Article Text

Abstract
Background Behavioural disorders associated with compulsive use of dopaminergic drugs for Parkinson's disease (PD) such as dopamine dysregulation syndrome (DDS) and impulse control disorders (ICDs) may have devastating consequences and are challenging to manage. Whether or not such patients should undergo subthalamic nucleus (STN) deep brain stimulation (DBS) is controversial. A few case reports and small series have reported contrasting effects of STN DBS on dopamine misuse and ICDs, while a recent prospective study found clear beneficial effects of STN DBS on these disorders.
Methods We conducted an observational study on 110 consecutive parkinsonian patients scheduled for STN DBS surgery. Patients were assessed preoperatively through extensive behavioural and psychiatric evaluations and divided into two groups: with or without compulsive dopaminergic medication use. Evaluations were repeated 1 year after surgery in both groups.
Results Before surgery 18 patients (16.3%) were compulsive dopamine users of whom 12 (10.9%) fulfilled all criteria for DDS. 90% of these patients also had at least one ICD compared to 20% in the group without compulsive dopamine use. One year after surgery, one patient had persistent compulsive dopamine use, while no new occurrences were reported in the group without the condition before surgery. STN DBS did not provoke any major psychiatric complications and ICDs were reduced in all patients.
Conclusions Our results suggest that STN DBS may reduce compulsive use of dopaminergic medication and its behavioural consequences. Whether this improvement is the result of STN DBS or the consequence of better treatment management remains to be established.
- PARKINSON'S DISEASE
- STEREOTAXIC SURGERY
- MOVEMENT DISORDERS
- BEHAVIOURAL DISORDER
Statistics from Altmetric.com
Introduction
Patients with Parkinson's disease (PD) typically do not exhibit a predisposition to addictive and reward-seeking behaviours.1 However, a minority of PD patients develop compulsive behaviours that are triggered by dopaminergic drug therapy.2 In the past decade, these behaviours have been increasingly recognised and are divided into three main categories: (i) impulse control disorders (ICDs) such as pathological gambling, hypersexuality, compulsive shopping or binge eating3; (ii) punding, which is a stereotyped purposeless repetitive activity4; and (iii) compulsive use of dopaminergic drugs together with the dopaminergic dysregulation syndrome (DDS), where the addictive pattern of dopaminergic drug use is associated with behavioural disorders.5 ,6 Such behaviours may result in devastating psychosocial consequences and are therapeutic challenges for physicians. In particular, the therapeutic management of these patients is difficult, as long-term dopaminergic drug reduction is often incompatible with the maintenance of motor benefits.
Subthalamic nucleus (STN) deep brain stimulation (DBS), an effective therapy for treating disabled parkinsonian patients, improves motor impairment and reduces dopaminergic treatment with long-term efficacy.7 However, data regarding its effects on addictive and compulsive behaviours in PD remain controversial. Some authors have highlighted the deleterious effects of STN DBS on DDS and ICDs.8–11 Others have reported its efficacy in controlling these behavioural disorders, albeit in a limited number of patients.12 ,13 More recently, one case series and two studies have found mixed effects of STN DBS on DDS and ICDs,14–16 while one large study has reported positive effects of STN DBS on DDS and ICDs.6
The aim of this study was to determine the impact of STN DBS on compulsive dopaminergic medication use. To this end we divided PD patients scheduled for STN DBS into two groups according to the presence or absence of compulsive dopaminergic medication use. We compared the groups before and 1 year after surgery to examine the postoperative outcome of the compulsive use as well as the incidence of associated behavioural disorders and the possible occurrence of new compulsive behaviours in patients free from the disorder before surgery.
This study was based on preliminary observations of two patients with severe DDS showing a good outcome after STN DBS,13 and similar results in animal models of cocaine addiction.17
Methods
Patients
This was a prospective evaluation of patients with PD selected for STN DBS from January 2004 to August 2008 using the established criteria.18 All patients gave their written informed consent to the procedure and the study was approved by the local ethics committee. The primary objective was to evaluate the outcome of STN DBS in terms of compulsive dopaminergic medication use in a group of PD patients selected for surgery. The secondary objective was to evaluate the motor and non-motor outcomes of STN DBS, particularly the psychiatric co-morbidities associated with compulsive dopaminergic medication use.
Patients were divided into two groups: with or without compulsive dopaminergic medication use. Patients were included in the first group if they fulfilled the following criteria: rapid increase in dopaminergic drug dosage, automedication, inability to reduce dopaminergic drugs, marked ‘off’ dysphoria, and euphoria and hypomania in the ‘on’ state.5 They were considered as having DDS if in addition to having at least one ICD there were also socio-familial consequences to these behaviours, but those could reliably be assessed only with the caregiver when present.6
All patients were assessed both preoperatively and 12 months after surgery using the following motor, cognitive and psychiatric scales: the complete Unified Parkinson's Disease Rating Scale (UPDRS), Mattis Dementia Rating Scale, Verbal Fluency and Trail Making Test A and B, Beck Depression Inventory (BDI), Montgomery–Åsberg Depression Rating Scale (MADRS) and Hamilton Anxiety Rating Scale. Furthermore, a questionnaire on non-motor fluctuations was administered as reported previously.19 All psychiatric interviews were conducted by the same specialist trained in addictive disorders (JC). Behavioural disorders were prospectively assessed using the Minnesota Impulse Disorder Inventory (MIDI), Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria for substance misuse, binge eating and pathological gambling, and Giovannoni's criteria for DDS.5 Criteria for hypersexuality and excessive shopping were based on the MIDI and the interview.
All patients were scheduled to undergo operation within 6 months and were closely monitored during the pre- and postoperative period. Except in the case of new major motor or behavioural manifestations occurring between screening and surgery, the management of the patients and particularly of dopaminergic or psychotropic drugs was not modified. During this period clozapine was started in one patient who exhibited major behavioural disorders leading to his hospitalisation in a psychiatric ward. His condition subsequently improved and surgery was performed as scheduled.
Surgical procedure
The neurosurgical procedure was performed simultaneously on both sides of the brain as previously described.20 Briefly, MR imaging (Siemens Magneton Vision 1.5-T MRI scanner) was performed under stereotactic conditions with controlled anaesthesia to avoid any movement artefacts. The STN could be viewed directly on the T2-weighted spin-echo coronal images obtained perpendicular to the axial slices. Implantation of the electrodes was carried out under controlled anaesthesia using halogenated gas and alfentanil. This type of anaesthesia is compatible with the recording of STN and substantia nigra neuronal activity.20 Implantation of the stimulator (Kinetra; Medtronic Neurological Division, Minneapolis, USA) took place a few days after electrode implantation. The stimulation settings were adjusted at regular intervals after surgery as is routine in the department of Neurology and Movement Disorders. Patients were assessed 1 year postoperatively since this delay allows optimal adjustment of medication and stimulation settings.
Statistical analysis
Before statistical analysis, data were checked for outliers and the distribution of variables. Continuous data were expressed as mean±SD and relative change as mean (95% CI). The dopamine abuser group was compared to the non-abuser group using the Student t test or Mann–Whitney test (between-group). Preoperative and postoperative assessments were compared using a paired t test or a Wilcoxon signed rank test (within-group).
Categorical variables were presented as number (%) of patients. Between-group comparisons were carried out with the χ2 test and within-group comparisons with McNemar's test. The significance level was set at 0.05 (two-sided test). Statistical analyses were performed using SAS V.9.2 (SAS Institute Inc., Cary, North Carolina, USA).
Results
Preoperative assessment
Out of 110 patients selected for STN DBS, 18 (16.3%, 16 male) were compulsive dopaminergic medication users among whom 12 (10.9%) fulfilled the criteria for DDS. The clinical details of the two groups are summarised in table 1.
Preoperative characteristics of the patients in both groups
Dopaminergic misusers were significantly younger at surgery, had a more severe motor score during the ‘off’ state (p=0.028) and had higher L-dopa equivalent daily dose (LEDD) (p=0.010). There was no significant difference between the two groups regarding disease duration, motor fluctuations or dyskinesia.
All dopaminergic misusers reported non-motor fluctuations, in particular psychic fluctuations such as anxiety or depression in the ‘off’ state, and euphoria and/or hyperactivity in the ‘on’ state. Although 92% of the non-misusers also reported non-motor fluctuations in ‘off’, only 44% experienced non-motor fluctuations in ‘on’. The mean number of psychic fluctuations was 6 in ‘off’ and 2.4 in ‘on’ for dopaminergic misusers compared to 3.7 in ‘off’ and 1 in ‘on’ for non-misusers.
Dopaminergic misusers reported other substance misuse such as drug misuse (five patients, 28%; mostly cannabis but cocaine in one patient) and alcohol misuse (four patients, 22%), while no drug misuse was reported in non-misusers and only two (2%) had excessive alcohol consumption. Five dopaminergic misusers (28%) and five non-misusers (6%) were smokers.
Dopaminergic misusers reported significantly more ICDs such as pathological gambling (50%), hypersexuality (72.2%) or excessive shopping (38.9%), compared to non-misusers (table 2).
Frequency of behavioural disorders related to dopaminergic drug misuse in both dopamine misusers and non-misusers
The frequency of binge eating as well as punding was not statistically different in non-misusers compared to misusers, although there was a trend towards a higher rate in the latter group. When binge eating was removed from the analysis, nearly 90% of dopamine misusers had at least one ICD compared to 20% of non-misusers (figure 1). Half of the dopaminergic misusers reported walkabouts, a symptom that was less frequently reported in the other group. A history of manic psychosis (paranoid ideas, hallucinations) was reported in 11 dopaminergic misusers (61%) but in none of the group without dopaminergic misuse.
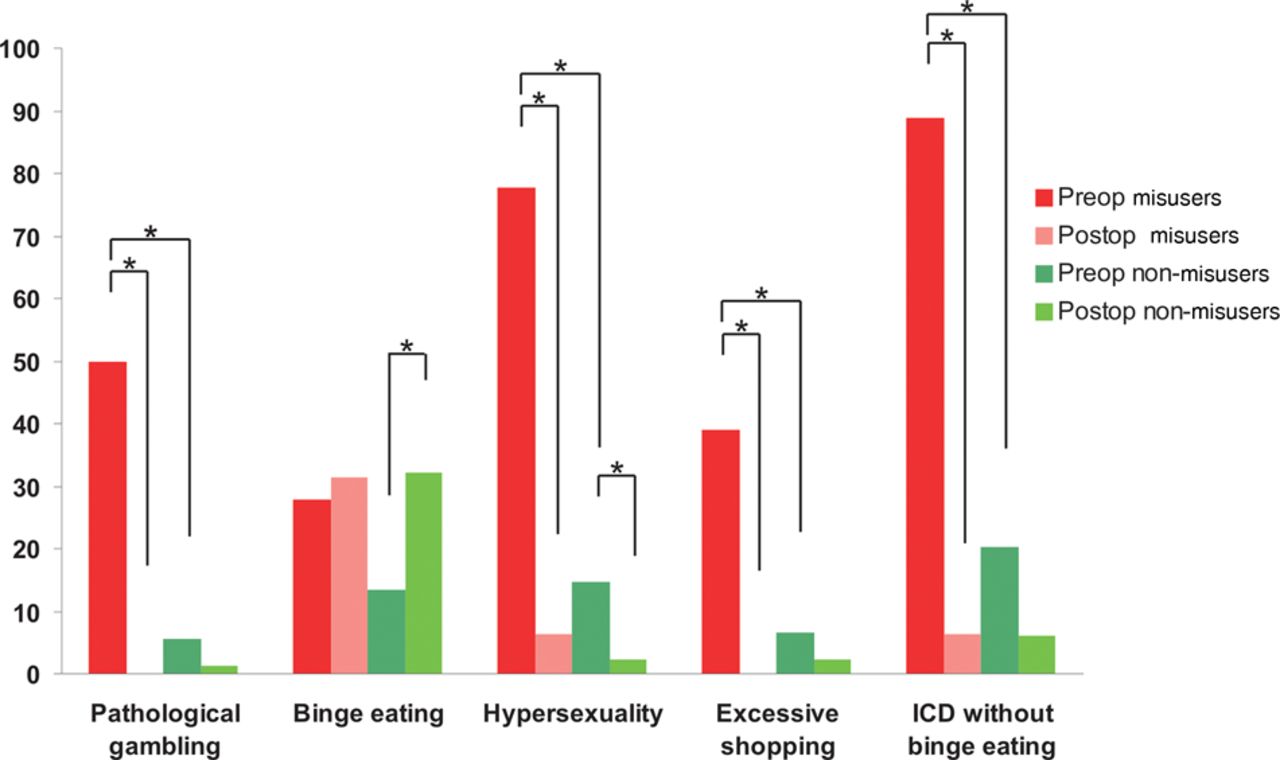
Pre- and 1-year postoperative frequency of impulse control disorders (ICDs) in dopamine misusers and non-misusers. The percentage of patients with pathological gambling, binge eating, hypersexuality, excessive shopping, or at least one of the above (binge eating excluded) are represented here. Note that in the misuser group n=18 preoperatively and n=16 postoperatively, while in the non-misuser group n=92 preoperatively and n=85 postoperatively. *p<0.05.
Postoperative assessment
All patients were implanted as scheduled bilaterally in the STN. Results at 1 year were available for 101 patients. Two patients in the dopamine misuse group were lost to follow-up before the end of the first year, while none was lost to follow-up in the non-DDS group. In the non-misusers group, two of the four patients (4.3%) who experienced an intraparenchymal haemorrhage died. One patient died before the 1-year assessment from aggressive pulmonary cancer. Two patients could not be assessed at 1 year because of temporary removal of the stimulator due to hardware infection. No patient in the dopamine misuse group experienced confusion postoperatively, while five patients in the group without dopamine misuse had transient confusion. In the latter group, one patient also experienced a pulmonary embolism and two patients had transitory cardiac insufficiency. No epileptic seizures were reported in either group.
Motor results
Motor improvements and reduction in LEDD are detailed in table 3. There was a significantly higher STN DBS-induced improvement in the motor score ‘off’ L-dopa in dopamine misusers compared to non-misusers (p=0.002). The decrease in LEDD was similar between groups when based on a percentage decrease with respect to the baseline dose (p=0.291). Similarly, the reduction in agonist dose was not different between groups (p=0.985). One patient with dopamine misuse and five non-misusers were able to completely stop their dopaminergic medication. In the dopamine misuse group, 13 patients were on L-dopa and dopamine agonists before surgery, six patients remained on the same drug combination, four patients were switched to L-dopa alone and one received no dopaminergic medication. For one patient who was on L-dopa alone before surgery, a dopamine agonist was added postoperatively because of the emergence of apathy.
Postoperative characteristics and change from preoperative values in both groups
In the non-misuser group, 75 patients were on L-dopa and dopamine agonists before surgery and 36 remained on the same drug combination after surgery. One patient was on dopamine agonist alone.
The stimulator settings were similar for both groups. The chosen contacts were no. 2 and no. 6 for 80% of patients. The mean stimulation intensity/pulse width was 3.1 V/62.3 µs for channel 1 and 2.9 V/64.6 µs for channel 2. The mean stimulation frequency was 137.3 Hz.
Behavioural results
Among the 16 patients with dopaminergic compulsive use assessed 1 year after surgery, only one patient had persistent overuse along with ‘on’ euphoria, ‘off’ dysphoria and still qualified as having DDS. In addition, two patients still experienced ‘off’ dysphoria and ‘on’ hypomania but without dopaminergic misuse. Both of these qualified as having DDS preoperatively. None of the 85 patients from the non-misuser group developed dopaminergic medication misuse postoperatively.
ICDs were analysed separately from binge eating (see below).
In the dopamine misuse group, none of the patients without ICD prior to surgery developed the condition after surgery. Pre-existing ICDs such as pathological gambling (n=9) and excessive shopping (n=7) completely resolved after surgery. Hypersexuality resolved in all (n=13) but the patient with persistent dopamine misuse and the net effect at the group level was a significant reduction after surgery (see figures 1 and 2 for significance levels).

{kind=link}
{kind=link}
Postoperative disappearance and occurrence of impulse control disorders in dopamine misusers and non-misusers. The percentage of patients with either preoperative pathological gambling, binge eating, hypersexuality, or excessive shopping whose ICD has disappeared postoperatively (disappearance) are represented here along with those who did not have any ICD prior to surgery and developed one postoperatively (occurrence). Note that in the misuser group n=18 preoperatively and n=16 postoperatively, while in the non-misuser group n=92 preoperatively and n=85 postoperatively. *p<0.05 (McNemar's test). NS, not significant.
In the non-misuser group, one patient who had no ICD preoperatively developed pathological gambling 6 months after surgery and two developed excessive shopping, all three after the introduction of low doses of dopamine agonists for apathy after surgery. Pre-existing ICDs such as pathological gambling (n=5) and excessive shopping (n=7) completely resolved after surgery. This led to a non-significant trend towards reduction in both gambling and shopping in the non-misuser group. Hypersexuality persisted in one patient postoperatively, developed in another patient and disappeared in 12 patients, leading to a significant net reduction after surgery (see figures 1 and 2 for significance levels).
Binge eating persisted after surgery in two dopamine misusers and developed in three others. In the non-misuser group, the number of patients with binge eating significantly increased after surgery (p=0.005) (figures 1 and 2). The weight gain after surgery was 2.6 kg (from 71.1 kg to 73.7 kg; p=0.037; Student t test) in the dopamine misuser group and 3.7 kg (from 69.7 kg to 73.4 kg; p=0.001; Student t test) in the non-misuser group. There was a non-significant trend towards a higher dosage of agonist LEDD in those patients who developed binge eating compared to those who did not in the non-misuser group only (157.5 mg vs 84.5 mg; p=0.07).
When binge eating was removed from the analysis, the percentage of patients with at least one ICD significantly decreased by 85% after surgery in the dopamine misuser group and by 70% in the non-misuser group.
There was a significant decrease in psychic non-motor fluctuations with less ‘off’ dysphoria and ‘on’ hypomania (p<0.002). The mean number of psychic fluctuations was reduced by 62% in ‘off’ and 90% in ‘on’ for dopamine misusers and by 84% in ‘off’ and 93% in ‘on’ for non-misusers. The patient with persistent DDS still experienced severe non-motor fluctuations and two patients whose dopamine misuse resolved postoperatively reported persistent psychic non-motor fluctuations although they were less severe. There was no significant difference in BDI and Mattis Dementia Rating Scale scores pre- and postoperatively or between the two groups (table 3).
Two patients with dopamine misuse still consumed cannabis after surgery. There was no illicit drug or excessive alcohol consumption in the non-misuser group. There was no change in smoking habits for either group.
Punding was less frequently reported after surgery in both groups but without reaching statistical significance (p=0.6). Walkabouts completely disappeared in the dopamine misuser group and only three patients reported this habit in the non-misuser group. No major psychiatric complications such as manic psychosis occurred during the follow-up of dopamine misusers. There were no suicide attempts in the group with dopamine misuse. In contrast, two non-misusers developed paranoid ideas and severe anxiety during the first year and one of them, who also had multiple ICDs, attempted suicide. Both of these patients had a history of major depression years before STN DBS. No significant modifications in BDI scores were found after surgery in either group.
Discussion
The outcome of STN stimulation in PD patients with dopaminergic medication compulsive use was hitherto mostly described in case series with mixed results. We conducted the largest prospective evaluation on 110 consecutive PD patients before and 1 year after STN DBS, comparing two groups of patients with and without dopaminergic medication compulsive use. The main result of this study is that compulsive and addictive behaviours were reduced in both groups 1 year after STN DBS.
Preoperative assessment
Compulsive use of dopaminergic medication and in particular DDS may be uncommon, but it has been reported to occur in up to 4% of PD patients.21 However, this prevalence is based on general PD population studies. Our study found that the prevalence of dopamine compulsive use and DDS among candidates for DBS was as high as 16.3% and 10.9%, respectively. As dopamine misuse occurs mainly in young patients with high LEDD and severe motor complications, and therefore overlapping selection criteria for STN DBS, candidates for surgery may represent a group of patients with a high prevalence of dopamine misuse.22 As usually described, dopamine misusers in our study were younger, with shorter disease duration and a lower ‘on’ motor score.5 Two recent studies have found a prevalence of DDS of 2.5% and 4% in a similar population, but in one the diagnostic criteria were applied retrospectively and in the second the prospective nature of the application of the criteria remains unclear.14 ,15 In contrast, a recent study with similar methodology to ours found a prevalence of compulsive dopaminergic medication use and DDS of 20.6% and 6.4%, respectively.6 Although dopamine misuse is more commonly reported in males, in our study the gender difference did not reach statistical significance between the groups perhaps because men are usually more prone to undergo DBS surgery than women, therefore introducing a bias.23 We found that dopamine misusers reported major psychic fluctuations with both ‘off’ dysphoria and ‘on’ euphoria and hypomania, while Evans and co-workers particularly highlighted the importance of ‘off’ symptoms.24 In the group without dopamine misuse, psychic fluctuations were less frequently reported (48% vs 94% for ‘off’ dysphoria and 27% vs 89% for ‘on’ euphoria) and were at comparable levels to those observed in a general pre-surgical PD population.19 Dopamine misuse was also associated with ICDs such as pathological gambling (50%), hypersexuality (72%) and excessive shopping (39%). In the group without dopamine misuse, these ICDs were found at levels similar to those in a general PD population.25 ,26 A recent study found that the prevalence of ICDs in a similar population could be as high as 34%.6 Binge eating was the only ICD that was found at comparable levels in both groups. Punding was also observed at comparable levels in both groups, which is not fully in agreement with previous studies describing DDS patients as having more punding than non-DDS patients.4 However, these discrepancies may be explained for the former by the difficulty in assessing eating disorders and for the latter by the rather broad definition of punding ranging from ritualistic sterile repetitive behaviours to hobbyism. In addition, the prevalence of punding in PD patients has proven extremely variable between studies.4 ,27
Effects of STN DBS on compulsive use of dopaminergic drugs
There is controversy over whether or not DDS patients should undergo STN DBS. Several authors reported cases with aggravation or even emergence of compulsive dopamine use after surgery.8–11 ,14 ,16 Our study shows that compulsive dopamine use is improved by STN chronic stimulation: dopamine misuse completely resolved after 1 year of STN DBS in 15 patients, while one patient still had abusive L-dopa consumption, therefore still fulfilling the criteria for DDS. However, it must be stressed that two patients with pre-existing DDS were lost to follow-up and their outcome at 1 year therefore could not be assessed. One recent study has found very similar results with complete resolution of dopaminergic compulsive medication use in 13/13 patients.6 In addition to the suppression of dopamine misuse following STN DBS, we did not observe any new occurrence of dopamine misuse in the patients free from the disorder preoperatively. This is in contrast with previous results from retrospective studies8 ,11 ,16 but in keeping with the above-mentioned study in which one patient developed compulsive dopamine use after surgery, but the electrodes were misplaced and therefore STN DBS was not completely successful.6
How do we reconcile the results of this study with the observations made earlier? First, most of these studies retrospectively analysed clinical data from multiples centres. Second, a critically important point is that the motor effect of STN DBS in our study and particularly in the dopamine misuser group was high. In fact, it was even higher than in the non-misuser group. This is important and may explain why some authors did not observe a significant improvement in DDS.11 ,14 ,16 In contrast, the study by Lhommee et al6 found complete resolution of dopamine misuse in line with a strong motor improvement after STN DBS with the exception of one patient with misplaced electrodes, and therefore inefficient STN DBS, who developed dopamine misuse postoperatively. However, it must be acknowledged that the motor score of the patient in our study whose DDS did not resolve after surgery was improved by STN DBS to a similar extent as in the rest of the dopamine compulsive users although he still experienced motor fluctuations postoperatively. This may suggest that although a significant motor effect of STN DBS is a prerequisite for dopamine misuse alleviation, it may not in itself suffice for its disappearance, which may be achieved by an additional effect of STN DBS on non-motor symptoms. Third, it is important to stress that the definition of compulsive dopaminergic use and DDS is not always the same in these studies and that the authors of these criteria stressed that milder forms with many of the features of the dysregulation can occur without the full syndrome developing.5
A similar picture was seen for ICDs which were reduced following STN DBS in both groups, except for binge eating which remained unchanged in dopamine misusers and significantly increased in non-misusers. The increase in binge eating in the non-misuser group is in line with a larger weight gain after surgery in that patient group (3.7 kg vs 2.6 kg). We believe that this result indicates that the definition of binge eating may not be entirely adequate and may encompass a large variety of complex eating disorders which may not all be impulsive.28
There is ongoing debate concerning the behavioural and psychiatric complications which may occur after STN DBS in DDS and ICD patients.12 ,13 ,29 In our study, there was no difference in depression scales in either group before and after surgery and no major psychiatric complications such as manic psychosis or attempted suicide during the follow-up of dopamine abusers patients in line with recent findings6 but in contrast with previous findings suggesting a higher suicide risk in that particular population.30
Study limitations
Our aim was to document the occurrence or disappearance of the compulsive use of dopaminergic drugs in PD patients following STN DBS. Therefore, we did not modify the strategy used in the department as regards medication and stimulation parameters. This means that the LEDD was reduced after surgery in both groups and that some patients had a different drug profile after surgery than before. However, we strongly believe that the possibility of reducing LEDD intake after surgery in dopamine compulsive users where previous attempts to do so have consistently failed, suggests a specific effect of STN DBS. Here dopamine misusers were able to reduce their LEDD intake at a similar magnitude as non-misusers.
Mechanisms of the effect of STN DBS on DDS
The basal ganglia are implicated at multiple levels, and in particular the STN, in reward-related processes.31 ,32 Several mechanisms may underlie the effect of STN DBS on the compulsive use of dopaminergic drugs and need not be mutually exclusive. First, there is evidence from animal studies to suggest a direct effect of both STN lesioning17 and DBS33 in reducing addictive behaviour, such as cocaine addiction. One of the hypotheses in this animal model is that the intervention on the STN reduces the rewarding properties of cocaine.33 Interestingly, most of the dopamine misusers in our study reported that they did not feel the same stimulating effect of L-dopa after surgery, some of them even reporting an aversion to dopaminergic drugs. Furthermore, in the above-mentioned animal study, STN DBS exerted opposite effects on eating behaviours with an increase in appetence for sucrose.33 This effect mirrors that observed in our patients where binge eating is either not reduced (in the misuser group) or further increased (in the non-misuser group) by STN DBS. Second, the reduction in the compulsive use of dopaminergic drugs may be secondary to the reduction in non-motor fluctuations and particularly those observed in the ‘on’ state.20
Conclusion
This study has shown that STN stimulation may significantly reduce the compulsive use of dopaminergic drugs in PD patients without significantly increasing the risk of inducing the disorder in previous non-misusers. In addition, most of the addictive behaviours improve after STN DBS partly as a result of the lower dosage of dopaminergic medication but also possibly through a specific effect of STN DBS in the limbic circuit of motivation and reward. There is ongoing debate over whether functional neurosurgery is a valid therapeutic strategy for drug addiction.34 Based on these results as well as on previous animal data, DBS may have a specific effect on dopamine addiction, thus paving the way for future studies in non-parkinsonian addicted patients.35
Acknowledgments
We would like to thank Marie Delfini for her help with the neuropsychological assessments. We are also indebted to Christelle Chabot for assisting in scheduling the visits and to Lydie Melas for assisting in the statistical analyses. Finally, we would like to thank Dr Starkman for revising the grammar and the English.
References
Footnotes
-
AE and TW contributed equally.
-
Contributors TW and JPA designed the study; AE, TW and JPA secured funding; AE, TW, JPA and FF assessed the patients; JC performed the psychiatric interviews; JR operated on the patients; EJ performed the statistical analyses; and AE and TW wrote the paper.
-
Funding This study was funded by a grant from the Agence Nationale de la Recherche, France (ANR-09-MNPS-028-01).
-
Competing interests None.
-
Ethics approval CCPRB Marseille approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.