Article Text

Abstract
Background The phosphorylated neurofilament heavy subunit (pNF-H), a major structural component of motor axons, is a promising putative biomarker in amyotrophic lateral sclerosis (ALS) but has been studied mainly in CSF. We examined pNF-H concentrations in plasma, serum and CSF as a potential biomarker for disease progression and survival in ALS.
Methodology We measured pNF-H concentration by monoclonal sandwich ELISA in plasma (n=43), serum and CSF (n=20) in ALS patients collected at the Mayo Clinic Florida and Emory University. We included plasma from an ALS cohort (n=20) from an earlier pilot study in order to evaluate baseline pNF-H levels in relation to disease progression using the Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R), survival and anatomical region of ALS onset.
Results Higher pNF-H levels in plasma, serum and CSF showed evidence of association with faster decline in ALSFRS-R. There was evidence for a relationship of higher serum and plasma pNF-H levels with shorter survival, although evidence was weaker for CSF. pNF-H concentration in plasma (n=62) may be higher in patients with bulbar onset than in patients with spinal onset.
Conclusions In ALS, increased pNF-H concentration in plasma, serum and CSF appears to be associated with faster disease progression. Factors affecting pNF-H levels or their detection in serum and plasma in relation to disease course may differ from those in CSF. Data raising the possibility that site of ALS onset (bulbar vs spinal) may influence pNF-H levels in peripheral blood seems noteworthy but requires confirmation. These data support further study of pNF-H in CSF, serum and plasma as a potential ALS biomarker.
- Als
- Csf
- Motor Neuron Disease
Statistics from Altmetric.com
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disorder of unknown cause, and is fatal in the majority of patients within 3 years owing to respiratory muscle weakness.1 ,2 The diagnosis of ALS is readily established on clinical grounds, but rate of disease progression and survival may vary significantly among patients. Prognosis can be estimated based on clinical features but these have limited sensitivity and may require extended follow-up, and there is a strong need for disease biomarkers in ALS that demonstrate greater sensitivity to disease progression and survival than those presently available.3 ,4 Putative molecular indicators of disease pathology in ALS measured in CSF or peripheral blood have been a focus of recent studies, but no biomarkers of this kind have been fully validated for use in clinical practice or clinical trials.5 ,6
Neurofilaments are major structural components of motor axons, and their subunit proteins have been investigated as potential biomarkers of motor axon breakdown in ALS.7–11 Several groups have shown that reactivity for the phosphorylated heavy subunit of neurofilament (pNF-H) and neurofilament light subunit (NF-L) measured by ELISA is increased in CSF in ALS compared with healthy and neurological disease controls, supporting the concept that elevated pNF-H and NF-L concentrations may be useful biomarkers in ALS.8–11
pNF-H and NF-L levels in CSF have been reported to correlate with rate of disease progression and survival in ALS.8–11 Given difficulties inherent in obtaining CSF as opposed to peripheral blood, in this study we evaluated pNF-H levels in plasma and serum in comparison with CSF in ALS patients using a new monoclonal antibody based sandwich ELISA.7 In our initial pilot study using this assay, pNF-H levels in plasma measured monthly for 4 months were significantly increased in ALS patients compared with similarly aged healthy control individuals, and were relatively stable longitudinally.7
Here we present data demonstrating an association between pNF-H concentration in plasma, serum and CSF and rate of disease progression in patients followed longitudinally at Mayo Clinic, expanding the analysis of plasma pNF-H by inclusion of data from our previously reported pilot study.7 We also present data demonstrating an association between pNF-H concentration in plasma and survival in two independently collected ALS cohorts at Mayo Clinic Florida and Emory University, and comparison data from a similar analysis of pNF-H levels in serum and CSF in a subgroup of these patients. Findings with regard to associations between site of onset of weakness in ALS and pNF-H levels in plasma, serum and CSF also are reported.
Methods
Patients
This study received ethics committee approval at Mayo Clinic, Emory University and University of Florida; all subjects provided written informed consent. ALS patients had El Escorial clinically definite, probable, laboratory supported probable or possible ALS of <5 years’ duration. Patients receiving tracheostomy ventilation or non-invasive mechanical ventilation for >23 h/day were excluded. Exclusion criteria included history of medical conditions that could potentially increase blood levels of pNF-H (ie, stroke within 30 days of enrolment, peripheral neuropathy). This study included two cohorts: 20 patients followed longitudinally for 12 months at Mayo Clinic from whom plasma, serum and CSF were collected at baseline, and 23 patients at Emory University who provided baseline plasma samples but were not followed longitudinally for the purposes of the study. Survival data were collected for both cohorts. In patients who completed a lumbar puncture, exclusions included a history of conditions which could potentially alter the blood–CSF barrier (ie, spinal surgery). Longitudinal disease progression was evaluated using the Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R), recorded at baseline and monthly to month 6, and then at month 9 and month 12. The ALSFRS-R is a validated functional outcome measure for ALS clinical trials.4 ,12 ,13 We included in our analysis baseline plasma pNF-H concentrations from a previously reported pilot cohort of patients with ALS evaluated at the Mayo Clinic Florida who were followed longitudinally for 4 months (Mayo 4 month follow-up cohort), updated with survival data collected since our initial publication.7
ELISA analysis
Plasma and serum were processed within 1 h of blood collection. CSF was obtained by lumbar puncture 2–3 h following blood sample collection and processed within 30 min. CSF was centrifuged to remove cells. Samples were stored at −80°C prior to analysis of pNF-H. pNF-H ELISAs were conducted in the laboratory of one of the authors (GS), as described previously, blinded to disease status.7 The pNF-H ELISA used in this study, including the monoclonal capture and detection, and bodies, was developed in the laboratory of GS. Intra-assay coefficient of variance (CV) for eight serially diluted pNF-H standards was 0.057. Inter-assay CV for each of the standards run 16 times on each of 7 days ranged from 0.085 to 0.125. All assays were performed with a single batch of reagents with subsets of samples run on different dates.
Statistical analysis
Numerical variables were summarised by the sample median and IQR. pNF-H was compared between patients with bulbar onset ALS and those with spinal onset ALS using a Van Elteren test stratified by cohort; a Mann–Whitney test was performed separately for each cohort (Mayo 12 month, Emory and Mayo 4 month). The association of pNF-H with the monthly rate of change in ALSFRS-R was estimated by Spearman's rank correlation coefficient (r). Single variable Cox proportional hazards regression models were used to examine the association of pNF-H with time to death, tracheostomy or use of non-invasive ventilation for >23 h per day from the time of sample collection; estimates of HRs and 95% CI are presented. Censoring occurred on the date of the last follow-up in patients who did not experience tracheostomy, non-invasive ventilation for >23 h per day or death. One patient whose unanticipated death was unrelated to ALS was censored at the date of death. A p value <0.05 was considered statistically significant. All analyses were performed using SAS (V.9.2; SAS Institute Inc, Cary, North Carolina, USA) and R Statistical Software (V.2.14.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
In the Mayo Clinic cohort from whom plasma, serum and CSF were collected (Mayo 12 month follow-up cohort; n=20), median disease duration from onset to blood and CSF collection was 18 months (range 11–56), median age was 58 years and 80% of patients were male. Site of onset of weakness was bulbar in nine and spinal in 11. Patient characteristics in the Mayo 12 month follow-up cohort were similar to those of the Emory cohort (n=23) and the Mayo Clinic 4 month follow-up cohort (n=19) (table 1). All patients were white except for a black American man in the 12 month follow-up cohort. All patients had sporadic ALS except for two patients in the 12 month follow-up cohort; one patient had a C9ORF72 repeat expansion and one had a TARDBP mutation.14–16 Of all the studied patients, 46 (74%) took riluzole; none had received experimental medications for the treatment of ALS within 30 days of enrolment.
Patient characteristics for the three cohorts included in the study
Baseline pNF-H concentrations
In the Mayo 12 month follow-up cohort, median pNF-H level was 4.38 ng/ml in CSF, 0.66 ng/ml in serum and 0.91 ng/ml in plasma (table 1). Plasma and serum pNF-H levels were highly correlated (r=0.97), and also correlated, but to a lesser degree, in CSF and plasma (r=0.47) and in CSF and serum (r=0.51; figure 1). In individual patients, CSF pNF-H levels were higher than serum pNF-H levels in all 20 patients (median ratio CSF:serum 5.45; range 1.18–40.95) and exceeded plasma pNF-H levels in 19/20 patients; in one patient, the pNF-H level in CSF was minimally lower than in plasma (median ratio CSF:plasma 5.71; range 0.98–62.58).

Cross comparison scatterplots of baseline phosphorylated neurofilament heavy subunit (pNF-H) concentrations in CSF, serum and plasma in 20 patients in the Mayo 12 month follow-up cohort, depicting correlations between pNF-H levels in each patient for the respective biofluid types. (A) CSF versus serum; (B) CSF versus plasma; and (C) serum versus plasma. (D) Bland–Altman plot of the data presented in (C) is shown to allow a visual assessment of the level of agreement between serum and plasma pNF-H concentrations obtained with our assay. There is a strong correlation between pNF-H concentrations measured in serum and plasma in this cohort.
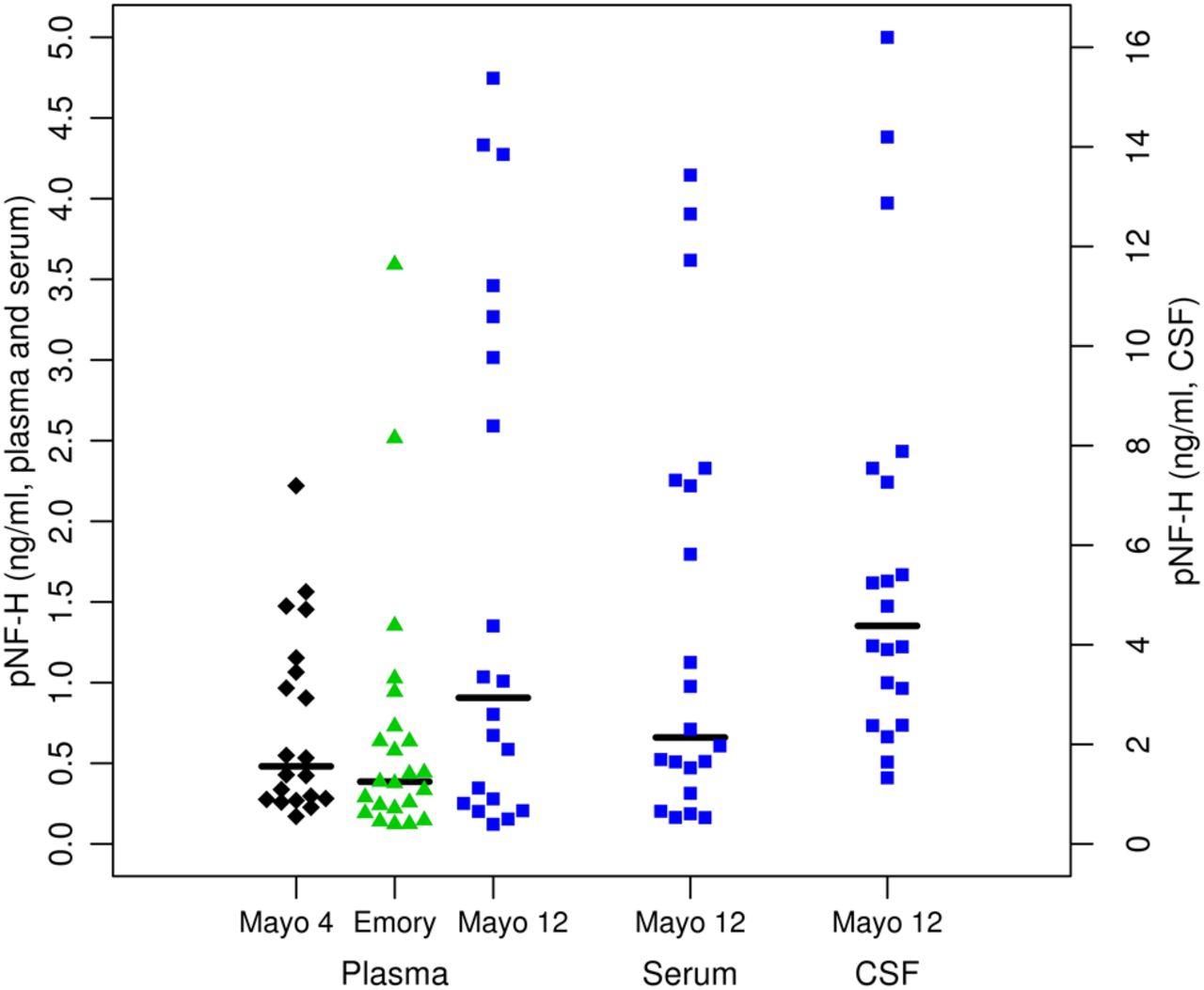
A median plasma pNF-H level of 0.91 ng/ml in the Mayo 12 month follow-up cohort was higher than the median of 0.39 ng/ml in the Emory cohort and 0.48 ng/ml found in the previously studied Mayo 4 month follow-up cohort, but there was no statistically significant difference in pNF-H levels across cohorts (p=0.16) (table 1, figure 2). No evidence of association was observed between pNF-H concentrations and gender or disease duration for any of the biofluid types studied across the three cohorts (data not shown).
{kind=link}
{kind=link}
Distributions of phosphorylated neurofilament heavy subunit (pNF-H) concentrations in plasma, serum and CSF. Squares represent patients in the Mayo Clinic 12 month follow-up cohort (Mayo 12; plasma, serum and CSF), triangles represent patients in the Emory University cohort (plasma only) and diamonds represent patients in the Mayo Clinic 4 month follow-up cohort (Mayo 4; plasma only). Black horizontal lines represent the median pNF-H for the given cohort. Note that the left vertical axis scale reflects pNF-H levels in plasma and serum and the right vertical axis scale represents pNF-H levels in CSF.
pNF-H concentration and disease progression
We examined the association between baseline pNF-H levels in the Mayo 12 month follow-up cohort and slope of the ALSFRS-R in the 4 months (median ALSFRS-R slope −1.0 points per month) and 12 months (median ALSFRS-R slope −0.9 points per month) from baseline. The association between higher CSF pNF-H level and faster rate of decline in the ALSFRS-R was significant after 4 months of follow-up (r=−0.59, p=0.006) and at 12 months (r=−0.54, p=0.015) (table 2). The association between higher serum pNF-H levels (n=20) and more rapid decline in the ALSFRS-R was significant after 4 months of follow-up (r=−0.46, p=0.042) but not after 12 months of follow-up (r=−0.31, p=0.19). Higher plasma pNF-H levels (n=20) showed weak evidence of association with faster decline in the ALSFRS-R at 4 months (r=−0.38, p=0.095) but less so over 12 months (r=−0.25, p=0.29). To increase numbers, we repeated the 4 month analysis, including data from the previously reported patients (Mayo 4 month follow-up cohort) in whom 4 month ALSFRS-R data were collected monthly for 4 months, similarly to the 12 month follow-up cohort.7 In this analysis (n=38; median ALSFRS-R slope −0.9 points per month) the association between higher plasma pNF-H level and more rapid decline in the ALSFRS-R was statistically significant (r=−0.35, p=0.030) (table 2). The Emory cohort was not included in this analysis because serial ALSFRS-R data were not available for these patients.
Association between pNF-H and ALSFRS-R rate of change per month
pNF-H concentration and survival
Examination of plasma or serum pNF-H levels in relation to survival from date of sample collection suggested an association between increased pNF-H concentration and the survival endpoint in the Mayo 12 month follow-up cohort (table 3); a doubling in pNF-H in plasma was associated with nearly a twofold increase in the risk of a death endpoint (HR 1.87, 95% CI 1.19 to 3.35, p=0.006), and a doubling of pNF-H in serum was associated with a greater than twofold estimated increase in the risk of death endpoint (HR 2.10, 95% CI 1.28 to 3.91, p=0.002). A similar relationship was found for plasma pNF-H in the Emory cohort alone and in the three cohorts combined, but not in the Mayo 4 month follow-up cohort alone (table 3). CSF pNF-H levels in the Mayo 12 month follow-up cohort in this analysis showed only weak evidence of association with shorter survival from the date of sample collection that was not statistically significant, although the estimated HR was of a similar magnitude to that seen for serum and plasma (table 3). We also examined the association of risk of death with increased pNF-H concentration in CSF, serum or plasma in relation to survival from clinical onset of ALS. HRs associated with higher pNF-H levels in CSF, serum or plasma in this analysis suggested a weaker association with survival from onset of weakness than in the analysis of survival from the time of sample collection and, aside from serum pNF-H, did not reach statistical significance (table 3).
Association of pNF-H level with survival from time of sample and from time of ALS onset
pNF-H and site of ALS onset and patient age
Median pNF-H in plasma or serum in each of the three cohorts was 2–3-fold higher in patients with bulbar onset compared with patients with spinal onset (see online supplementary table S1). This difference was not statistically significant in any of the cohorts analysed individually, although the difference for plasma pNF-H in the combined cohorts (n=62), with a median of 0.85 ng/ml in patients with bulbar onset (n=24) versus 0.34 ng/ml in those with spinal onset, approached significance (p=0.055; see online supplementary table S1). In CSF (n=20), pNF-H levels were of comparable magnitude in bulbar versus spinal onset and were not significantly different (see online supplementary table S1). The distribution of pNF-H levels in bulbar and spinal onset ALS patients revealed in all cohorts a similar pattern in each biofluid type, with levels in spinal onset patients skewed towards lower pNF-H levels than those with bulbar onset (see online supplementary figure).
pNF-H levels tended to be higher with both age at ALS onset and age at time of sample collection, although these associations were not statistically significant (see online supplementary table S2). To investigate possible confounding, we re-examined the association of pNF-H in plasma with survival from the time of sample collection in the three cohorts combined, with adjustment for site of onset and age at the time of sample; the results were similar to those reported without adjustment (HR 1.32, 95% CI 1.04 to 1.66, p=0.020) (table 3).
Discussion
We found an association in our patients between higher concentration of pNF-H in plasma, serum and CSF and more rapid rate of decline in the ALSFRS-R, supporting the concept that pNF-H levels in peripheral blood or CSF may represent an indicator of disease activity and prognosis in ALS. These findings are in line with data from others suggesting that increased levels of pNF-H in CSF are associated with more rapid disease progression in ALS measured by the Medical Research Council score.8 To our knowledge, this is the first report examining pNF-H in peripheral blood in relation to a validated ALS functional outcome measure, and suggests that pNF-H levels in plasma or serum hold promise as a biomarker associated with future clinical course in ALS.
That a statistically significant association between CSF pNF-H and rate of decline in the ALSFRS-R was seen with follow-up to 12 months, while the association for serum or plasma pNF-H levels was not significant beyond 4 months, and that for plasma pNF-H a larger sample size was needed to achieve significance, suggests that CSF pNF-H may be more closely associated with future clinical course than serum or plasma pNF-H in the follow-up intervals studied.
pNF-H levels present in plasma, serum and CSF in ALS patients are likely a complex function of several variables. These include the quantity and rate of pNF-H released from CNS and peripheral nerve tissue, the dynamics of pNF-H conveyance from source tissues, metabolism of pNF-H in the respective compartments, transport of pNF-H into peripheral blood from the CNS and relative volumes of CSF and peripheral blood. Disease specific and homeostatic factors presumably contributed to differences in the association between pNF-H levels in CSF and peripheral blood and disease outcome measures, but unrecognised effects on the detection of pNF-H by our ELISA that are specific to serum/plasma and/or CSF also are possible. The pNF-H level in most patients was slightly higher in co-collected plasma than in serum, suggesting possible sequestration of a component of the pNF-H signal into clotted material. However, we found an excellent correlation between pNF-H values determined from each sample type (figure 1), so that our assay is expected to produce workable data with both plasma and serum. It remains to be seen if this is a general feature of pNF-H determination not limited to studies of ALS, or is specific to particular types of CNS disease and damage states.
Median pNF-H levels in plasma and serum tended to be higher in our patients with bulbar onset of ALS compared with spinal onset, a pattern not evident in CSF; the differences were not statistically significant in any of the individual cohorts but approached significance for plasma pNF-H in the three cohorts combined, the analysis with the largest number of patients (see online supplementary table S1, figure). Although uncertain, the data raise the possibility that the anatomical level of clinical onset of ALS, bulbar versus spinal, may influence pNF-H levels, particularly in peripheral blood, and leave open the possibility that any association between higher pNF-H levels in peripheral blood and bulbar onset may reflect the effects of bulbar disease on the physiology of pNF-H transfer from the CNS to the periphery. Our observations regarding pNF-H levels in CSF with regard to site of ALS onset are in line with a previous report by others on pNF-H in ALS CSF in which no relationship between CSF levels and site of ALS onset was observed.8 However, sample size is relatively small in both studies and further investigation seems warranted in order to determine whether the site of ALS onset influences the concentration of pNF-H, and whether any such effect may differ between CSF and peripheral blood.
Given the reported association between older age at disease onset and shorter survival in ALS, we looked for an association between pNF-H levels and age at ALS onset and age at time of sample collection but found no significant associations (see online supplementary table S2).3 The level of pNF-H in CSF was reported in one study to be increased with age in ALS, but in multiple other studies of neurological disorders, including ALS, no such association was found.8 ,17–19 Any potential association between pNF-H level and age does not appear to have been a confounding factor in our data, which suggests that in ALS, pNF-H levels in peripheral blood and CSF are more strongly associated with clinical course than with the age of the patient, although age warrants attention as a potential covariate in future studies of pNF-H in ALS.
Although examination of the potential association between pNF-H levels and time from onset of weakness to ALS diagnosis was of interest in view of the reported association between shorter time to diagnosis and shorter survival, we did not have adequate information in all cases as to when the patient's condition met the diagnostic criteria for ALS.3 As a consequence, we were unable to conduct a reliable analysis of this in our patients.
The observation that higher pNF-H levels conferred increased risk of shorter survival from the time of sample collection in serum and plasma in the Mayo 12 month follow-up cohort, and in plasma in the Emory cohort and the three cohorts combined, seems internally consistent with the association between higher pNF-H levels and more rapid decline in the ALSFRS-R in these cohorts, as is the lack of such associations for plasma pNF-H in the Mayo 4 month follow-up cohort (tables 2 and 3). Notable is the lack of statistically significant association between survival from the point of sample collection for CSF pNF-H in the Mayo 12 month follow-up cohort in view of the strong association seen between CSF pNF-H and rate of decline in the ALSFRS-R. The small sample size and resulting high variability may account for this, but the data also leave open the possibility that factors governing day to day pNF-H concentration in CSF, and potentially its detection by our assay, may differ from those in serum or plasma. Further study of pNF-H in larger numbers of patients, particularly examination of serially collected longitudinal samples of plasma, serum and CSF obtained in parallel, would help to address this question, as would further refinement of our pNF-H assay.
The median plasma level of pNF-H in the Mayo 12 month cohort was approximately twofold higher than in the Emory or Mayo 4 month cohorts but the differences were not statistically significant. Technical factors involving the assay or sample processing seem unlikely to be a significant factor in this, given similar specimen processing at the participating centres, and based on our extensive experience with the pNF-H ELISA. We suspect that differences in clinical characteristics among patients in the respective cohorts may contribute, but relatively small sample size limits detailed analysis.
The concept that pNF-H in plasma, serum or CSF measured at a given time point may allow estimation of prognosis over a limited time interval is supported by our observation of a greater hazard risk for higher plasma or serum pNF-H in relation to survival from time of sample collection compared with survival from ALS onset (table 3), given that median survival from time of sample collection was 25 months while median survival from time of ALS onset was 43 months, although limited precision in estimation of the date of ALS onset and small sample size may also be important factors. Two previous reports noted an association between neurofilament subunit levels in CSF and survival in ALS, measured from the time of ALS onset, one focusing on neurofilament NF-L protein and the other on pNF-H.9 ,11 Comparison of our results with those reports is limited in that we employed a Cox proportional hazards model in our survival analysis that considered deceased and surviving subjects, while the earlier reports used statistical methods that apparently did not censor for surviving patients. Further studies of pNF-H levels in peripheral blood and CSF and survival should help to resolve these discrepancies.
While the number of patients included in this study is relatively small, these data support continued study of pNF-H in plasma and serum, as well as CSF as a potential biomarker of disease activity and progression in ALS. Our data further raise the possibility that site of ALS onset and bulbar dysfunction at the time of sample collection warrant further investigation as potential covariates in these studies.
Acknowledgments
We thank the patients and caregivers who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
Footnotes
-
Contributors KBB drafted and revised the manuscript, contributed to the concept and design of the study, supervised the study, acquired, analysed and interpreted the data, obtained funding and is the guarantor. JDG and GS revised the manuscript for content, contributed to the concept and design of the study, supervised the study, acquired and analysed or interpreted the data, and obtained funding. GS contributed essential reagents. JEC revised the manuscript for content, analysed or interpreted the data, and conducted the statistical analysis. CY acquired and analysed the pNF-H assay data. CST revised the manuscript for content and conducted the statistical analysis. PD, AJ, KO, CK and MP coordinated the study and acquired and analysed the data.
-
Funding This work was supported by the ALS Association, grant Nos 1152 and 1478, the Packard Centre for ALS Research, Mayo Clinic Florida ALS Centre Donor Funds and Mayo Foundation.
-
Competing interests KBB receives research support from the ALS Association, Biogen Idec, Cytokinetics Inc, Neuraltus Pharmaceuticals, NIH and Mayo Foundation. JDG receives research support from NIH, Muscular Dystrophy Association, Packard Centre for ALS Research and Neuralstem Inc. GS receives research support from the ALS Association, the American Health Assistance Foundation and the NIH. He is also the owner and founder of EnCor Biotechnology Inc, a company marketing reagents used in this study. He may therefore benefit from increased royalties or equity growth. The pNF-H assay used in this study is available commercially from EnCor Biotechnology Inc (Gainesville, Florida), and is referred to as ELISA-pNF-H-v2.
-
Ethics approval The study received ethics committee approval at Mayo Clinic, Emory University and University of Florida.
-
Provenance and peer review Not commissioned; externally peer reviewed.