation
- channels
- neuromuscular
- motor neuron disease
- neuropathy
Introduction
Psychogenic non-epileptic seizures (PNES) are paroxysmal episodes that resemble epileptic seizures, but are not based on epileptiform brain activity as recorded by EEGs and have no clinical evidence for epilepsy. Furthermore, no evidence has been found for other somatic causes of the seizures. Instead, psychogenic factors are assumed to cause the seizures.1
PNES is one of the most important differential diagnoses of epilepsy. Although the differential diagnosis has been facilitated by the introduction of video EEG, there are as yet no real positive ictal features suggested to be pathognomonic for PNES. Most patients with PNES are initially misdiagnosed as having epilepsy, which has serious consequences for the patient, such as exposure to unnecessary anticonvulsant medication and considerable delay in starting the appropriate psychological therapy.2 In addition, misdiagnosis of PNES as epilepsy has a substantial economic burden, as erroneous treatments for intractable epilepsy are expensive.3
More knowledge of PNES aetiology is needed to facilitate the process of PNES diagnosis and decide the nature of treatment.4 Existing theories regarding the underlying psychological mechanisms of PNES are diverse and involve multiple factors that may play a role in the development and prolongation of PNES. One factor that is considered particularly important in most theories for PNES5 and other functional symptoms6 7 is dissociation. Dissociation is a broad concept that involves a variety of manifestations. In the literature on somatoform disorders, psychological and somatoform dissociation are often distinguished, but they can be seen as related constructs.8 The process of psychological dissociation is a disruption of the integration of a person's conscious functioning by severing the connection to thoughts, memories, feelings and sense of identity. Somatoform dissociation involves the loss of integration of somatic experiences, functions and responses.9 Dissociation is postulated to be closely related to the process of hypnosis10 and is regarded as a coping strategy in the context of acute or chronic traumatisation when the individual lacks the capacity to integrate adverse experiences.11 PNES patients often demonstrate dissociative symptoms12 and high hypnotisability,13 and dissociative disorders have been reported in over 90% of PNES patients.14 In fact, PNES may be considered as somatoform symptoms resulting from dissociated mental organisation.11 Accordingly, the DSM-IV-TR and ICD-10 classifications of PNES as, respectively, conversion disorder and dissociative disorder are still a matter of debate.15
Since the tendency to dissociate is considered such an important mechanism in the aetiology of PNES, a better understanding of the neurobiological mechanism of dissociation might shed light on the pathophysiology of PNES and lead to more specific treatments. It might explain how information in patients with PNES or other functional symptoms is processed differently compared with non-affected individuals. A previous functional MRI (fMRI) study in patients with a motor conversion disorder identified abnormal functional connectivity (FC) between regions involved in emotion and motor preparation.16 fMRI may identify a similar abnormality in patients with PNES, providing evidence for alternative neuronal routes of information and emotion processing in patients with PNES that probably result in dissociative seizure-like episodes.4 17 18 As yet, no fMRI study has been performed in patients with PNES.
We hypothesise that functional connections between networks involved in emotion, sensorimotor and cognitive processes are abnormal in patients with PNES. Additionally, these abnormal connections are associated with the tendency to dissociate. To test these hypotheses, we performed an fMRI study in patients with PNES and healthy controls.
Materials and methods
Participants
Patients were selected by their clinical psychologist or neurologist (>10 years and >9 years experience, respectively), on the basis of their seizure characteristics,5 tendency to dissociate, and the absence of mental retardation and comorbid psychiatric disorders (eg, mood and anxiety disorders, schizophrenia and psychosis, and substance-related disorders), which were determined through (hetero-)anamnesis and extensive (neuro-)psychological assessment. Individuals with neurological comorbidity (including epilepsy) and malingering patients were excluded. Patients were only included after the PNES diagnosis was confirmed in a tertiary epilepsy centre by an experienced neurologist/epileptologist, using clinical description and, when available, additional (video) EEG investigations.
The total study population included 13 patients with PNES and 13 healthy volunteers. Two patients with PNES did not complete the study and one healthy control demonstrated periventricular heterotopia on MRI, because of which these patients were excluded from the analysis. The other subjects did not have clinically significant MRI abnormalities (table 1). Analyses were performed on the data obtained from 11 patients and 12 healthy volunteers. All participants gave informed consent to participate in the investigation, which received ethical approval by the Medical Ethical Committee of Maastricht University (ref. 10-3-045).
Participant demographics and characteristics
Questionnaires and neuropsychological investigation
All participants were asked to complete questionnaires to evaluate their dissociation tendency. These questionnaires included the Dissociation Questionnaire (DIS-Q), Dissociative Experiences Scale (DES) and the Somatoform Dissociation Questionnaire (SDQ-20).20 Both the psychological forms of dissociation (DES and DIS-Q) and somatoform dissociation (SDQ-20) were assessed. Global cognitive performance was tested using the Raven's Progressive Matrices test.21 We obtained completed questionnaires from 10 patients with PNES and 12 healthy controls, as one patient did not return the questionnaires.
Neuroimaging
MRI was performed on a 3.0-tesla unit equipped with an 8-channel head coil (Philips Achieva, Philips Medical Systems, Best, The Netherlands). For anatomic reference, a T1-weighted 3D turbo field echo was acquired with the following parameters: repetition time (TR) 8.2 ms, echo time (TE) 3.7 ms, flip angle 8°, matrix 240×240, field of view 256×256×180 mm3, 1 mm adjacent reconstructed coronal slices. fMRI data were acquired using a whole-brain single-shot multi-slice blood oxygen level-dependent echo-planar imaging sequence, with TR 2 s, TE 35 ms, flip angle 90°, voxel size 2×2×4 mm3, matrix 128×128, 32 contiguous slices per volume and 195 volumes per acquisition.
For fMRI, four different scans were performed: (1) first resting-state fMRI (rsfMRI) session, (2) picture encoding, (3) Stroop colour naming and (4) second rsfMRI session. During the rsfMRI sessions, subjects were instructed to close their eyes and think of nothing in particular. The rationale for including a second resting-state session after two task-related paradigms was that attentional effort may provoke dissociative phenomena,22–25 which thus may provoke dissociation during the second rsfMRI session.
The picture-encoding task was included in an attempt to stimulate the process of suggestibility by presenting pictures with a high positive sentimental value. During this task, subjects viewed five images of real-life outdoor scenes prior to the fMRI scans during acquisition of the T1-weighted scan.26 Each picture was presented 25 times for 3 s. After approximately half an hour, an fMRI examination was performed while variable-length epochs of new pictures (new condition) were demonstrated mixed among variable-length epochs of the five old pictures (old condition). The epochs were mixed into a run of 195 stimuli. A total of 120 new pictures were shown. With each picture, the subjects had to decide whether it was old or new. The activation during the task was contrasted with the resting-state activation for further analysis. Previous studies with this task showed activation of the bilateral medial temporal lobes and other limbic structures.26
The Stroop task was selected because susceptibility to hypnotic induction (associated with dissociation), has previously been related to Stroop performance and FC changes in the frontal attention system.27 28 In the covert variation of the Stroop test,29 30 a word stimulus is presented in green, blue, yellow or red colour on a black background. Subjects were instructed to think of the colour in which the word was displayed. For example, the word ‘blue’ was written in red letters; the subject had to think ‘red’. Each word was presented for 2 s. In the baseline condition, subjects focused on a cross-hair. The paradigm consisted of seven baseline rest condition blocks (30 s each) alternated with six activation blocks, consisting of 15 words. In total, 24 congruent and 66 incongruent stimuli were presented in a random order. The contrast between the baseline condition and the activation condition was used for further analysis.30
Neuroimaging analysis
Structural MRI scans were reviewed by an experienced neuroradiologist (>10 years experience). fMRI data analysis was performed in MATLAB (Mathworks, Natick, Massachusetts, USA) using the statistical parametric mapping software package (SPM8) (Wellcome Department of Cognitive Neurology, London, UK). Task-related paradigms were analysed using brain activation contrasts according to the general linear model. The blood oxygen level-dependent images were realigned, transformed into the standardised Montreal Neurological Institute space and smoothed with an 8-mm Gaussian kernel. In the general linear model, a standard discrete cosine set was used to correct for (low-frequency) signal drift. Additionally, the paradigms were convolved with the haemodynamic response function. To explore differences in activation between the PNES and control group, a random-effects analysis was performed. Results were thresholded at the p<0.05 level (corrected for family-wise multiple comparisons).
Subsequently, regions of interest with strong activation were defined (of approximately 300 voxels), based on the activation patterns during the tasks averaged for all subjects. This way, we ensured that the created masks were specific for this population, which is preferred over mask definitions available from the literature.31 The masks were created in MRIcro.32
For the resting-state FC analysis, the signal time-course data were filtered by applying a bandpass filter (0.01–0.1 Hz) and corrected for head movement effects by using the six motion correction parameters as a covariate. Seed time courses for each region and subject were then generated by averaging the signal within the region of interest at each time point. Each seed time course was then regressed against all brain voxel time courses to obtain an FC map, which was subsequently transformed using the Fisher-Z transformation.31 Multiple regression was then performed with subject type (patient or control) and rsfMRI session (first or second) as covariates. The resulting contrasts were thresholded at the p<0.05 level (corrected for multiple comparisons using regional FDR33). Regions with significant differences in FC between patients and controls (called FC regions hereafter) were identified, and corresponding masks were created in MRIcro.32 Subsequently, for these regions individual functional connectivity values (called FC values hereafter) were computed by averaging the FC values over all voxels within each mask.
Statistical analysis
Statistical data analyses on summary values were performed in SPSS (PASW Statistics V.18.0, Chicago: SPSS Inc.), whereas analyses on a voxel-by-voxel level were performed in MATLAB (see previous section). Descriptive statistics of relevant variables were obtained, and Mann–Whitney U tests were performed to examine differences between patients with PNES and controls. Additionally, correlation coefficients between dissociation scores, intelligence scores and FC values were obtained over all subjects using the non-parametric Spearman rank-correlation test. Finally, to gain insight into the predictive value of the tested variables for relevant significant correlations from the latter analysis, a linear regression was performed with FC as a dependent variable and dissociation and intelligence scores as independent variables. Statistical significance is denoted as p<0.05.
Results
Clinical and neuropsychological assessments
The study population comprised of 11 patients with PNES (6 women, 5 men, age 34±11 years, number of seizures in previous month 2.0±2.5) and 12 healthy volunteers (8 women, 4 men, age 34±11 years) (table 1). The patients displayed significantly lower performance on the Raven's Progressive Matrices test, and significantly higher dissociation tendency on the dissociation questionnaires, as assessed with Mann–Whitney U tests (p<0.05). The patients displayed high scores for both psychological and somatoform dissociations (p<0.05).
Neuroimaging analysis
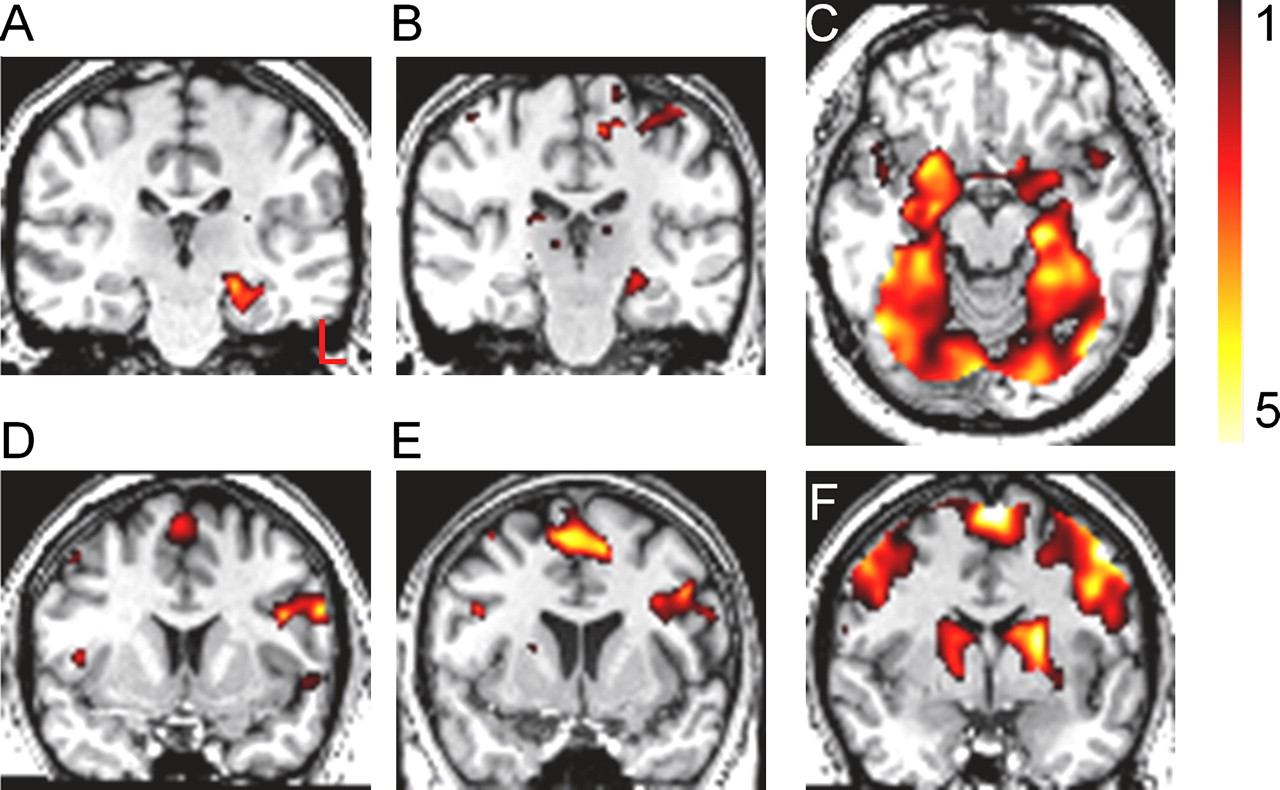
For both the PNES and control groups, the picture-encoding paradigm yielded significant activation within both hippocampi, the left lateral frontal cortex, the parahippocampal gyrus and fusiform gyrus. The Stroop paradigm activated the inferior frontal, precentral and parietal cortices. These results for both groups are typical activation maps, in accordance with the literature.26 30 34 Figure 1 displays the average activation for the picture-encoding and Stroop paradigms for both groups. The random-effects analysis did not reveal any significant differences for picture-encoding and Stroop colour-naming activation maps between controls and patients with PNES.

Group averaged fMRI activation maps superimposed on a normalized T1-weighted MR image. Mean activation patterns for PNES patients are shown in A and D and for healthy controls in B and E. Averaged activation patterns over all subjects are shown in C and F. For the picture encoding paradigm the characteristic hippocampal activation is shown on coronal (A−B), and axial (C) slices. For the Stroop paradigm (D−F) the characteristic prefrontal activation is shown on coronal (D, E, F) slices. The bar on the top right indicates the t-value of the activation level. Slice positions are specified in the MNI coordinate system: y=−24 mm for A and B; z=−18 mm for C, and y=6 mm for D, E, and F.
Based on the average activation for the task-related paradigms, nine seed regions of interest were created (figure 2): left parahippocampal gyrus and right parahippocampal gyrus (based on the encode paradigm), and right inferior frontal gyrus, left inferior frontal gyrus, right intraparietal sulcus, left intraparietal sulcus, left supramarginal gyrus, anterior cingulate cortex and left precentral sulcus (based on Stroop paradigm). The FC maps based on the seed regions left inferior frontal gyrus, left intraparietal sulcus, left supramarginal gyrus and left precental sulcus yielded significant group differences in connectivity values (p<0.05, corrected) (table 3, figure 3). The right intraparietal sulcus yielded similar results as the left intraparietal sulcus (data not shown). The other four seed regions did not yield significant differences in FC values. Multiple regression did not yield statistical significant differences between the two rsfMRI sessions (p>0.12).

Seed regions obtained from the activation maps from the picture-encoding (8, 9) and Stroop paradigms (1–7), superimposed on a normalised T1-weighted MR image. 1, right inferior frontal gyrus; 2, left inferior frontal gyrus; 3, right intraparietal sulcus; 4, left intraparietal sulcus; 5, left supramarginal gyrus; 6, anterior cingulate cortex; 7, left precental sulcus; 8, right parahippocampus; 9, left parahippocampus. MNI coordinate system: z=+46 mm for A, y=+6 mm for B and y=−42 mm for C. MNI, Montreal Neurological Institute.

Regions of significant higher functional correlation for seed regions left precentral sulcus (A–C) and left inferior frontal gyrus (D) for PNES patients compared with controls during resting-state fMRI, overlaid on an average normalised T1-weighted MR image generated using MRIcro (A, B, D) or projected on an inflated right hemisphere surface map generated in Freesurfer (MGH, Massachusetts, USA) (C). Contrast is visible in the central sulcus (CS), anterior insular cortex (ICa), posterior insular cortex (ICp), anterior cingulate cortex (ACC), posterior cingulate cortex (PCC) and parietal occipital fissure (POF). The bar on the top right indicates the t-value of the FC map. MNI coordinate system: x=−44 mm for A, y=+8 mm for B and y=50 mm for D. FC, functional connectivity value; MNI, Montreal Neurological Institute; PNES, psychogenic non-epileptic seizures.
Compared with healthy controls, patients had several significantly stronger functional correlations in the following FC regions: the anterior insular cortex, posterior insular cortex, central sulcus, posterior cingulate cortex, anterior cingulate cortex and parietal occipital fissure (table 2). Interestingly, most FC regions were significantly different in FC maps from more than one seed region (table 3). For example, the posterior insular cortex showed significantly higher correlation values with the precentral sulcus, the supramarginal gyrus as well as the intraparietal sulcus in PNES patients than in controls (average Fisher-Z transformed connectivity values: 0.37±0.12 vs 0.25±0.10, 0.31±0.15 vs 0.15±0.13 and 0.30±0.15 vs 0.17±0.13, respectively).
Maximal Z-score and (cluster size) of regions with significant (positive) differences in FC between PNES patients and controls
Spearman's correlation coefficients (over all subjects) between FC values and scores on DIS-Qs and Raven's test
Correlation analysis
As the two rsfMRI sessions did not differ, FC values were averaged over the two sessions. Significant correlations (p<0.05) were found between the abnormal FC values and DES, DIS-Q, SDQ and Raven scores (table 3). We would like to highlight two correlations that were identified as related to dissociation, especially relevant from the perspective of PNES: precentral sulcus-anterior insula and precentral sulcus-posterior insula. For example, the FC value of the precentral sulcus-posterior insula correlated significantly with the DES (Spearman's ρ=0.56, p=0.007; figure 4). The FC value of the precentral sulcus-posterior insula connection also negatively correlated significantly with the Raven performance (Spearman's ρ=−0.56, p=0.005). A linear regression for this FC value as a dependent variable and DES and Raven test scores as independent variables yielded DES score as a significant predictor (β=0.066, p=0.046). Raven test score was not a significant predictor (p=0.37).
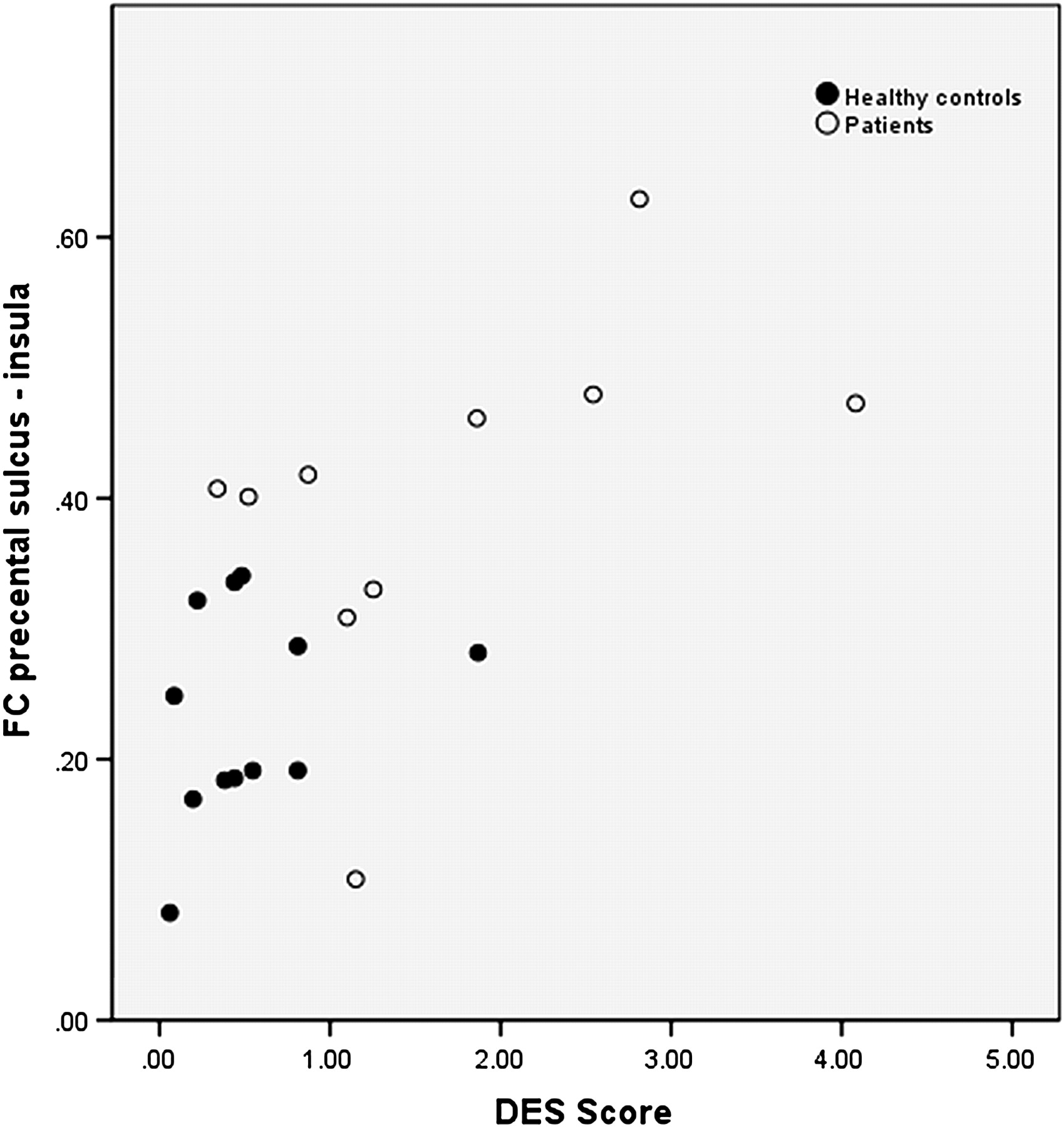
Scatter plot of distribution of the left precentral sulcus—right posterior insular FC values and DES scores in the whole population. Healthy controls are depicted by black dots, PNES patients are depicted by white dots (Spearman's ρ=0.56, p=0.007). DES, Dissociative Experiences Scale; FC, functional connectivity value; PNES, psychogenic non-epileptic seizures.
Discussion
In this study, we investigated resting-state networks in PNES patients and healthy controls to potentially reveal PNES-associated neurophysiology in terms of altered routes of information and emotion processing. First, a significantly higher dissociation tendency was observed in patients with PNES. Furthermore, an abnormal functional correlation was observed between the precentral sulcus, which resides in the motor cortex controlling voluntary muscle movement, and the insula, which is part of the limbic system and involved with emotion regulation, visceral sensory perception and self-awareness.35 Additionally, significantly stronger correlations were found between the parietal lobe, which is involved in processing of sensory information and subsequent action organisation,36 and the insula. Moreover, a positive relationship between FC values and dissociation scores was found.
Dissociation and PNES
Our results reconfirm that patients with PNES have in general a higher tendency for dissociation than healthy individuals. This is a general effect concerning both psychological and somatoform dissociation.14 28 37
Dissociation and fMRI
The functional connections of the ACC are of interest as the ACC is an area that has been identified to be involved in dissociation and hypnosis.38 The FC value of the IFG with ACC was significantly higher in the PNES group. Furthermore, the strength of this connection was significantly related to DES scores. This might have clinical relevance in PNES, as this connection has been associated with cognitive integration and dissociation.27
Outside the domain of PNES, previous studies have related dissociation with fMRI outcomes. For example, Veltman et al39 have demonstrated increased activation of the dorsolateral and ventrolateral prefrontal cortices, parietal cortex and supplementary motor area during working memory tasks in healthy, high-dissociative participants. Similarly, Elzinga et al40 reported increased activation in anterior, dorsolateral and ventrolateral prefrontal cortices and parietal cortex during a working memory task in patients with dissociative disorder. These results suggest that dissociation is associated with an altered working-memory network.
In contrast, the results of the current study do not reveal differences in activation maps of the encoding task (working memory) or in FC based on seeds relevant to memory (hippocampi), between healthy controls and highly dissociative PNES patients. Also, although the picture-encoding task employed emotional stimuli, the activation was related to processes of working memory instead of suggestibility. However, we did find abnormalities in FC in highly dissociative patients with PNES based on seed regions obtained by the Stroop task. Previous studies in patients with PNES did indicate only a modest working memory deficiency.41 We propose that the PNES pathology affects the neurobiology of executive control, which underlies dissociation, rather than the networks involved in memory processes.
Dissociation and cognition in PNES
Subjects with lower performance on the Raven's test scored significantly higher on the dissociation scales, which is in accordance with previous literature.42 Dissociation might exert a perturbing action on individuals, which can negatively influence cognitive performance.
The FC values also correlated significantly with global cognitive functioning scores, as assessed using the Ravens' test. Previously, we showed in patients with chronic epilepsy that FC values, as assessed with fMRI, were strongly correlated with intelligence (ie, performance on word fluency and text-reading tests). We hypothesised that a reduced performance was related to a reduced synchronisation of activity in the brain.43 In the current study, we observed the opposite effect, namely, a negative correlation of FC values with global cognitive performance. However, a linear regression analysis showed that global cognitive performance (ie, intelligence) was not a significant predictor for FC values, whereas dissociation was. This emphasises that dissociation, and not intelligence, is a key mechanism underlying abnormal FC values as observed in patients with PNES (figure 4).
Conversion disorders and fMRI
It has been suggested that PNES share a pathophysiological mechanism with other conversion disorders.4 18 An fMRI study in patients with motor conversion revealed that patients have a higher FC between the amygdala and the supplementary motor area during processing of positive and negative emotional stimuli.16 It was suggested that this abnormal FC hints at a greater influence of limbic regions over motor preparatory regions.18 Similarly, in dissociative amnesia, the relationship between memory-related areas and executive control areas may be affected,18 44 which also hints at a ‘faulty’ connection between executive control and areas specifically affected by dissociation.
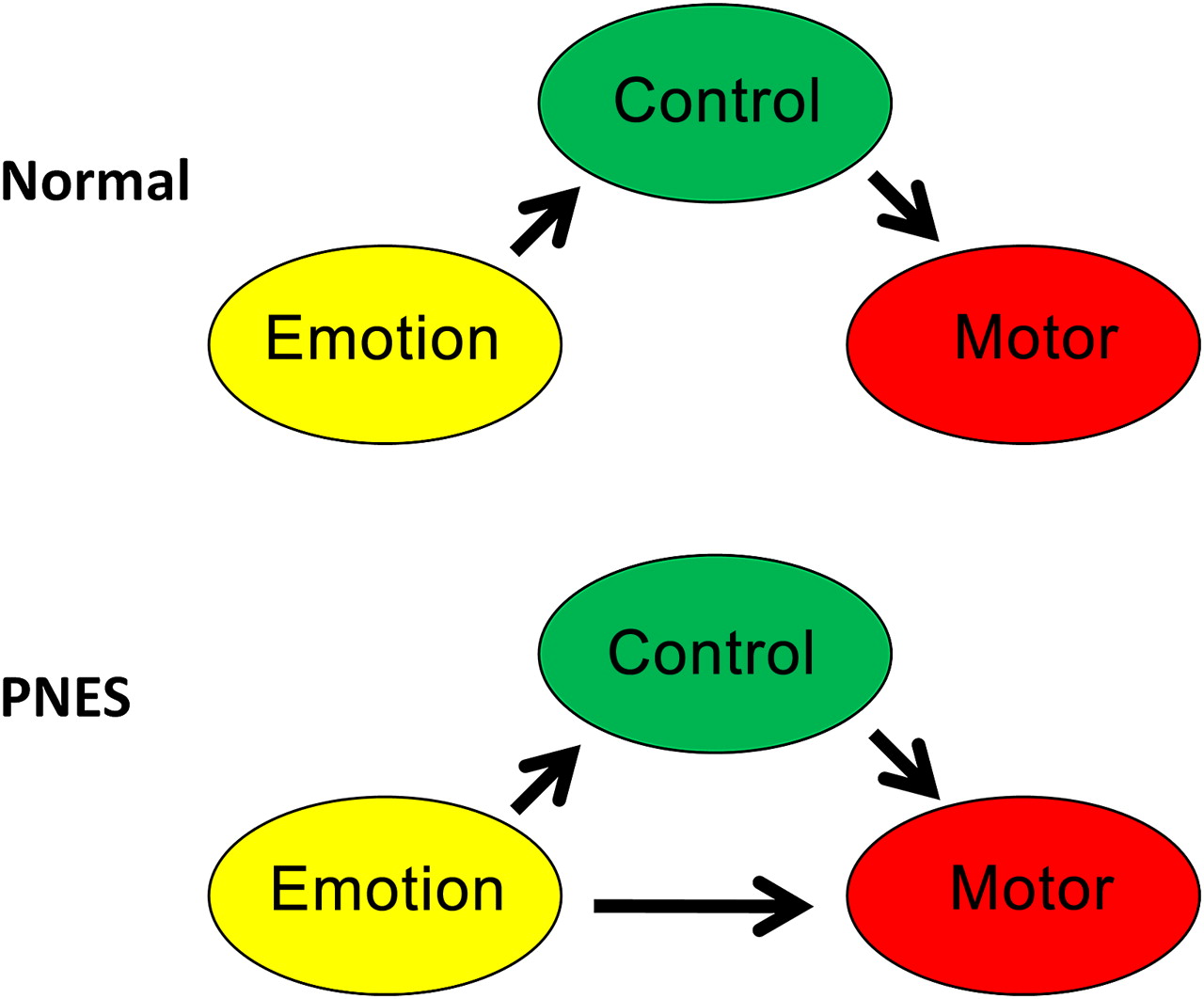
As we found in PNES, higher FC values between regions involved in emotion and self-perception (insula) and motor preparation (precentral and the sulcus) between these two regions might underlie the pathophysiology for conversion disorders in general, including PNES.4 The existence of such an unstable cognitive–emotional–motor ‘hyperlink’ is further supported by the fact that PNES is often accompanied by many diffuse psychological, psychiatric and somatoform symptoms.18 45 In addition to the connection pair ‘insula-precentral sulcus’, we also identified other combinations of seed regions and FC regions (originating in the frontal, parietal and limbic cortices) with higher FC values for patients. The presence of higher FC in these regions strengthens the assumption that the whole network involved in sensory processing, executive control and emotion regulation in patients with PNES is abnormal. Figure 5 displays a schematic representation of the underlying dysfunctioning in this network in patients with PNES.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic overview of the circuitry involved in cognitive–emotional executive control. In this study, we found significantly higher functional connectivity strengths between regions involved in emotion (insula) and motor planning (precentral sulcus) for patients with PNES. It appears that healthy controls can control their motor functions without strong influence of emotions, whereas in patients with PNES emotions can bypass executive control and cause involuntary movement. PNES, psychogenic non-epileptic seizures.
Clinical implications
Demonstration of a relationship between dissociation and deficient neuronal processing in PNES has substantial implications for the understanding of the aetiology. Dissociation is one of the mechanisms through which an emotional state can influence executive control, resulting in a seizure-like episode17 18 (figure 5). Furthermore, the high FC identified in the current study has potential for the use of functional imaging to aid the differential diagnosis between PNES and epilepsy.
More knowledge of PNES aetiology is necessary for the clinical management of PNES diagnosis and treatment.4 As such, a higher tendency to dissociate, associated with the hyperlink between regions involved in emotion (insula) and motor preparation (precentral sulcus), may be seen as an increased vulnerability to develop PNES. Moreover, identifying a neurobiological substrate of dissociation in PNES changes the concept of psychogenic seizures into a biopsychological phenomenon, where a psychogenic aetiology collides with a specific neurological vulnerability. This has implications for the development and evaluation of treatment, and may eventually improve the clinical management of PNES diagnosis. Moreover, it might aid the patient in accepting diagnosis of PNES. However, it is difficult to consider network abnormalities purely as a predisposition factor, as a diseased network connectivity could either be the cause or the consequence of dissociation and PNES.
Study limitations and future considerations
This study had a limited number of patients. However, even in this small population, statistically significant deviations were demonstrated. These findings should be validated in larger studies, to be able to identify the direction of causality between abnormalities in FC and dissociation and PNES.
Another limitation is that the effect of PNES cannot be disentangled from the effect of dissociation. All of our patients had both PNES and a high dissociation score. To resolve this problem, future studies should include a control group of PNES patients who are not highly dissociative and/or a control group of healthy normal subjects with a high dissociation.
Furthermore, it is not known whether FC abnormalities are accompanied by microstructural (white matter) abnormalities.
Conclusion
The abnormal strong FC found in patients with PNES hints at an underlying psychoform and somatoform dissociation mechanism where emotion can influence executive control, resulting in altered motor function (eg, seizure-like episodes). Future studies should clarify the exact contribution and interaction of the process of dissociation and network disturbances in PNES.
Acknowledgments
The authors thank Remco Berting for assistance with image acquisition.
References
Footnotes
Funding JFAJ was funded by VENI research grant 916.11.059 from The Netherlands Organization for Scientific Research (NWO) and The Netherlands Organization for Health Research and Development (ZonMw). APA is supported by the National Epilepsy Foundation (NEF), Zeist, the Netherlands.
Competing interests None.
Patient consent Obtained.
Ethics approval Medical Ethical Committee of Maastricht University (ref. 10-3-045).
Provenance and peer review Not commissioned; externally peer reviewed.