Article Text

Abstract
Background Body region of onset and functional disability are key components of disease heterogeneity in amyotrophic lateral sclerosis (ALS).
Objectives To evaluate patterns of grey matter pathology in the motor cortex and correlate focal structural changes with functional disability.
Methods We conducted a single-centre neuroimaging study of a cohort of 33 cognitively normal patients with amyotrophic lateral sclerosis (ALS) and 44 healthy controls. A voxel-wise generalised linear model was used to investigate the distribution of disease burden within the motor cortex in relation to clinical disability.
Results Patients with bulbar onset have bilateral focal atrophy in the bulbar segment of the motor homunculus compared with patients with limb onset who have focal cortical changes in the limb segment of their motor strip. Furthermore, the extent to which different body regions are affected in ALS corresponds to the extent of focal grey matter loss in the primary motor cortex. Cortical ALS pathology also extends beyond the motor cortex affecting frontal, occipital and temporal regions.
Conclusions Focal grey matter atrophy within the motor homunculus corresponds with functional disability in ALS. The findings support the existing concepts of cortical focality and motor phenotype heterogeneity in ALS.
- ALS
- Motor Neuron Disease
- MRI
- Neuroanatomy
- Neuroradiology
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive, clinically heterogeneous neurodegenerative condition. ALS progression is measured using the revised ALS Functional Rating Scale (ALSFRS),1 a 48-point scale subdivided into 12 different domains. The slope of decline of ALSFRS is a prognostic indicator.2 ,3 ALSFRS is a highly reproducible measure of clinical disability4 and is used worldwide as a primary end point of clinical trials.
The functional architecture of the motor cortex in the precentral gyrus was originally described by Wilder Penfield.5 Based on careful clinical evaluation, Ravits and La Spada6 proposed that ALS spreads focally in the nervous system based on the somatotropic anatomy of upper and lower motor neurons. While disease focality is supported by clinical,7 neurophysiological and neuropathological observations, it has not been supported by neuroimaging studies. Most MRI studies in ALS describe motor cortex atrophy, but the distribution of disease burden within the motor strip has not been fully characterised in vivo, and regional motor cortex involvement has not been correlated with clinical disability. Despite successful white matter studies,8 previous imaging studies comparing patients with bulbar and limb onset9 have not identified grey matter differences within the precentral gyrus.
The presence of known mutations, such as the D90A SOD-1 gene mutation, contributes further to motor phenotype heterogeneity in ALS. The imaging signature of this mutation has been elegantly presented in both symptomatic and pre-symptomatic patient cohorts using diffusion tensor imaging,10 magnetic resonance spectroscopy11 and positron emmission tomography imaging.12
In addition to voxel-based morphometry (VBM), cortical thickness measurement is increasingly used to assess regional grey matter pathology in ALS. This technique also detects precentral gyrus cortical thinning in ALS,13 but limited correlation has been established with the overall ALSFRS scores or bulbar subscores.14 However, the degree of cortical thinning in the precentral gyrus was successfully correlated with disease progression rate.15
Reports on the extent of extra-motor cortex involvement in ALS are also inconsistent. Various degree of frontal,16 ,9 temporal,17 parietal,18 cingulate19 and occipital20 atrophy have been described. In an attempt to correct for disease heterogeneity, imaging studies have segregated patients based on psychometric measures, such as verbal fluency deficits,21 frontotemporal lobar dementia,22 semantic memory impairment23 and the consensus criteria for the diagnosis of frontotemporal cognitive and behavioural syndromes in ALS.24 Most of these studies have identified various degrees of frontotemporal atrophy in patients with ALS with no overt detectable cognitive or behavioural impairment, and have suggested a continuum of extra-motor involvement in ALS.25
Objectives
Our study was designed to evaluate patterns of focal grey matter loss in the motor cortex. The primary objective was a volumetric analysis of patients with bulbar and limb onset and interpretation of the regional differences in the context of the functional architecture of the motor strip. The second objective was to identify key regions in the motor cortex where focal atrophy correlates with clinical disability, and examine if the location of these clusters corresponds with the somatotropic anatomy of the precentral gyrus. A third objective was to investigate the patterns and degree of extra-motor cortex involvement in ALS.
Patients and methods
Patient cohort
Population-based incident cases of ALS were recruited between 2009 and 2011 from the Irish National ALS Register, which has been described previously.26 All patients had probable or definite ALS according to the El Escorial criteria.27 Assessment before imaging included a full neurological examination and comprehensive neuropsychological testing. ALSFRS scores and subscores were recorded; handedness, education, age, medication, body region of onset and date of first symptom were also documented. Details of all participating subjects, including healthy controls and patients with bulbar onset and limb onset, are presented in table 1.
Demographic characteristics of the cohorts
Exclusion criteria included cognitive or behavioural impairment, the use of drugs that would affect cognitive performance on neuropsychological testing and a background of cerebrovascular events: haemorrhage or ischaemic stroke. Inclusion criteria included the ability to participate in the imaging study by lying supine in the scanner for up to 40 min. This criterion led to exclusion of patients with severe diaphragmatic weakness. Healthy controls matched for age, gender and education were recruited by local public advertisement. None of the healthy controls were related to the patients with ALS. All participants provided informed consent in accordance with the medical ethics approval of the research project (Ethics (Medical Research) Committee—Beaumont Hospital, Dublin, Ireland).
Neuropsychology
Neuropsychological testing assessed behavioural, executive, memory, letter fluency, attention, visio-spatial and language domains. Normal psychometric values were provided by a large cohort (n=110) of controls matched for age and education. The neuropsychological battery and neuropsychological control characterisation have been described previously.28 ,29 In timed tasks, where possible, performance was corrected for motor disability.30 Assessments were carried out at the patients’ home. Only patients with no evidence of cognitive or behavioural impairment on extensive neuropsychological testing were included in this study.
Neuroimaging
MR data were acquired on a 3 Tesla Philips Achieva (Best, The Netherlands) system with gradient strength 80 mT/m and slew rate 200 T/m/s using an eight-channel receive-only head coil. A three-dimensional inversion recovery prepared spoiled gradient recalled echo (IR-SPGR) sequence was used to obtain high resolution T1-weighted images of the brain with FOV=256×256×160 mm, spatial resolution=1 mm3, TR/TE=8.5/3.9 ms, TI=1060 ms, flip angle=8°, SENSE factor=1.5. FLAIR images were acquired in axial orientation using an inversion recovery turbo spin echo sequence: FOV=230×183×150 mm, spatial resolution=0.65×0.87×4 mm, 30 slices with 1 mm gap, TR/TE=11000/125 ms, TI=2800 ms, 120° refocusing pulse, with flow compensation and motion smoothing and a saturation slab covering the neck region. The FLAIR sequence was included in the imaging protocol to detect subjects with previous ischaemic cerebrovascular events. Based on this, one subject was excluded with an old left posterior parietal infarct.
Data analysis
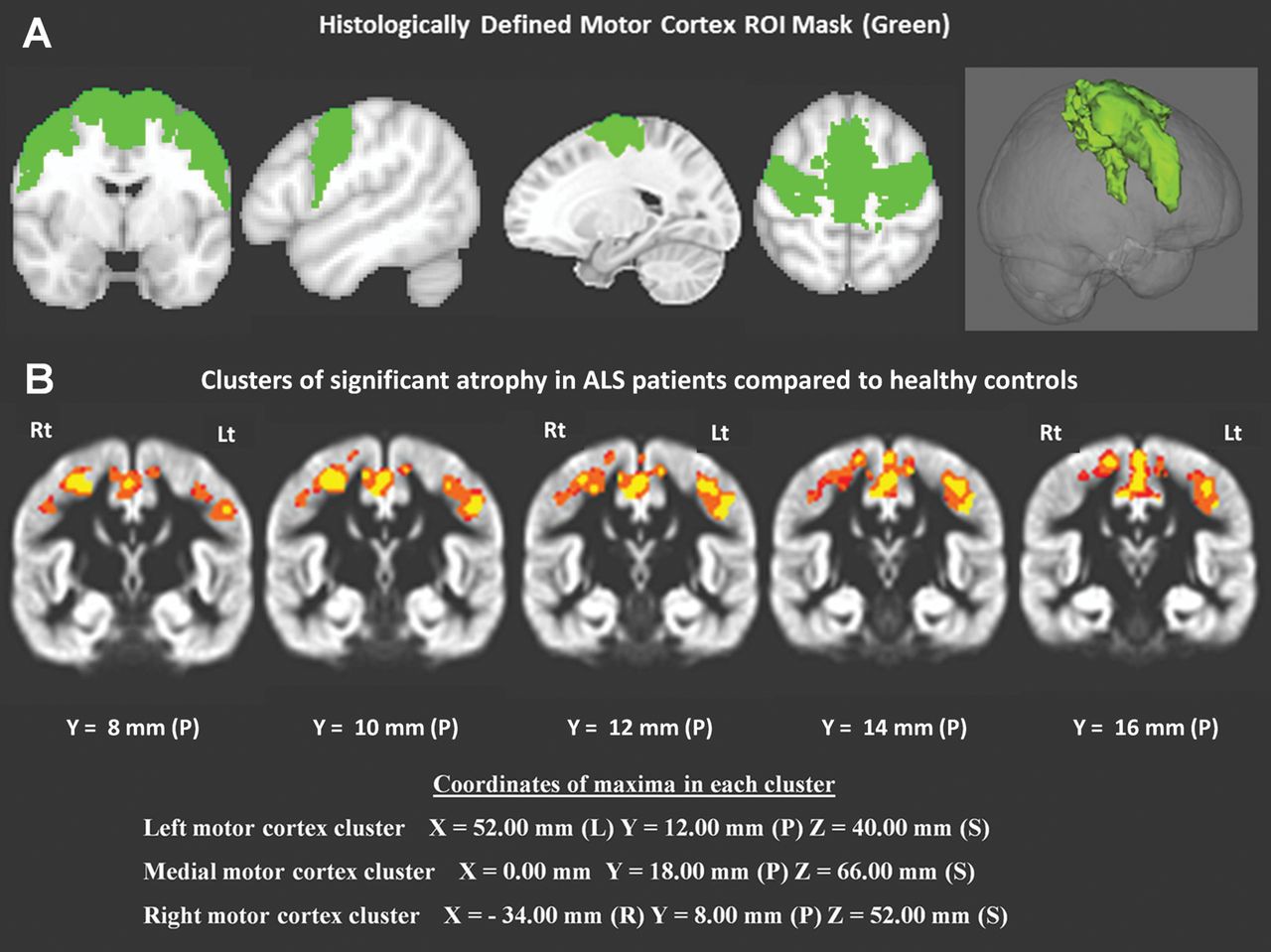
Voxel-based morphometry analysis31 was carried out with FSL32 comparing the patient groups and healthy controls. After brain extraction and tissue-type segmentation, the resulting grey matter partial volume images were aligned to Montreal Neurological Institute152 standard space using affine registration. A study-specific template was created for each analysis, to which the grey matter images from each subject were non-linearly coregistered. A voxel-wise generalised linear model was used to test for differences between groups using permutation-based non-parametric testing. The minimum cluster size was calculated for each analysis using a Monte Carlo simulation to obtain a statistical significance of p<0.05 (family-wise error) corrected for multiple comparisons. Based on the pathological hallmark of motor cortex involvement in ALS, a region of interest (ROI) was defined (see figure 1) consisting of the primary motor cortex (PMC) (BA4), premotor cortex and supplementary motor area (BA6). This a priori ROI was created by merging the Harvard–Oxford probabilistic atlas33 for the PMC and the Jülich histological atlas for the pre- and supplementary motor cortex.34

(A) Histologically defined motor cortex region of interest (ROI) mask (green). (B) Bilateral motor cortex atrophy (orange) in the group with amyotrophic lateral sclerosis (ALS) compared with the healthy controls (p<0.05 family-wise error). The highlighted clusters are projected onto the study-specific averaged grey matter map. The coordinates are with reference to the Montreal Neurological Institute (MNI) stereotactic template.
To highlight grey matter differences between patients with ALS and controls within this ROI, non-ROI voxels were zeroed. The voxel-level statistical significance was set at p<0.01 with a minimum cluster size of 520 µl, leading to a multiple-comparisons corrected statistical significance at p<0.05 (family-wise error).
The main objective was to investigate grey matter differences in the motor cortex between patients with bulbar and limb onset. The previously described motor mask ROI was used, and the non-ROI voxels were zeroed. The voxel level statistical significance of p<0.01 and a cluster size threshold of 500 µl led to a p value of <0.05 corrected for multiple comparisons using family-wise error.
The second objective was to identify the grey matter correlates of functional clinical measures in the ALS group. A permutation-based non-parametric35 approach was used to explore the relationship between clinical variables and grey matter volumes. Subscores and the overall ALSFRS-R score were not treated as independent variables and were not included in the same design matrix. The variables were analysed separately with FSL- Randomise V.2.1 controlling for age, gender and education.
Clinical variables included the total ALSFRS-R score (maximum score 48), bulbar scores (questions 1–3 of the ALSFRS on speech, salivation and swallowing; maximum score 12), upper limb scores (questions 4–6 of the ALSFRS on handwriting, cutting food/handling utensils and dressing/hygiene, maximum score 12) and interval from onset of symptoms to the date of MRI scan (months). The identified clusters were corrected for multiple comparisons within the motor mask ROI using a cluster size threshold of 520 µl, leading to a statistical significance of p<0.05. To underscore the linear association between clinical disability and focal atrophy, the grey matter volume signal of the clusters were plotted against the relevant functional scores of the patients.
To identify other regions of significant cortical atrophy outside the motor ROI, a whole-brain VBM was performed. The cluster size threshold was set at 800 µl and the statistical significance at p<0.01 (voxel level), leading to multiple-comparisons corrected statistical significance of p<0.05 (family-wise error). Volume signal values in the identified clusters were plotted to further illustrate the volume differences between patients with ALS and controls in these key regions.
Results
Thirty-three patients with ALS were recruited to this imaging study, who had no evidence of cognitive or behavioural dysfunction on detailed neuropsychological testing. Five patients with ALS were excluded from the study owing to comorbid behavioural variant frontotemporal dementia fulfilling the Lund-Manchester (Neary) Criteria. The demographic and clinical data of the patients and healthy controls are summarised in table 1.
Comparative grey matter analysis of patients with ALS versus healthy controls in the motor cortex
Similarly to previous studies,16 ,18 the ALS versus healthy controls analysis (see figure 1) confirmed significant bilateral PMC involvement, pathognomonic of ALS.
Comparative grey matter analysis between patients with bulbar onset versus those with limb onset in the motor cortex
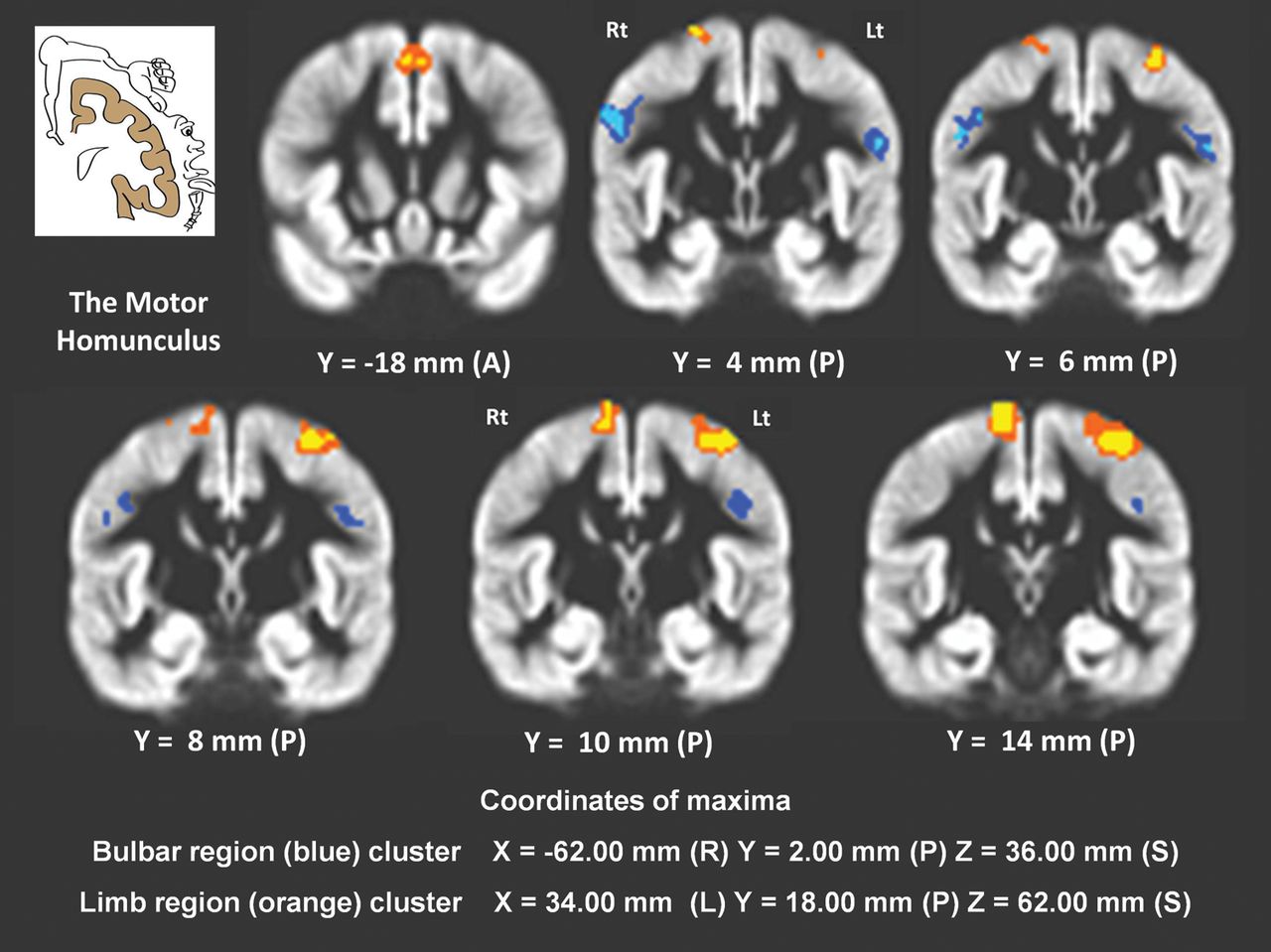
The 33 patients with ALS were divided according to site of onset, and comparative VBM analysis was performed between 13 patients with bulbar onset and 20 with limb onset. Age, handedness and education were similar in the two groups (see table 1). As shown in figure 2, the focal grey matter atrophy in the bilateral bulbar segment of the motor homunculus was significant in the patients with bulbar onset compared with those with limb onset. In contrast, patients with limb onset had a lower grey matter volume signal in the limb segments of the motor homunculus than patients with bulbar onset.

Focal atrophy of the motor homunculus, when comparing patients with bulbar onset amyotrophic lateral sclerosis (n=13) and those with limb onset (n=20). The blue colour indicates focal atrophy in patients with bulbar onset compared with those with limb onset, while the orange colour indicates focal atrophy in patients with limb onset compared with those with bulbar onset (p<0.05 family-wise error). The relevant clusters are overlaid onto the study-specific averaged grey matter map.
Linear association of clinical variables with regional grey matter atrophy
Validated clinical measures were used to determine whether grey matter volume is linearly associated with clinical variables. We focused on three key measures of motor disability: bulbar scores, upper limb scores and overall ALSFRS. We identified three distinct grey matter regions in the PMC where cortical volumes correlated with disability. The location of these clusters corresponded precisely with the classic functional representation of the motor homunculus (see figure 3). In addition, a PMC cluster was identified where the grey matter volume signal showed a negative linear association with disease duration.

Clusters where grey matter volume signal shows positive linear association with specific functional scores (red-yellow) and negative linear association with disease duration (blue). Clusters are displayed on the study specific averaged grey matter map. ALSFRS, Amyotrophic Lateral Sclerosis Functional Rating Scale.
The linear association between grey matter volume signal and clinical scores was further illustrated by plotting the clinical scores of individual patients against their grey matter volume signal in the relevant cluster of the motor cortex (see figure 4). As symmetrical bilateral bulbar clusters were identified, the left motor cortex cluster was used to demonstrate the correlation between bulbar scores and volume signal.
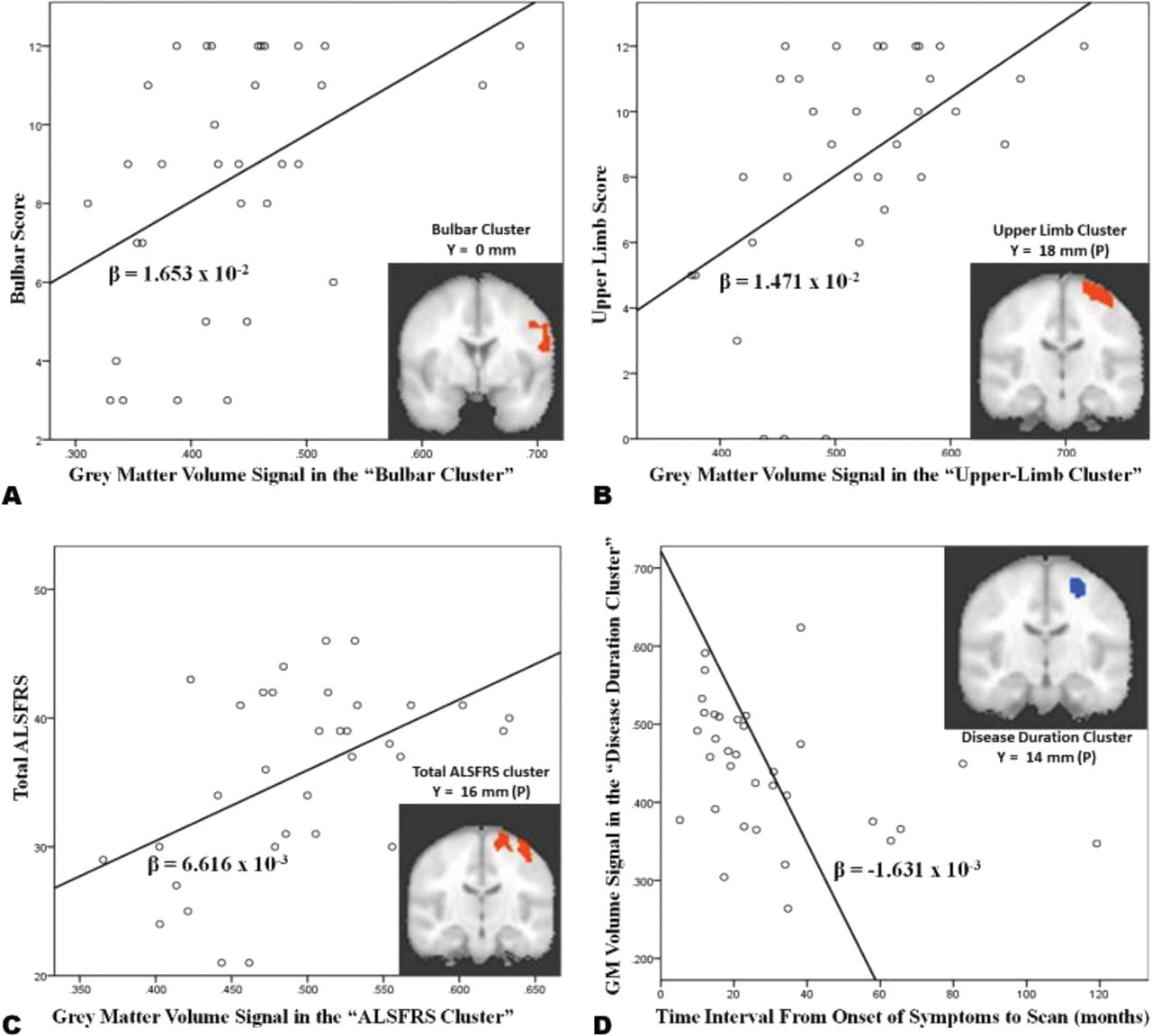
A,B,C: Positive linear association between functional scores and grey matter volume signal in the highlighted clusters D: Negative correlation between grey matter volume signal and disease duration. GM: Grey Matter, ALSFRS: Amyotrophic Lateral Sclerosis Functional Rating Scale Range: 0–48, Bulbar Score range: 0–12 Upper Limb Score range: 0–12, β-Beta regression coefficient. ALSFRS, Amyotrophic Lateral Sclerosis Functional Rating Scale.
Explorative grey matter analysis of patients with ALS compared with healthy controls in the entire brain
Group level comparison across the entire brain between patients with ALS and healthy controls revealed five distinct grey matter clusters. These clusters were located in the bilateral motor cortex, right occipital pole, the left inferior temporal lobe (parahippocampal region), the right superior temporal gyrus and the right superior frontal gyrus (see figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Regions of significant grey matter differences between ALS patients and healthy controls (p<0.05 family wise error). The distribution of the grey matter volume signal in each cluster is displayed in the boxplots for the two groups. The coordinates of the location of the maxima in each cluster are provided. ALS, amyotrophic lateral sclerosis; GM, grey matter; HC, healthy controls.
Discussion
This study was designed primarily to explore cortical changes within the motor cortex. Comparisons of patients with ALS and healthy controls and bulbar versus limb onset were performed. In a separate analysis, all patients with ALS were allocated to a single study group to investigate the imaging correlates of functional scores. Intentionally, simple, validated and commonly used clinical measures were chosen and correlation sought with basic structural T1-weighted imaging data.
The main finding of our study is the strikingly linear association between grey matter volumes in the PMC and well-established clinical measures of ALS. The locations of these clusters closely match the functional cortical representation of different body regions. The focal motor cortex grey matter differences between patients with limb onset and bulbar onset in the relevant regions of the motor homunculus further support the concept of ‘cortical focality’ in ALS as enunciated by Ravits and La Spada.6 The demonstrable relationship between relevant clinical variables and imaging findings in key regions of the motor strip suggests that neuroimaging could be useful as an objective measure of ALS disease burden, opening the possibility of imaging-based biomarkers in clinical trials.
One of the major challenges of biomarker development in ALS is the significant disease heterogeneity. ALS is now correctly regarded as a spectrum disorder of overlapping phenotypes. Disease heterogeneity in ALS has multiple dimensions, including genetic origin, site of onset,36 rate of decline, the presence of cognitive impairment and the relative degree of upper and lower motor neuron involvement.37 Several ALS imaging studies to date have compared clinically predefined ALS phenotypes such as ALS versus ALS-FTD.22 Such group-level comparative studies are often compromised by the artificial clinical criteria by which subjects are allocated to the different study groups, and are frequently driven by strong a priori assumptions. In our example, the limitation of allocating patients to bulbar onset and limb onset groups is that by the time the patient is scanned, patients with bulbar onset have a degree of limb involvement and vice versa. In our view, an alternative and more desirable approach in ALS imaging is to compile patients into a single study group, control for age, education, handedness, and explore which part of the brain is most linearly associated with a given clinical variable. Accordingly, we placed all patients into a single study group, and design matrices were created with the key clinical measures to explore the relevant cortical regions. This methodology allowed us to show the strong anatomical correlation between cortical volume loss and ALSFRS subscores.
There is now considerable imaging and neuropathological evidence of extra-motor cortex involvement in ALS. Early neuropsychological observations have been extensively validated by neuroimaging studies.38 Our findings of frontal, temporal and occipital regions in a large group of cognitively normal patients with ALS also support the concept of widespread extra-motor involvement in ALS. While the clinical implications of the non-motor aspects of the disease on survival,29 management and decision-making are well established, the pathological substrate underlying this multifocal involvement remains unclear. Neurodevelopmental factors39 and functional network associations40 have been implicated. Recent identification of the hexanucleotide repeat expansion in C9ORF72 of chromosome 9p41 ,42 and its clinical43 and pathological correlates44 suggests that patterns of extra-motor cortex atrophy are heterogeneous and are likely to be defined by complex genetic factors.45
One of the obvious limitations of the study is the use of ALSFRS-R and its subscores. ALSFRS-R is a clinically useful metric, a composite score reflecting both upper and lower motor neuron dysfunction. By its nature, it cannot be used as an accurate proxy for upper motor neuron markers. The use of more refined composite motor scores such as tapping speeds, spasticity scales and power measurements would be desirable, although such scales also have limitations. Additionally, it was not possible to investigate the structural correlates of respiratory scores, because in our sample low scores were not represented, the distribution of this variable was in a narrow range between 7 and 12. Thirdly, as our data are cross-sectional, the natural history of the disease has not been captured. Longitudinal data acquisition and analysis would provide further valuable insight into focal spread in the motor cortex.
In conclusion, we have demonstrated that the degree by which different body regions are affected in ALS corresponds to the degree of focal grey matter atrophy in the motor homunculus. Volumetric measurements of key cortical regions, such as the ones identified by this study, needs to be validated longitudinally. Our data, if confirmed, indicate that these analyses have the potential to provide an important objective measure of upper motor neuron disease burden.
References
Footnotes
-
Contributors PB: Conceptualization and design of the study, imaging data acquisition, analysis and interpretation, drafting and revision of the manuscript. AB: Conceptualization and design of the study, analysis and interpretation of the MRI data, revision of the manuscript for intellectual content. ME: Analysis and interpretation of neuropsychological data. SB: Interpretation of clinical and epidemiology data. RLM: Study design, optimization of MRI protocols. NJ: Analysis and interpretation of neuropsychological data. HH: Conceptualization of the study, revision of the manuscript for intellectual content. LG: Analysis and interpretation of neuropsychological data. CL: Acquisition of epidemiology data, maintenance of the Irish ALS register. AJF: Supervision of the biophysical aspects of the study, development and optimization of MRI protocols and sequences, revision of the manuscript. NP: Supervision of the neuropsychological aspects of the study, interpretation of the neuropsychological data, design of the neuropsychological battery. OH: Principal investigator, director of the Irish ALS Register and the Irish National ALS Clinic, conceptualization and design of the study, supervision of all clinical aspects of the study, drafting and revision of the manuscript. Statistical analysis was conducted by Peter Bede MD—Trinity College Institute of Neuroscience (TCIN), Trinity College Dublin, Ireland. All authors reviewed the manuscript before submission.
-
Funding This work was supported by the Health Research Board (HRB) grant number HPF/2009/17. The study is also sponsored by the Research Motor Neuron (RMN) foundation. The research leading to these results has received funding from the European Community's Seventh Framework Programme (FP7/2007-2013) under grant agreement n° (259867). AB's work is supported by Science Foundation Ireland (SFI) and he receives no commercial sponsorship. HH's research group is supported by the LOEWE excellence initiative, Neuronal Coordination Research Focus Frankfurt (NeFF), neurodegeneration branch, Alzheimer's disease project. OH's research group has received speaking honoraria from Janssen Cilag, Biogen Idec, Sanofi Aventis and Merck-Serono. HH has been a member of advisory panels for Biogen Idec, Allergen, Cytokinetics, Ono Pharmaceuticals and Sanofi Aventis.
-
Competing interests None.
-
Patient consent The manuscript does not contain personal medical information about an identifiable individual. Composite statistical results of complex neuroradiological data are presented, and no recognisable imaging is presented on any single individual.
-
Ethics approval Beaumont Hospital Ethics (Medical Research) Committee, Dublin, Ireland.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentaries